Detection of Extravascular Trypanosoma Parasites by Fine Needle Aspiration
In This Article
Summary
Fine Needle Aspiration is a technique, whereby cells are obtained from a lesion or organ using a thin needle. Aspirated material is smeared, stained and examined under a microscope for diagnosis or used for molecular biology, cytometry or in vitro analysis. It is cheap, simple, quick and causes minimal trauma.
Abstract
Fine Needle Aspiration (FNA) is a routine diagnostic procedure essential to both medical and veterinary practices. It consists of the percutaneous aspiration of cells and/or microorganisms from palpable masses, organs or effusions (fluid accumulation in a body cavity) using a thin needle similar to the regular needle used for the venous puncture. The material collected by FNA is in general highly cellular, and the retrieved aspirate is then smeared, air dried, wet-fixed, stained and observed under a microscope. In the clinical context, FNA is an important diagnostic tool that serves as a guide to the appropriate therapeutic management. Because it is simple, fast, minimally invasive and requires limited investment in the laboratory and human resources, it is extensively used by veterinary practitioners, mostly in domestic, but also in farm animals. In studies using animal models, FNA has the advantage that it can be performed repeatedly in the same animal, enabling longitudinal studies through the collection of cells from tumors and organs/tissues over the course of the disease. In addition to routine microscopy, retrieved material can also be used for immunocytochemistry, electron microscopy, biochemical analysis, flow cytometry, molecular biology or in vitro assays. FNA has been used to identify the protozoan parasite Trypanosoma brucei in the gonads of infected mice, opening the possibility for a future diagnosis in cattle.
Introduction
Fine Needle Aspiration (FNA) is widely used in the diagnosis of cancer and non-neoplastic diseases, both in human and domestic animals. The technique has been standardized over the years and is described in numerous textbooks1,2.
It largely consists of the percutaneous aspiration of palpable masses, organs or effusions with a thin needle fitted onto an empty syringe, using the negative pressure to withdraw cells or fluid from the mass1,3. Needles are typically 22 to 25 G (gauge corresponding to the needle inner diameter), and the use of a larger bore needle (large diameter, e.g., 21 G) is helpful to increase the cellularity, although this can produce excessive blood contamination. Needle length will depend on the depth of the mass but 1 or 1½ inch is commonly used for superficial masses. Syringes are typically 5 to 10 mL, with larger syringes achieving higher vacuum, which in turn increases aspirate yield. Non-palpable deep-seated masses can also be aspirated, with longer needles and under image guidance (ultrasonography). The retrieved aspirate can then be smeared, air dried, wet-fixed, stained and observed under a microscope to achieve a diagnosis3 (Figure 1).
This is a simple, inexpensive, painless and minimally invasive technique mainly used in the preoperative setting to achieve a diagnosis on palpable masses and also for organs, like lymph nodes, thyroid, prostate or even the external male reproductive structures1. In addition to being a diagnostic tool, this technique can be used for the collection of cells for other purposes as well, namely cytogenetics, electron microscopy (Figure 1D), flow cytometric characterization4,5,6,7, establishment of cell cultures8. A common example in clinical practice is sperm retrieval for in vitro fertilization9.
Aspiration can be repeated several times in the same mass to obtain multiple smears. In case of a heterogeneous lesion, e.g., a solid area and a cystic space, it is important that cells are aspirated from each region. The material collected by FNA is in general highly cellular, which in most cases allows for the diagnosis of diseases without the need for a tissue biopsy. Special stains, immunofluorescence. immunocytochemistry (Figure 1D), and molecular techniques may also be performed in smears obtained through FNA, e.g., for the identification of infectious agents when not recognizable by morphology alone10. A brief overview of the general applications and of the equipment and supplies needed for FNA are summarized in Tables 1 and 2, respectively.
The first report on the use of the needle puncture for diagnostic purposes is described in early writings of Arab medicine, but it’s in the early 20th century that modern needle aspiration techniques were implemented11. Notably, perhaps the first report that suggests the use of FNA for the diagnosis of infectious diseases was a study in 1904, where Grieg and Gray reported needle aspirations of lymph nodes from patients with sleeping sickness revealed motile trypanosomes12. The authors reported the presence of trypanosomes in both early and advanced cases, and at a higher density than that seen in blood smears, where these are often rare events12.
Current diagnosis of Trypanosomiasis in cattle relies on the direct observation of parasites in the blood, lymph or in immunodiagnostic techniques13,14,15. We have previously shown that in experimental Trypanosoma infections in the mouse, Trypanosoma brucei (T. brucei) has a remarkable tropism to adipose tissue16 and also to some of the external male reproductive structures, namely epididymis17. Parasites accumulate in the stroma of these tissues in large numbers16.
The protocol depicted below describes a detailed step-by-step technical procedure for FNA in live mice, aimed at the aspiration of trypanosomes present in the external male reproductive structures (testis, epididymis, and epididymal fat), followed by conventional cytology and immunostaining for specific parasite proteins (VSG)16,17. Aspiration was performed 6 days after the infection and safety procedures that apply are those commonly established for routine handling of experimental animals. Additional measures are required for animals that have immune deficiencies (wearing a steam-sterilized gown, mask, hair bonnet, sterile gloves, and ensuring aseptic technique at all times) to mitigate accidental exposure to opportunistic pathogens.
Protocol
All animal experiments in this protocol were performed according to EU regulations and approved by the Animal Ethics Committee of Instituto de Medicina Molecular (iMM), (AEC_2011_006_LF_TBrucei_IMM). The animal facility of iMM complies with the Portuguese law for the use of laboratory animals (Decree-Law 113/2013) and follows the European Directive 2010/63/EU and the FELASA (Federation of European Laboratory Animal Science Associations) guidelines and recommendations concerning laboratory animal welfare.
1. Aspiration of Parasites from the External Male Reproductive Organs of the Mouse
NOTE: Fine needle aspiration (FNA) was performed in wild-type male C57BL/6J mice, 6 to 10 weeks old, infected with T. brucei through intraperitoneal injection of 200 µL of saline with 2,000 parasites as described previously16.
- For FNA of the external male reproductive organs, place the mouse in a laminar flow hood, anesthetize the animal with an intraperitoneal injection of 200 µL of a mixture of 75 mg/kg Ketamine + 1 mg/kg Medetomidine in saline.
- Confirm anesthetization with the toe pinch method. When the reflex of the retraction of the leg is absent, position mouse in dorsal recumbency (Figure 2A).
- Carefully palpate the testis, assessing size and distance from the overlying skin. Restrain the organ between the index and middle finger or between the index finger and thumb. Stretch the overlying skin tightly across the mass to further immobilize the target. Clean the surface with alcohol wipes (Figure 2A).
- Hold the assembled 22 G needle and 5 mL syringe and insert the needle tip into the target, always with the plunger in the rest state (Figure 2B-C).
- Apply suction by retracting the syringe plunger to the 4 mL to 5 mL mark 2-3 times. Redirect the needle within the organ either in a straight line or along several different tangents to increase the probability of a representative sample and of targeting smaller structures like the epididymis. Make sure that this procedure is gentle, to minimize the tissue damage (Figure 2C-D).
- Release the suction and then withdraw the needle. Do not redraw the needle with the retracted plunger as this will lead to the suction of the aspirate into the barrel of the syringe and impede its recovery (Figure 2E). After the withdrawal of the needle, control any bleeding by applying pressure with a sterilized gauze sponge at the puncture site.
- Disconnect the syringe from the needle, fill it with air, reconnect the needle and gently eject the contents of the needle onto a slide. Place the tip of the needle very close or even on the slide to avoid splattering (Figure 2F-I).
- Perform at least one additional aspiration per organ/animal to ensure replicate sampling.
- Revert anesthesia with a subcutaneous injection of 200 µL of 1 mg/kg Atipamezole in saline and return animals to their home cage for recovery and observe until full recovery.
2. Smear Preparation from the Aspirated Material
NOTE: Use gloves throughout the procedure and ensure safe disposal of needles and syringes.
- Two steps pull method
- Pick up the slide that has the drop of the aspirate using the nondominant hand, and pinch the frosted end between the thumb and index finger (Figure 3A).
- Pick up a second clean slide, the spreader slide, with the dominant hand and bring it across the first slide with the drop of the aspirate. Place the smooth clean edge of the slide on the specimen slide just on the top of the drop at an angle of approximately 30° (Figure 3B).
- Glide the slide forward with one light, continuous and steady movement to obtain a thin film (Figure 3C).
- Rest the slide and allow for the complete and fast air drying of the material (Figure 3D). Do not heat-fix. Label the frosted edge of the slide with a pencil.
NOTE: The protocol can be paused at this step and smears can be stored indefinitely until ready to be stained.
3. Staining of the Smears
NOTE: Use gloves throughout the procedure and ensure that steps 3.1.4 and 3.2.9 are performed inside a fume hood.
- Giemsa staining protocol
- Fix air-dried smears by immersing the slides into a Coplin jar containing 100% methanol for 5 min (Figure 3E).
- Transfer the slide into a Coplin jar containing 20% Giemsa solution (diluted to 1/5 in distilled water) for 30 min, or 10% Giemsa for 10 min (Figure 3F).
- Rinse off in tap water and dry thoroughly using tissue paper to dab.
- Hold the slide horizontally and apply one drop of the non-aqueous mounting medium onto the smear. Place the edge of a cover-glass onto the slide, lower it and press gently to remove any air bubbles.
- Immunocytochemistry in FNA smears
- Fix air-dried smears in 100% methanol at room temperature for 10 min.
- Wash the slide for 5 min in a Coplin jar with 1x phosphate buffer (PBS), repeating this step 3 times using fresh 1x PBS every time.
- Remove the slide from Coplin jar, wipe excess buffer without touching the smear and draw a circle around the smear with a water repellent pen (Table of Materials).
- Hold the slide horizontally and apply 150 μL of diluted primary antibody solution to each smear and incubate for 1 h at room temperature.
NOTE: Primary antibody used here is a non-purified rabbit serum anti-T. brucei VSG13 antigen (cross-reactive with many T. brucei VSGs, produced in-house), diluted in 1x PBS at 1:50,000. Perform negative controls by replacing the appropriate primary antibody with preimmune serum (Table of Materials) to allow for the assessment of the non-specific binding of the secondary antibody. - Wash the slide for 5 min in a Coplin jar with 1x PBS, repeating this step 3 times using fresh 1x PBS every time.
- Hold the slide horizontally and apply 150 μL of commercially available horseradish peroxidase/DAB visualization system to each smear. Incubate for 30 min at room temperature (Table of Materials).
- Wash for 3x for 5 min in 1x PBS.
- Counterstain by immersing the slides into a Coplin jar containing Harris hematoxylin. Rinse off in tap water and dry thoroughly using paper to dab.
- Hold the slide horizontally and apply one drop of the non-aqueous mounting medium onto the smear. Place the edge of a cover-glass onto the slide, lower it and press gently to remove any air bubbles.
Representative Results
FNA was performed in the external male reproductive organs of mice infected with T. brucei using a 22 G needle coupled to a 5 mL syringe, and glass slides for the smear preparation (Figure 1A-C). The method is simple but optimal results rely on critical steps: perfect immobilization of the mouse achieved through general anesthesia, and stabilization of the organs throughout the whole procedure (Figure 2A-B). Suction was applied 2-3 times and needle redirected 1-2 times to allow for representative sampling of the smaller organs and tissues: epididymis and epididymal fat. Negative pressure was released prior to externalizing the needle. The aspirate contained in the lumen and hub of the needle (approximately 20 µL), was used to produce 2 smears (Figure 3A-C). In cases where the needle was withdrawn without the release of the suction, the material was sucked into the syringe and was not recoverable. The process was successfully repeated twice, one for each paired organ. After drying, smears were wet-fixed and immunocytochemistry for the trypanosome surface proteins was performed.
A good quality smear (Figure 4A-C) was characterized by a monolayer of cells with good cellular density, in which host cells show preserved morphological features, allowing for the identification of their tissue of origin and relative proportion between one another. Parasites were efficiently immuno-stained, identifiable and countable (Figure 4B). One case of an FNA of a peritoneal effusion in an infected mouse, stained with Giemsa for direct observation and diagnosis, is also shown (Figure 3D-F and Figure 4C).
A poor or negative FNA result may be due to different reasons: (1) too little FNA material is expressed onto the slide and is under-representative of the sample; (2) too much FNA material is expressed onto a single slide, making overly thick smears and impairing cytological evaluation; (3) too much force is applied when making the smear, and cells are disrupted, resulting in a lot of naked nuclei and DNA streaks (crush artifact); or (4) not enough force is applied when making the smear and cells do not disaggregate, resulting in a stratified layer that impedes evaluation of the morphological features of the cells (Figure 5).
When we compare FNA cytopathology with histopathology, i.e., the analysis of cells versus tissues, the fist has the advantage that cellular morphology is better preserved and relative proportions and counting of cells can be better assessed (Figure 6). Furthermore, immunocytochemistry is simpler, faster and easier to optimize than immunohistochemistry, which is typically performed in formalin-fixed and paraffin-embedded tissue.
| Target | Applications | Advantages | Limitations |
| Palpable mass | Routine microscopy, diagnosis | Simple, quick | No tissue architecture |
| Organ | Immunohistochemistry | Low cost | Blind aspiration (needle may miss target tangentially; aspiration may target necrotic, cystic or hemorrhagic areas) |
| Effusions | Flow cytometry | Sampling from multiple sites | |
| Cytogenetics | Well-preserved cellular morphology | ||
| Electron microscopy | Free of complications | ||
| PCR, other molecular techniques | High diagnostic accuracy | ||
| Biochemical analysis | Anesthesia (for immobilization) | ||
| In vitro assays, cell culture | Non-terminal procedure |
Table 1: Target, general applications, advantages and limitation of fine needle aspiration.
| FNA Kit | Archetype of an aspiration needle and syringe |
| Aspiration: | Needle parts: |
| 1. Disposable plastic syringes (5 or 10 mL) (Figure 1B) | Bevel. Tip of the needle shaft is slanted to form a point, the slant being the bevel. Only beveled needles are suitable for percutaneous aspirations. |
| 3. Needles of 22 to 25-gauge (diameter); 0.75, 1.0, 1.5 inches long, with standard beveled needle tip edge (Figure 1A) | Shaft. Hollow tubular portion of the needle whose length may be adjusted according to the depth of the mass. The gauge of the needle corresponds to the diameter of its bore, which is the diameter of the inside of the shaft (smaller needles have higher gauge). The use of larger bore needles (less than 22 G) is helpful to increase the cellularity, although this can produce excessive iatrogenic blood contamination. |
| 1. Anesthesia (if necessary). Pain associated with FNA is similar to that of a venous puncture, however, good aspiration requires good immobilization of the subject, specially important in small-sized animals and/or for small, fluctuant lesions and organs. Rats and mice subject to FNA should be appropriately passively restrained, or, when necessary, sedated or be under light general anesthesia. | Hub. Plastic portion of the needle that is attached to the syringe; should be transparent to allow for the visualization of the aspirated material. The aspirate material obtained during FNA should be collected in the needle shaft and the aspiration stopped when material is seen entering the hub. |
| FNA smear making and interpretation: | Syringe parts: |
| 1. Frosted end glass microscope slides (Figure 1C) | Barrel/cylinder. Hollow portion of the syringe. Unless dealing with cystic lesions or effusions, material that is aspirated to the barrel generally cannot be recovered. Ideal volume of aspirate for FNA cytology is approximately 5 μL, corresponding to the average volume of aspirate that occupies the shaft and hub of the needle. |
| 2. Romanowsky type stains (e.g. Diff-Quik, Giemsa) | Tip. End of the barrel to which the needle hub is attached. |
| 3. Microscope (bright-field) | Plunger. Movable portion of the syringe that has a flat disk or lip at one end and a rubber seal at the other end. Fits into the barrel and provides the pressure to draw the cells, fluid into the needle. A perfectly sealed plunger that creates good negative pressure is obligatory to obtain a good aspirate yield. |
Table 2: Equipment and supplies needed for fine needle aspiration.

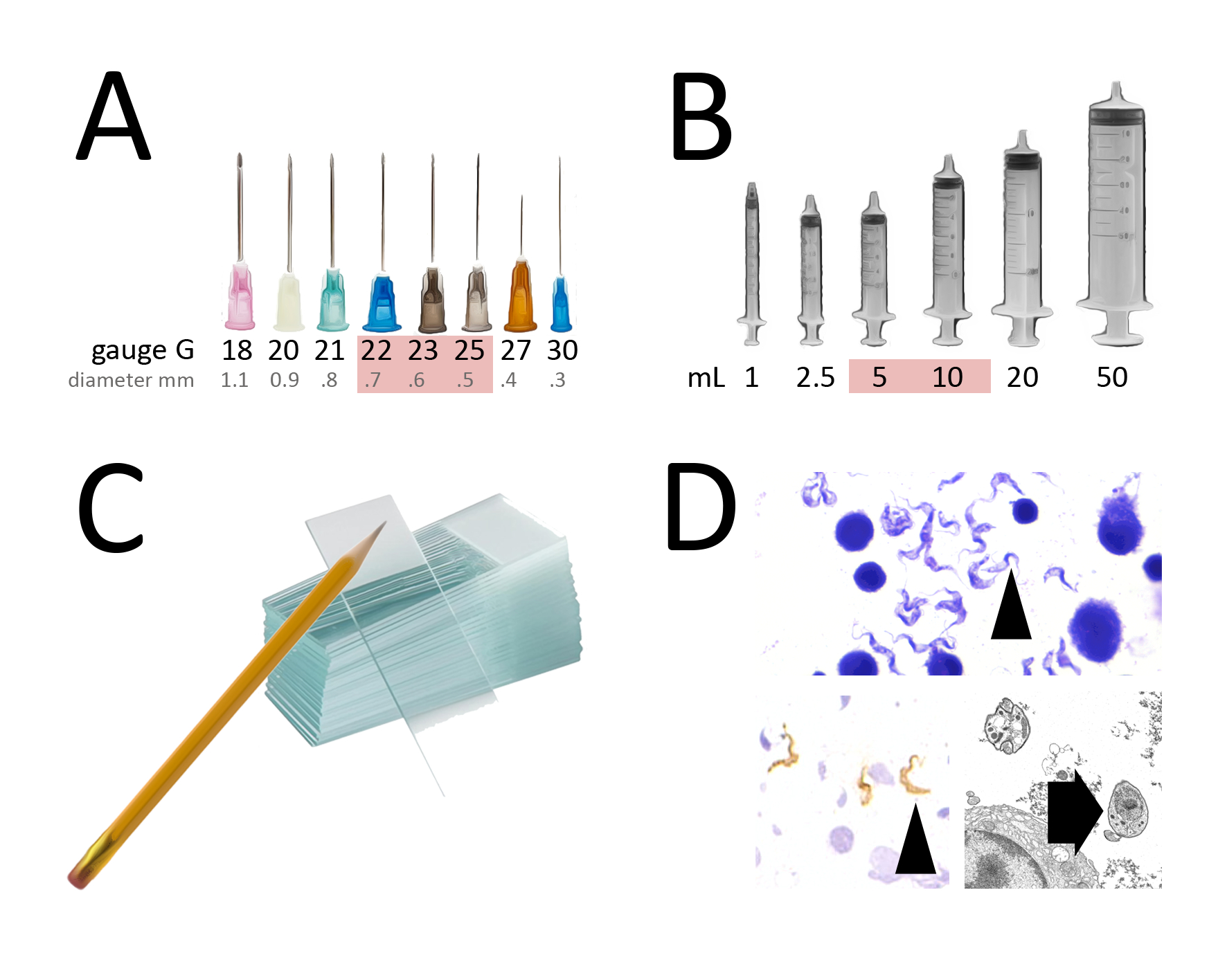
Figure 1: Tools and results for fine needle aspiration. (A) Ideal diameter of the needle for FNA is from 22 to 25 G. (B) Ideal syringe volume to obtain a good aspirate yield is of 5 to 10 mL. (C) Clean, dry, free of grease glass slide with frosted marking area for writing with pencil and pre-coated (if for immunohistochemistry). (D) Example of Trypanosomes observed with Giemsa staining (black arrowhead), immunostained for the VSG surface proteins (white arrowhead) and under transmission electron microscopy (block arrow). Please click here to view a larger version of this figure.
{kind=link}

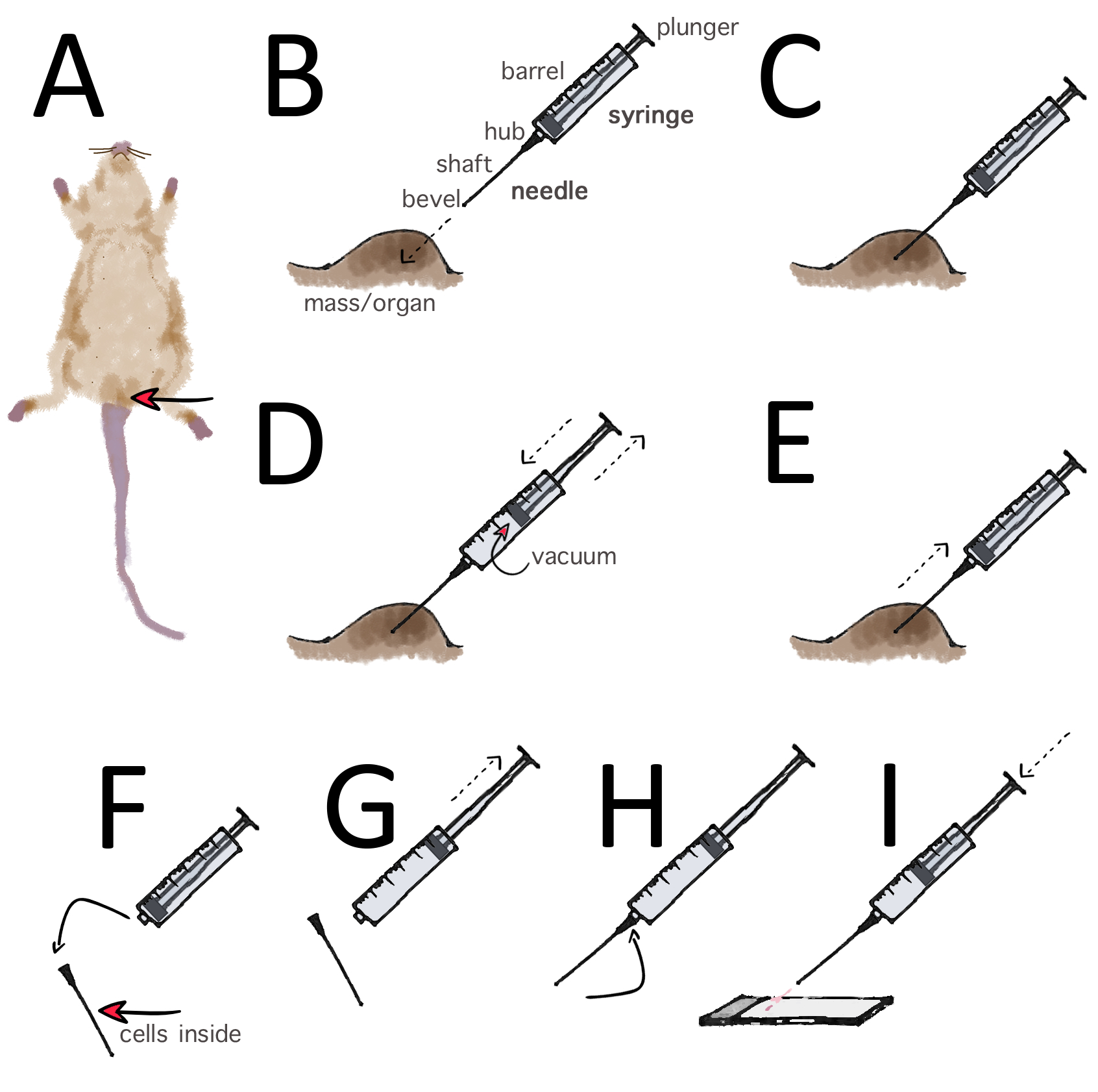
Figure 2: Schematics showing fine needle aspiration (FNA) of the external male reproductive organs (testis, epididymis, and epididymal fat) in mice. (A) Once the animal is secured, the previously assembled aspiration instrument is picked up. (B-C) Insert the needle tip into the target organ. (D) Apply the suction by retracting the syringe plunger to the 1 mL to 2 mL mark, repeatedly 3-4 times. Needle tip can also be moved back and forth within the target while applying suction, to collect sufficient material. (E) Release the suction and only then withdraw the needle. (F) Remove the needle from the syringe and (G) Pull the plunger back. (H) Reattach the needle. (I) Expel the material onto a glass slide by pushing the plunger swiftly through the syringe. In order to avoid splattering, ensure that the tip of the needle rest very close or even on the slide. The drop of aspirate is placed approximately 1 cm from the edge of the frosted marking area. Please click here to view a larger version of this figure.
{kind=link}

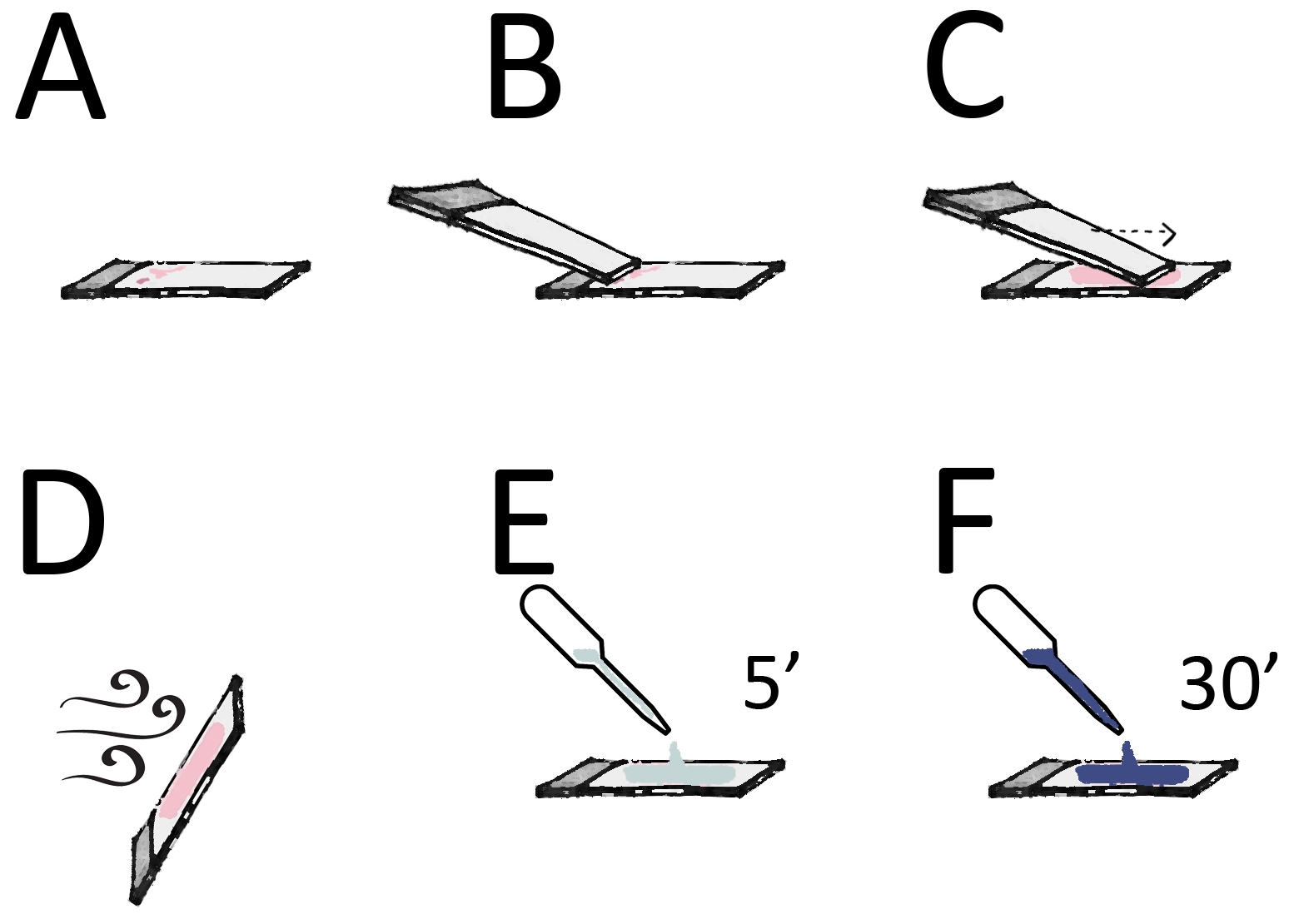
Figure 3: Smear preparation and staining. (A) Hold one end of the slide (frosted area) between the thumb and index finger. (B) Place the smooth clean edge of a second slide (spreader) on the specimen slide just in front of the drop of material. (C) Slide the spread forward once with moderate speed to obtain a thin film. (D) Allow the slide to air dry and label the frosted edge of the slide with a pencil. (E) After complete drying fix with methanol for 5 min. (F) Stain with 20% Giemsa solution for 30 min (or 10% Giemsa for 10 min). Lightly rinse with water, dry completely, dip in xylene, and mounted with a water-insoluble mounting agent. Please click here to view a larger version of this figure.
{kind=link}

Figure 4: Microphotographs of smears obtained from FNA of external male reproductive structures in mice infected with T. brucei. (A) Gross appearance of a good quality direct smear: the material was expressed onto the slide approximately 1 cm away from the frosted edge (black dot), smeared and stopped 0.5 cm before the edge of the slide (parallel lines). (B) Immunocytochemistry for the surface proteins of the parasite (VSG) was performed for smears obtained from FNA of the external male reproductive organs on the day 6 of infection. Numerous parasites (arrowhead) were detected admixed with mouse germ cells (arrow). DAB counterstained with Harris hematoxylin. Original magnification: 40x (Scale bar = 50 μm). (C) Giemsa-staining of the smear obtained after FNA of a peritoneal effusion on day 21 of the infection, showed numerous parasites (arrowhead) admixed with host (mouse) cells, in this case inflammatory cells, macrophages (arrow) and lymphocytes. Original magnification: 40x (Scale bar = 50 μm). Please click here to view a larger version of this figure.
{kind=link}

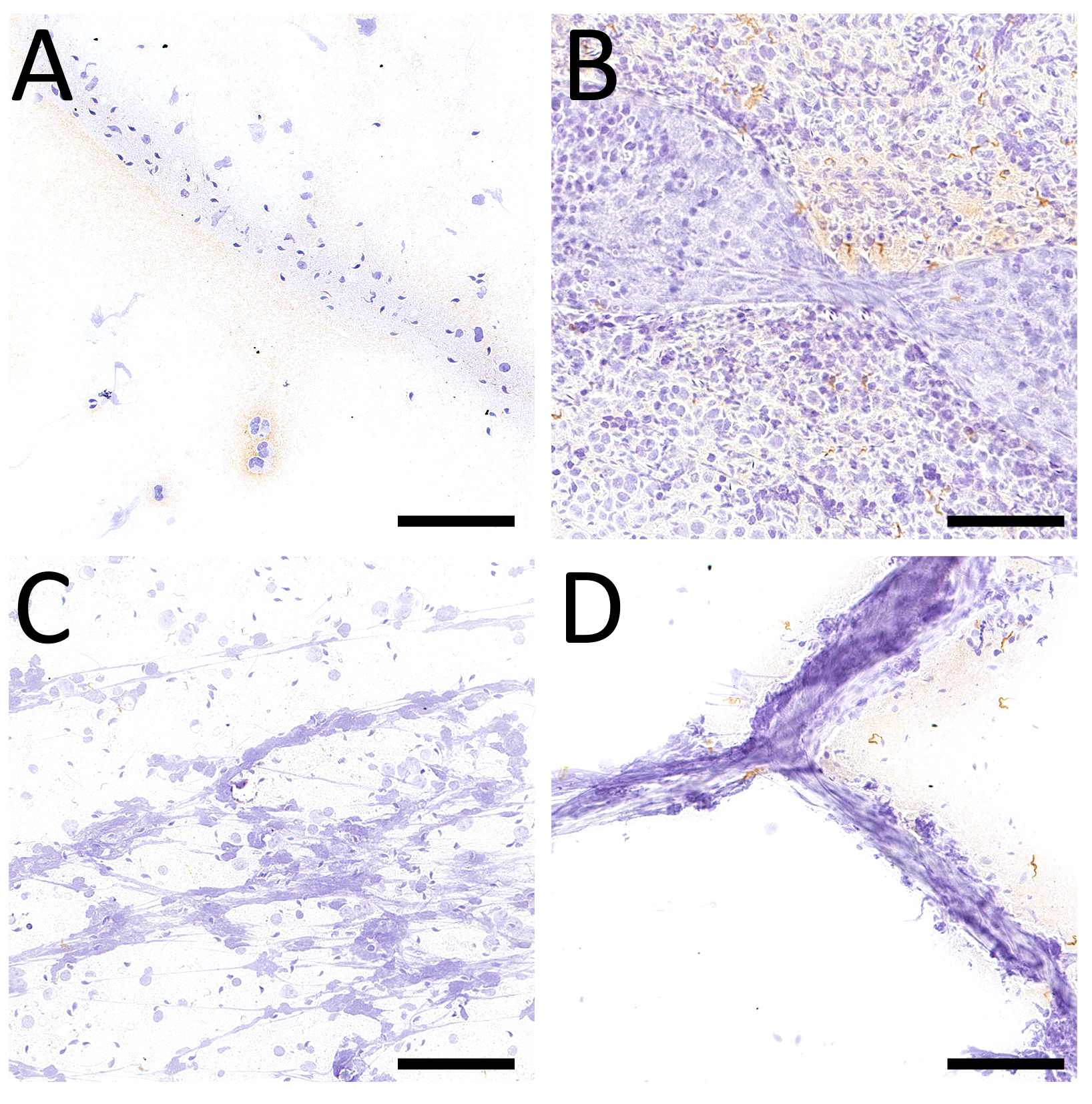
Figure 5: Poor quality FNA smears. (A) Poorly cellular smear, under-representative of the mass or organ. (B) Very thick smear. (C) Crushed artifact, with disrupted cells, naked nuclei and DNA streaks. (D) Aggregates and stratified layers of cells. DAB counterstained with Harris hematoxylin. Original magnification: 20x (Scale bar = 100 μm). Please click here to view a larger version of this figure.
{kind=link}

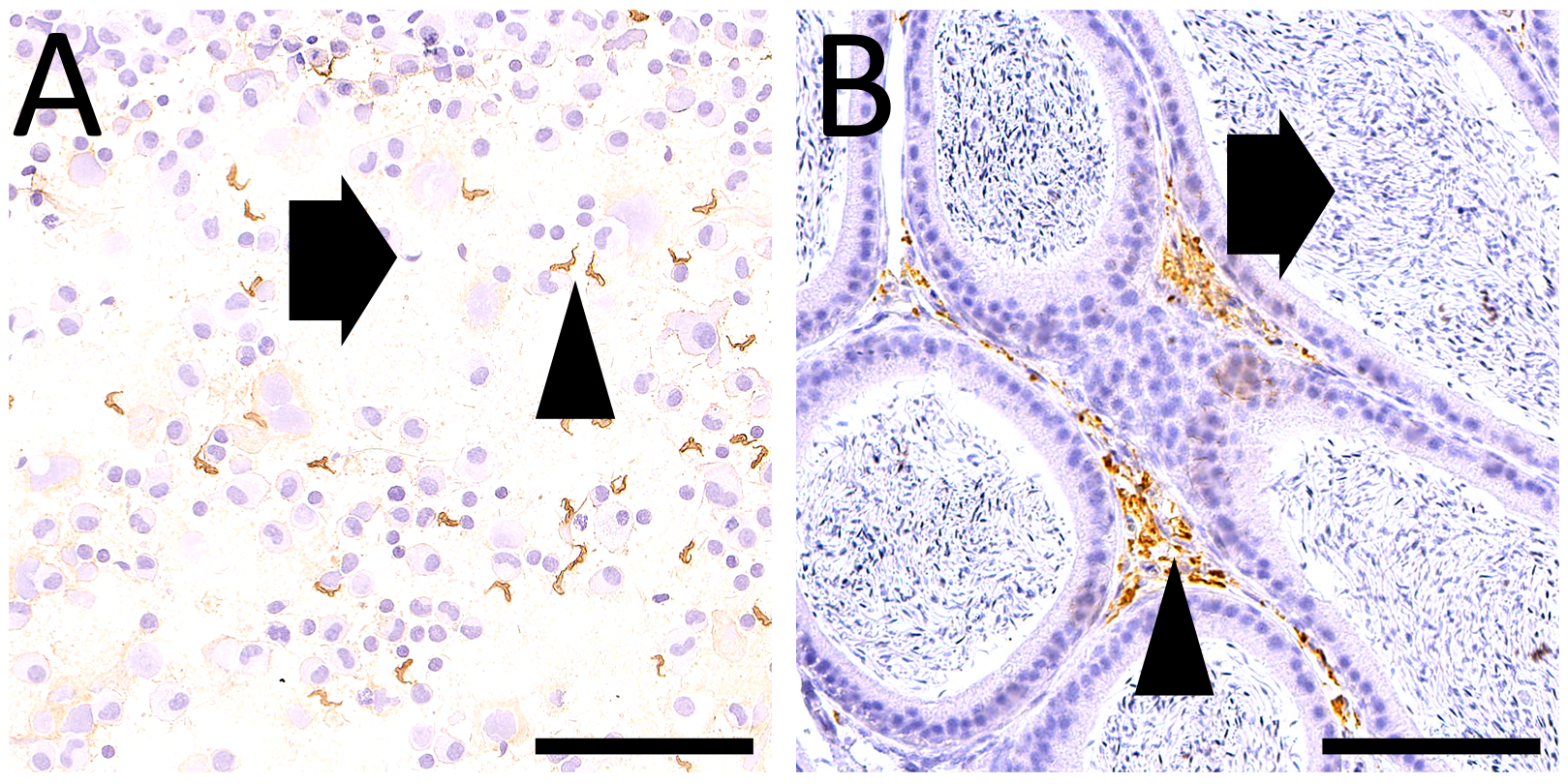
Figure 6: Comparison of epididymal cytology and histology in mice infected with T. brucei. (A) Microphotographs corresponding to an FNA smear and (B) a 4 μm paraffin section, at the same magnification (20x original magnification, Scale bar = 100 μm), both immunostained for the surface proteins of the parasite (VSG). The smear showed large numbers of parasites (arrowhead) with well-preserved cellular morphology, admixed with moderate numbers of germ cells and few spermatozoa (arrow). The histological section showed a well-preserved tissue architecture, composed of epididymal ducts with intra-luminal spermatozoa (arrow), and the presence of large numbers of parasites expanding the epididymal stroma (arrowhead). DAB counterstained with Harris hematoxylin. Original magnification: 20x (Scale bar = 100 μm). Please click here to view a larger version of this figure.
{kind=link}
Discussion
Fine Needle Aspiration (FNA) is a method widely used to diagnose disease in human and domestic animals. The technique has been standardized over many years1,2, which makes use of a small-bore needle to aspirate cells or fluid from a palpable mass or organ1,3. The aspirate is then typically smeared on a glass slide and stained for microscopic observation to achieve a diagnosis, but the technique can also be used to retrieve cells for other purposes4,5,6,7,8,9.
The procedure is quick (<5 min per mouse, for an experienced researcher) and the risk of complications is minimal, similar to the risk incurred when undergoing simple venous puncture. For this reason, for FNA of palpable masses, anesthesia is only required for sensitive anatomic locations or when a good immobilization of the animal and stabilization of the organ or mass to be aspirated is extremely crucial for optimum results. This is frequent for small laboratory animals, as safe and effective restraint of a small rodent with one hand while ensuring the best access to the area for aspiration with the other hand, is hard to achieve without anesthesia. Short-term anesthesia is in most instances sufficient, nonetheless necessary, for a good FNA in the mouse. A good immobilization maximizes the chances of obtaining an aspirate that is representative of the cellular components of the lesion and also minimizes the chances of externalizing the tip of the needle while negative pressure is applied.
Although the procedure itself is very simple, coordinated application and release of vacuum are the most critical steps. After insertion of the needle, the plunger of the syringe is retracted to achieve a controlled vacuum (suction), and the needle can only be removed from the mass after releasing the negative pressure by letting go of the plunger (Figure 2); otherwise the aspirate is sucked into the barrel of the syringe and is then very hard to recover. Another very important step is the preparation of high-quality smears. There are various methods to make a smear but regardless of the method, smears should be prepared immediately after the material has been placed onto the glass. The biological material should be spread out gently to avoid cell-crush artifacts. Use of a coverslip as spreader can help prevent these artifacts. However, the application of too much force while making the smear will break the coverslip. A good quality smear typically has most of the cell population distributed as monolayer so that they can easily transmit light. Cellular material should not be excessively trapped in the blood clot.
The goal of an FNA is to collect cells from a mass, tissue or organ. The use of larger bore needles is helpful to increase the cellularity, but can be associated with excessive blood contamination, while sampling with smaller needles yields higher quality, though less abundant material. In our case, percutaneous aspiration of the external male reproductive structures in mice experimentally infected with T. brucei, was performed with 22-gauge needles coupled to a 5 mL syringe. Mice were anesthetized, the testis was stabilized with one hand and puncture and aspiration guided and performed with the other hand. We retrieved numerous trypanosomes admixed with germ cells, spermatozoa, epithelial cells and stromal cells, which were smeared and immunostained for the parasites’ surface proteins (VSG) (Figure 4).
There is always the potential sampling error in aspirates yielding negative results because although multiple areas of a given lesion can be sampled multiple times, this is a blind aspiration where we do not visualize the needle tip and target organ or mass. This is extremely relevant in a clinical setting, where a negative FNA of a suspicious lesion does not obviate further investigations, but it’s not so relevant in animal models of disease. Thus, general limitations include mainly false negative results, and less frequently false positive results (e.g., from blood contamination), but the most important limitation in the setting of animal experimentation is the lack of information on tissue architecture17, like we have with histopathology, e.g. distribution pattern of parasites, of immune cells, and cell-cell interaction features. Nonetheless, advantages are that FNA is a non-terminal procedure allowing for the repeated sampling in the same animal over-time and always allows for better preserved cellular morphology (Figure 5). Alternatives to FNA for harvesting host cells, immune cells or microorganisms from a mouse always rely on euthanizing the mouse to collect the mass or organs of interest.
To our knowledge, there are only a few reports on the use of FNA in small laboratory animals, one from 1949 corresponding to the aspiration of bone marrow with 22 G needle for studying hematopoiesis18, and all other in combination with flow cytometry to quantify either tumor-associated inflammatory cells or endothelial cells7,19,20. Our work shows that this technique can be extended to the diagnosis and study of infectious disease models and can combine cytology with techniques like immunocytochemistry or electron microscopy. Two of the major advantages of the method in experimental animals are: (1) this procedure is not terminal, i.e., can be performed in live mice; and (2) due to its mild severity it allows for serial aspirations in the same animal. Hence fewer mice are required for each study, and the correlation between progression of clinical disease and evolution of the cellular and molecular features of a disease and/or microorganism can be easily performed, thus enabling longitudinal studies.
Perhaps the first report on the use of FNA for diagnosing an infectious diseases is a study by Grieg and Gray in 1904 that reports needle aspirations of lymph nodes from patients with sleeping sickness, which revealed motile trypanosomes12. If our findings in laboratory mice find translation to cattle, i.e., that if Trypanosoma can be easily sampled by FNA from the external male reproductive structures, one can expect that this technique will be useful to veterinarians for diagnosing animal trypanosomiasis in-farm, in livestock.
Acknowledgements
This Project was funded by Fundação para a Ciência e a Tecnologia (FCT)/ Ministério da Ciência, Tecnologia e Ensino Superior (MCTES) through Fundos do Orçamento de Estado (ref.: ID/BIM/50005/2019). LMF is an Investigator of the Fundação para a Ciência e Tecnologia (IF/01050/2014) and the laboratory is funded by ERC (FatTryp, ref.771714). Publication of this work was also funded UID/BIM/50005/2019 project funded by Fundação para a Ciência e a Tecnologia (FCT)/ Ministério da Ciência, Tecnologia e Ensino Superior (MCTES) through Fundos do Orçamento de Estado. We thank Andreia Pinto from the Histology and Comparative Pathology Laboratory of the iMM for expert Electron Microscopy assistance, and Sandra Trindade, Tiago Rebelo and Henrique Machado (iMM) for sharing tissues from infected mice.
Materials
| Name | Company | Catalog Number | Comments |
| Atipamezole (ANTISEDAN 10 mL) | Bio 2 | 7418046 | Anesthesia reversal |
| Cover slips (24 x 60 No.1) | VWR | 631-0664 | Smear making |
| DAB | Dako | K3468 | Immunocytochemistry |
| Entellan (500 mL) | VWR | 1.07961.0500 | Mounting media |
| Envision Flex antibody diluent | Dako | 8006 | Immunocytochemistry |
| EnVision Flex conjugated w/ HRP (anti-rabbit) | Dako | K4010 | Immunocytochemistry |
| Envision Flex Wash Buffer | Dako | K8007 | Immunocytochemistry |
| Giemsa stain | Atom Scientific Ltd | RRSPSS-A | Smear staining |
| Glass slides (Superfrost Plus) | VWR | 631-9483 | Smear making |
| Harris Haematoxylin | Bio-optica | 05-06004E | Immunocytochemistry |
| Hydrogen Peroxidase solution | Sigma | H1009-500ML | Immunocytochemistry |
| Hypodermic needles Microlance 3 (23G) | Henry Schein | 902-8001 | Aspiration technique |
| Ketamin (IMALGENE 1000 - 10 mL) | Bio 2 | 7410928 | Anesthesia |
| Medetomidine (DOMITOR 10 mL) | Bio 2 | 7418335 | Anesthesia |
| Methanol | Merck | 1.06009.2511 | Smear fixative |
| Pap pen | Merck | Z377821-1EA | Immunocytochemistry |
| Protein Block Serum free | Dako | X0909 | Immunocytochemistry |
| Syringes (5 mL, 10 mL) | Henry Schein | 900-3311, 900-3304 | Aspiration technique |
References
- Leopold, G., Koss, M. R. M. . Koss’ Diagnostic cytology and it’s histologic bases. , (2006).
- Raskin, R. E., Meyer, D. J. . Canine and Feline Cytology: a Color Atlas and Interpretation Guide. Canine and Feline Cytology. , (2016).
- Hopper, K. D., Abendroth, C. S., Sturtz, K. W., Matthews, Y. L., Shirk, S. J. Fine-needle aspiration biopsy for cytopathologic analysis: Utility of syringe handles, automated guns, and the nonsuction method. Radiology. 185 (3), 819-824 (1992).
- Saliba, A. E., et al. Microfluidic sorting and multimodal typing of cancer cells in self-assembled magnetic arrays. Proceedings of the National Academy of Sciences, U.S.A. 107 (33), 14524-14529 (2010).
- Guzera, M., Cian, F., Leo, C., Winnicka, A., Archer, J. The use of flow cytometry for immunophenotyping lymphoproliferative disorders in cats: a retrospective study of 19 cases. Veterinary and Comparative Oncology. 14, 40-51 (2016).
- Young, N. A., Al-Saleem, T. I., Ehya, H., Smith, M. R. Utilization of fine-needle aspiration cytology and flow cytometry in the diagnosis and subclassification of primary and recurrent lymphoma. Cancer. 40 (4), 307-319 (1998).
- Carroll, C. S. E., Altin, J. G., Neeman, T., Fahrer, A. M. Repeated fine-needle aspiration of solid tumours in mice allows the identification of multiple infiltrating immune cell types. Journal of Immunological Methods. 425, 102-107 (2015).
- Araujo, R. W., Paiva, V., Gartner, F., Amendoeira, I., Martinez Oliveira, J., Schmitt, F. C. Fine needle aspiration as a tool to establish primary human breast cancer cultures in vitro. Acta Cytologica. 43 (6), 985-990 (1999).
- Craft, I., et al. Percutaneous epididymal sperm aspiration and intracytoplasmic sperm injection in the management of infertility due to obstructive azoospermia. Fertility and Sterility. 63 (5), 1038-1042 (1995).
- Powers, C. N. Diagnosis of infectious diseases: A cytopathologist’s perspective. Clinical Microbiology Reviews. 120 (3), 351-367 (1998).
- Diamantis, A., Magiorkinis, E., Koutselini, H. Fine-needle aspiration (FNA) biopsy: Historical aspects. Folia Histochemica et Cytobiologica. 47 (2), 191-197 (2009).
- Greig, E. D. W., Gray, A. C. H. Note on the lymphatic glands in sleeping sickness. British Medical Journal. 1 (2265), 1252 (1904).
- Robson, J., Ashkar, T. S. Trypanosomiasis in domestic livestock in the Lambwe Valley area and a field evaluation of various diagnostic techniques. Bulletin of the World Health Organization. 47 (6), 727-734 (1972).
- Disease, T. African Animal Trypanosomiasis. In Vitro. , 1-15 (2009).
- Kennedy, P. G. E. Clinical features, diagnosis, and treatment of human African trypanosomiasis (sleeping sickness). Lancet Neurology. 12 (2), 186-194 (2012).
- Trindade, S., et al. Trypanosoma brucei parasites occupy and functionally adapt to the adipose tissue in mice. Cell Host and Microbe. 19 (6), 837-848 (2016).
- Carvalho, T., Trindade, S., Pimenta, S., Santos, A. B., Rijo-Ferreira, F., Figueiredo, L. M. Trypanosoma bruceitriggers a marked immune response in male reproductive organs. PLoS Neglected Tropical Diseases. 12 (8), 1-15 (2018).
- Sundberg, R. D., Hodgson, R. E. Aspiration of bone marrow in laboratory animals. Blood. 4 (5), 557-561 (2013).
- Sottnik, J. L., Guth, A. M., Mitchell, L. A., Dow, S. W. Minimally invasive assessment of tumor angiogenesis by fine needle aspiration and flow cytometry. Angiogenesis. 13 (3), 251-258 (2010).
- Betka, J., Hovorka, O., Boucek, J., Ulbrich, K., Etrych, T., Rihova, B. Fine needle aspiration biopsy proves increased T-lymphocyte proliferation in tumor and decreased metastatic infiltration after treatment with doxorubicin bound to PHPMA copolymer carrier. Journal of Drug Targeting. 21 (7), 648-661 (2013).
This article has been published
Video Coming Soon
ABOUT JoVE
Copyright © 2024 MyJoVE Corporation. All rights reserved