Iris Fixation via External Pentagram Suturing
In This Article
Summary
The present protocol describes how a 10-0 polypropylene suture crosses the anterior surface of the iris, forming a pentagram to prevent both iris and pupil from moving toward the cornea. This can be combined with subsequent keratoplasty to cure bullous keratopathy with extensive anterior synechia of the iris.
Abstract
Extensive anterior synechia of the iris can result in the gradual disappearance of the anterior chamber. It is one of the most common outcomes of both oculopathy and complicated post anterior segment surgery. This can impact visual function and lead to bullous keratopathy, making it one of the most complex clinical problems. Conventional anterior chamber plasty will partially create the anterior chamber, but the anterior chamber disappears again in some cases. The main reasons are: (1) the iris lens diaphragm is loose with atrophied and tension-free iris so that the aqueous humor circulation will push and squeeze the iris forward; (2) the effect of "roller" formed in the process of inflammation or restoration will change the iris structure from peripheral anterior synechia (PAS) to extensive anterior synechia again; (3) the fibration will result in synechia from iris to the cornea. In such cases, corneal endothelium deficiency can't stop the aqueous humor from entering the cornea. This results in persistent corneal edema post-conventional anterior chamber plasty, resulting in progressive rubbing and lachrymation. Therefore, anterior chamber plasty is not the first choice for patients without surgical indications of Descemet's stripping automated endothelial keratoplasty (DSAEK). However, this can be performed in patients with surgical indications who plan to receive DSAEK. A unique method of iris fixation via external pentagram suturing anterior chamber plasty (PSACP) is described here. The present technique is also compared with the conventional anterior chamber plasty. PSACP and DSAEK might be an effective way to cure the bullous keratopathy with extensive anterior synechia of the iris and disappeared anterior chamber.
Introduction
Extensive anterior synechia is usually observed in the eyes of patients with malignant glaucoma or primary angle-closure glaucoma after laser peripheral iridotomy or iridoplasty and after anterior segment surgery1,2,3,4,5,6. This can cause gradual reduction of the anterior chamber leading to visual dysfunction. Once extensive anterior synechia forms, the aqueous humor can enter the cornea due to endothelium decompensation, leading to bullous keratopathy7. Although a well-controlled intraocular pressure (IOP) has been obtained after lens extraction and anterior vitrectomy, the iris lens diaphragm is still soft due to atrophied and tension-free iris8. Therefore, conventional anterior chamber plasty can only temporarily form the anterior chamber9. In cases where anterior synechia is extensive, the anterior chamber disappears again and adds difficulty to the subsequent keratoplasty surgery.
Keratoplasty with iris-diaphragm intraocular lens (IOL) implantation was reported as an effective way to cure the bullous keratopathy with aniridia10,11,12,13,14. Therefore, it may be helpful to treat eyes with bullous keratopathy and extensive anterior synechia after removing the atrophied and tension-free iris. However, this idea is possibly bringing significant iatrogenic injury now and not feasible in China due to unaffordable price of such IOL.
A recent study suggested that retention or barrier sutures could prevent silicone oil from moving into the anterior chamber in aphakic eyes with iris loss15,16,17,18. Sutures enhance the surface tension of silicone oil in such situations. Therefore, the current study was conducted to investigate whether these retention or barrier sutures could improve atrophy's stress and make the iris tension-free by preventing the iris and iris lens diaphragm from approaching the cornea. The presented study was performed to explore an effective way of doing anterior chamber plasty before keratoplasty to cure the bullous keratopathy with extensive anterior synechia of the iris. The current surgery method was named "Pentagram Suturing Anterior Chamber Plasty" (PSACP) with a core process of iris fixation via external pentagram suturing.
Malignant glaucoma patients with bullous keratopathy and extensive anterior synechia who already underwent lens extraction, anterior vitrectomy, IOL implantation, and had a well-controlled IOP were included for the current study. Willingness to receive further keratoplasty to cure bullous keratopathy was also considered an inclusion criterion. Exclusion criteria include (1) eyes with no light perception, (2) IOP ≥ 35 mmHg under anti-glaucoma medications, (3) eyes with infection, acute inflammation,aniridia or chronic uveitis, (4) eyes with retinal detachment, choroidal detachment, or ciliary detachment, (5) patients with uncontrolled hypertension, cardiovascular disease, cerebrovascular disease, or diabetes mellitus, (6) patients with a severe hemorrhagic tendency or mental disorders.
Protocol
The study was approved by the Ethics Committee Review Board of Peking University Third Hospital and conformed to the Declaration of Helsinki. The new method of surgery named Pentagram Suturing Anterior Chamber Plasty (PSACP) was approved by the medical technology clinical application management Committee Review Board of Peking University Third Hospital. All the patients undergoing PSACP had provided written informed consent before the surgery.
1. Preparations before PSACP
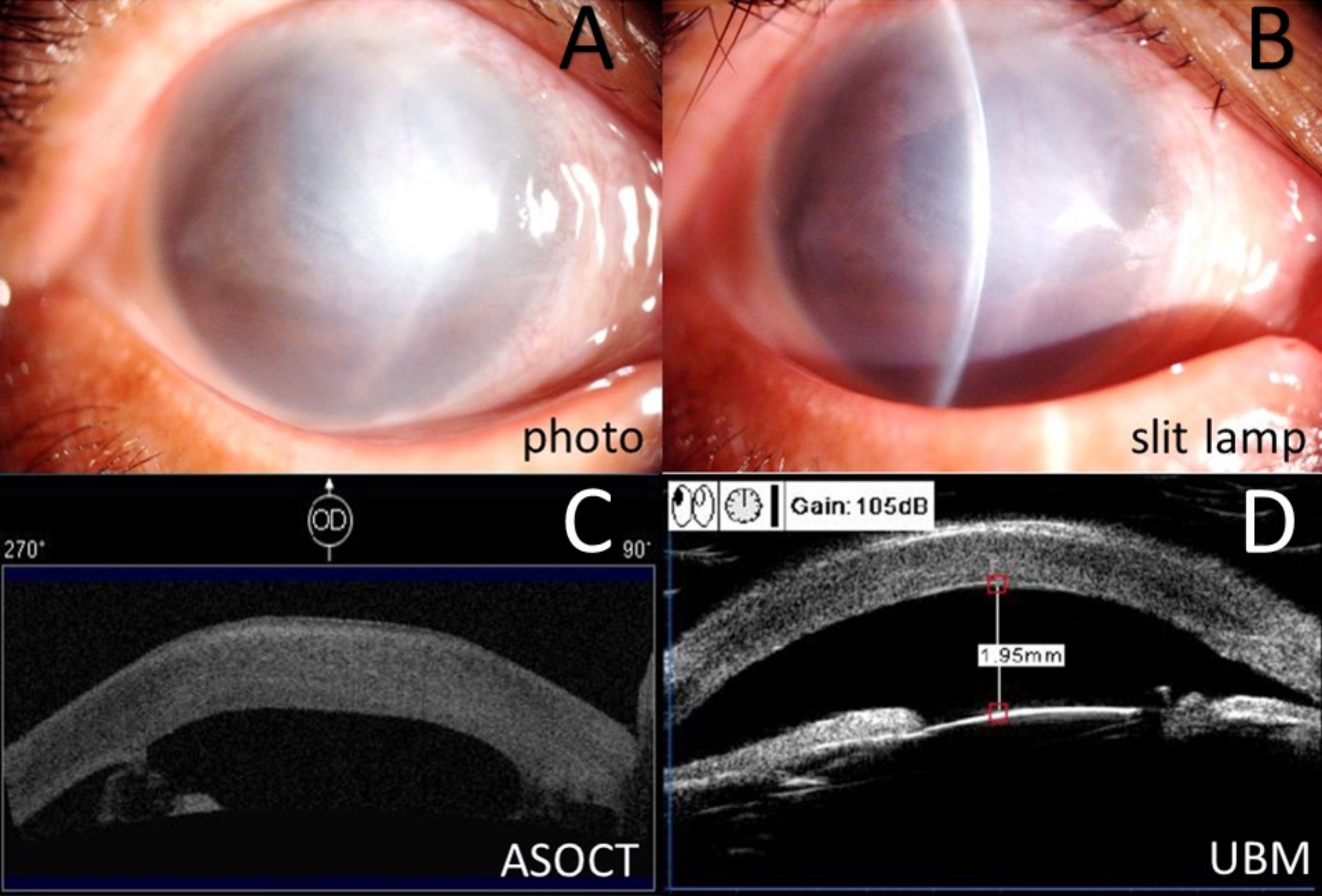
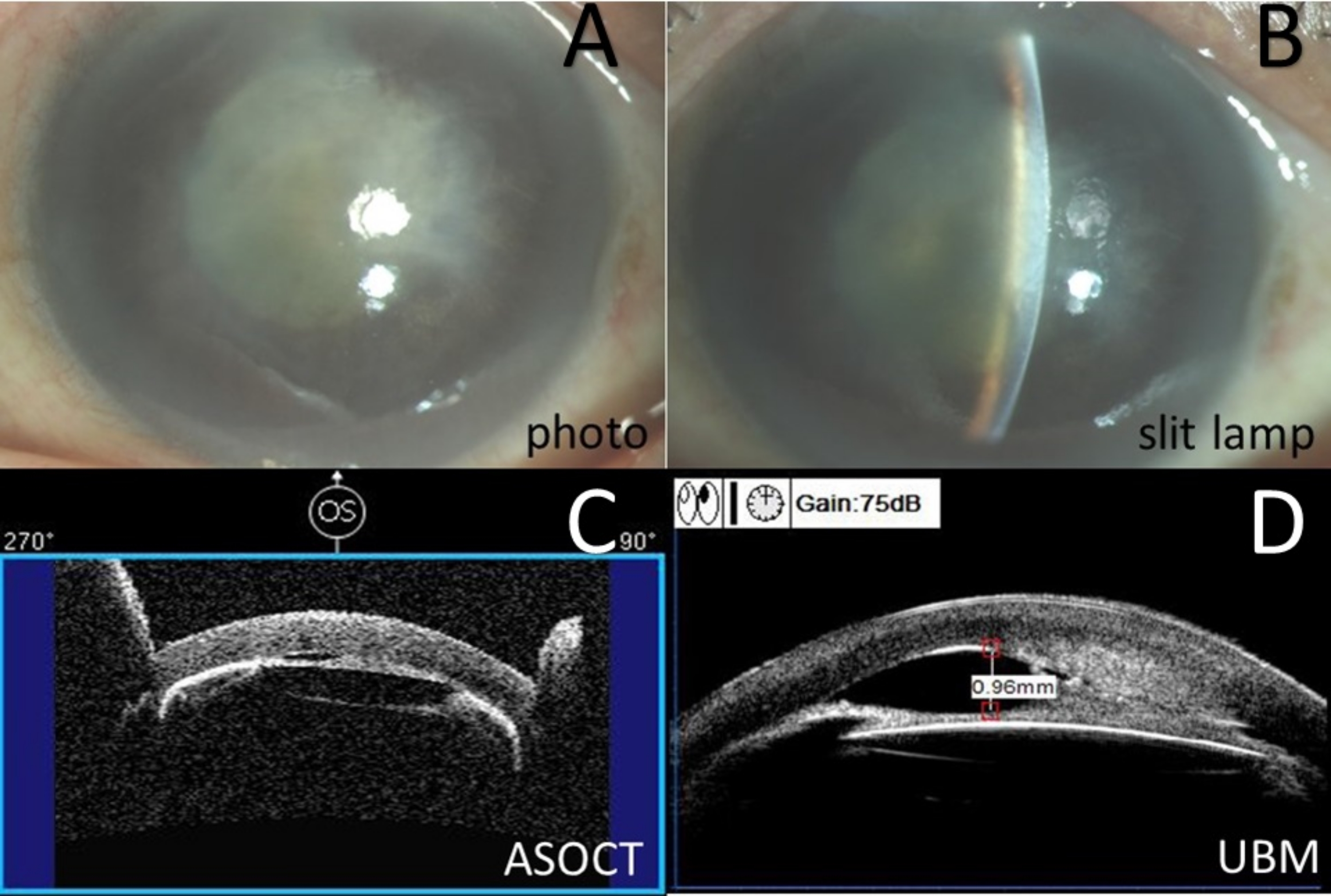
- Perform ophthalmic examinations for all the patients, including a visual acuity assessment, rebound tonometer, color slit lamp photography (Figure 1A,B), and ophthalmic ultrasound.
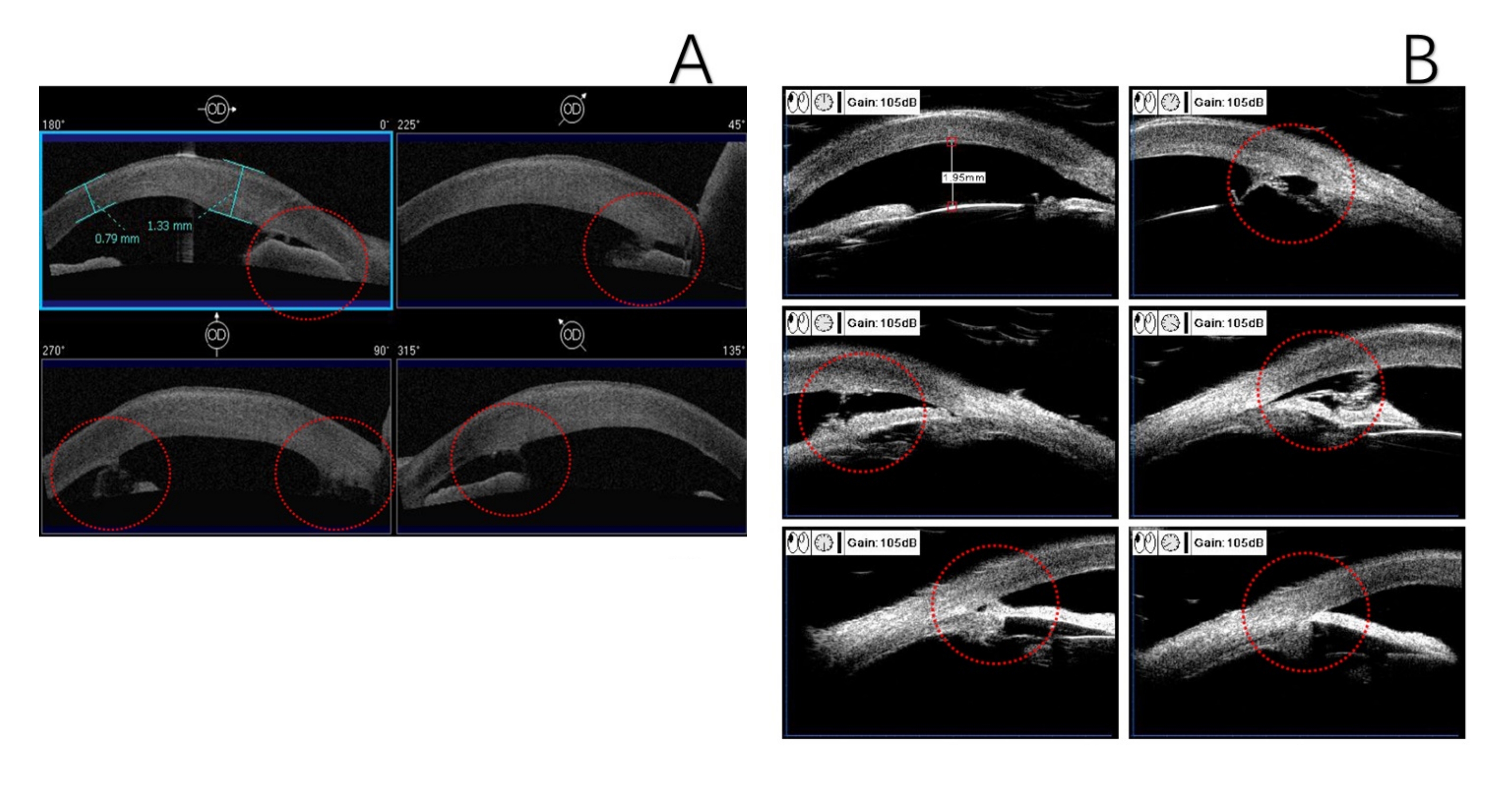
- Display the range of anterior synechia by anterior segment optical coherence tomography (ASOCT) and ultrasound biomicroscopy (UBM) to design the position of incisions (Figure 1C,D and Figure 2).
- Ensure adequate availability of 10-0 polypropylene sutures on a STC-6 needle, 29 G syringe, cohesive viscoelastic, and balanced salt solution (BSS) (see Table of Materials).
- Provide general anesthesia with 2% lidocaine hydrochloride injection (2.5 mL) (see Table of Materials).
- Place the patient in a supine position with routine disinfection, towel laying, film sticking, and palpebral fissure opening by an eye speculum.
2. Surgical procedure
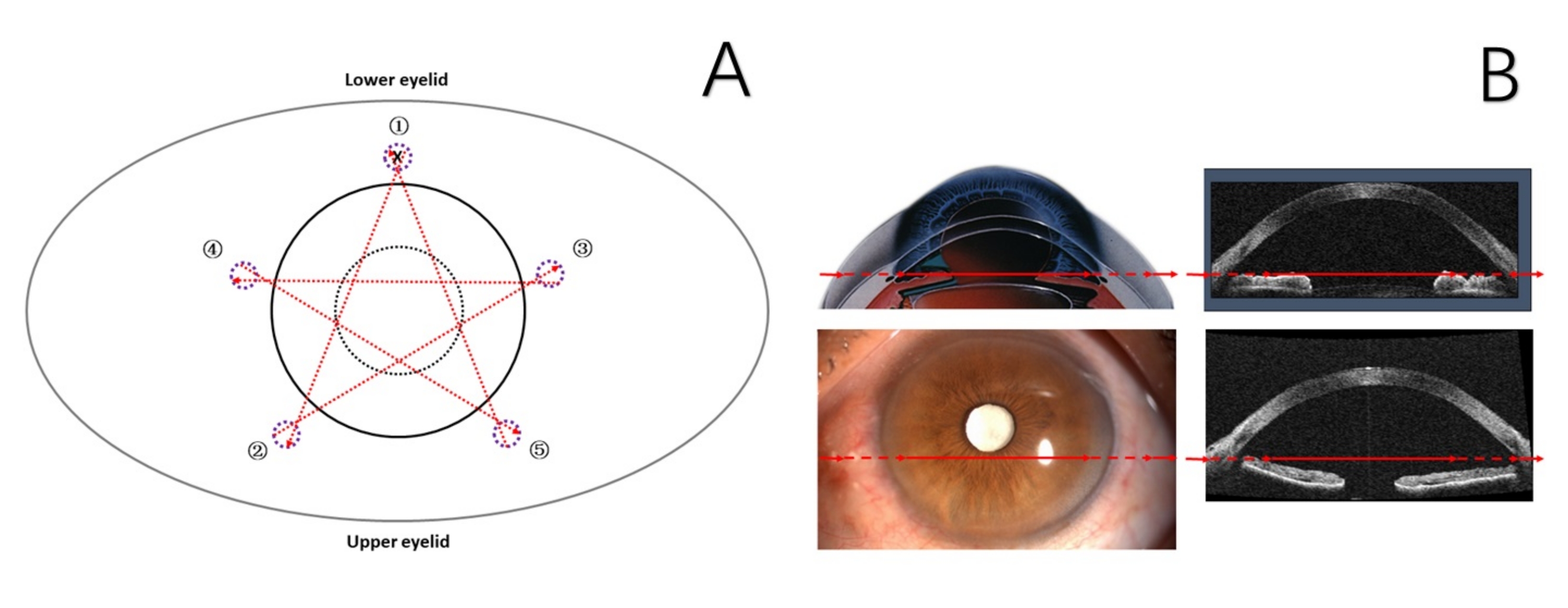
- Mark the five scleral puncture points 1.5 mm posterior to the limbus keeping away from the anti-glaucoma filtration bleb with 1% crystal violet solution. Ensure that the circular degree between the adjacent puncture points is 72° (Figure 3).
- Remove the edematous epithelium of the cornea with a sclera tunnel knife.
NOTE: Hypertonic glucose solution is recommended to reduce corneal stromal swelling. - Make a limbus incision (1 mm), inject cohesive viscoelastic to separate the anterior synechia of the iris, and remove the fibrous membranes when necessary.
- Perform blunt separation for peripheral anterior synechia (PAS).
- Insert the 16 mm (STC-6) needle from the position 1 mm beside one of the puncture points (Figure 3) into the anterior chamber and retrieve across the surface of the iris within the bore of a 29 G syringe from another side puncture point with a circular distance of 144° (Figure 3).
- When the 16 mm (STC-6) needle comes out from the anterior chamber, select the next inserting point 1 mm beside the retrieve point and 1.5 mm posterior to the limbus (Figure 3).
- Repeat steps 2.5-2.6 until the retention sutures in the anterior chamber form a pentagram-like barrier on the surface of the iris and pupil.
- Tie a surgical knot from the initial insert point and embed it into the superficial sclera under the bulbar conjunctiva.
- Perform the anterior chamber irrigation with BSS. Ensure removing all the viscoelastic, and then seal the incisions to watertight by a sterile irrigateor (see Table of Materials).
Results
Representative results from three bullous keratopathy patients with extensive anterior synechia who had a well-controlled IOP after lens extraction, anterior vitrectomy, and IOL implantation to cure malignant glaucoma are described in the study. In these cases, one received conventional anterior chamber plasty with synechia separation and penetrating keratoplasty (PKP), the other two received PSACP first, and then received Descemet's stripping automated endothelial keratoplasty (DSAEK) or PKP. Postop reaction and pigment release of all three cases were mild and faded within 4 weeks under routine anti-infection and anti-inflammatory eye drops. The prognosis of these three patients was compared on different days after 360° PAS appearance with the ASOCT (1-day post-operation) or UBM (12 weeks or 24 weeks post-operation) after the anterior chamber plasty surgery.
Case 1
A 68-year-old female was diagnosed with bullous keratopathy and extensive anterior synechia in her right eye from IOP-well-controlled (21 mmHg with four kinds of anti-glaucoma eye drops) malignant glaucoma. She already had lens extraction, anterior vitrectomy, and IOL implantation. Her right eye's best-corrected visual acuity (BCVA) was 20/4000. The iris's extensive anterior synechia was shown with ASOCT and UBM (Figure 1 and Figure 2).
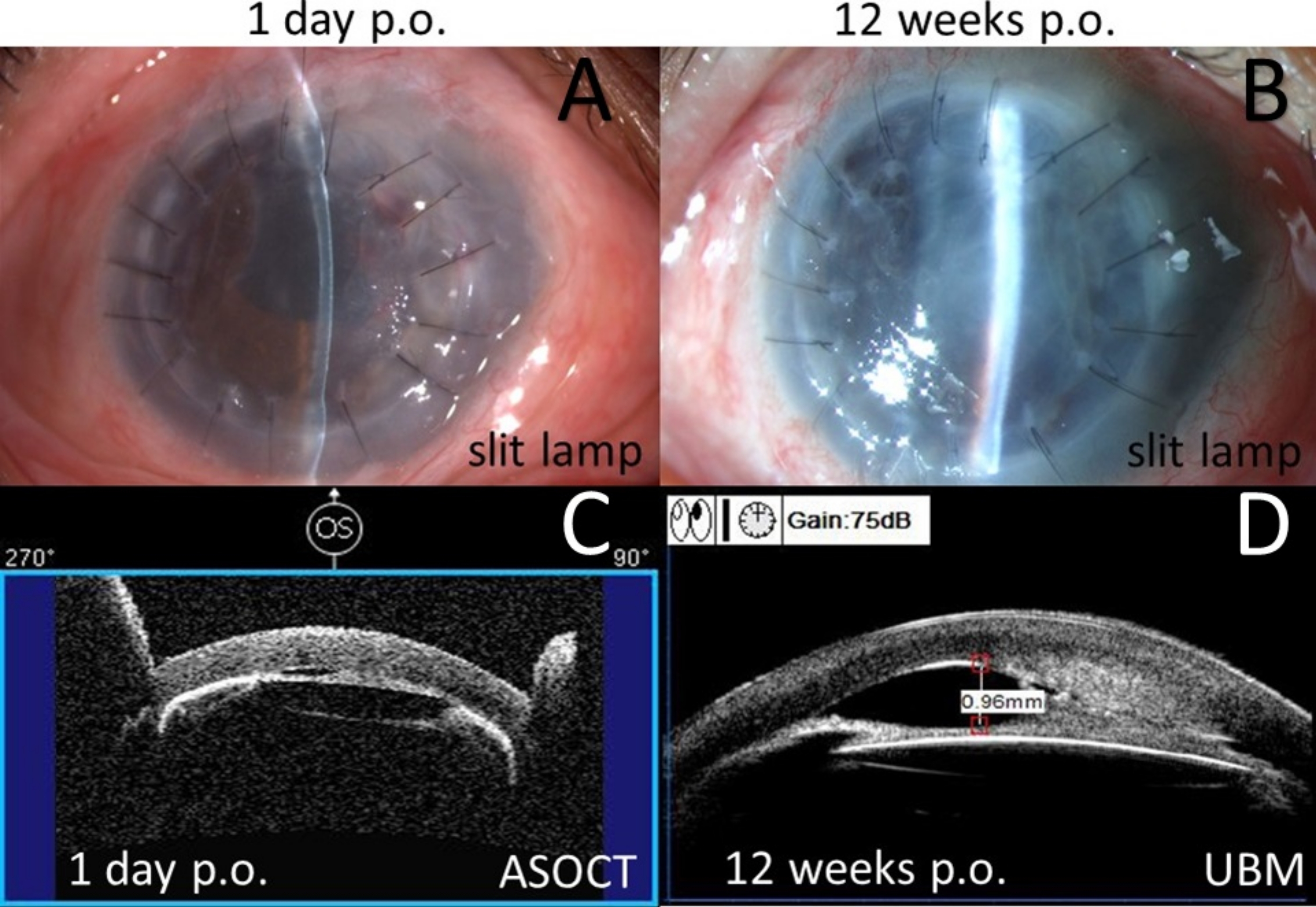
She received anterior chamber plasty with synechia separation and penetrating keratoplasty (PKP) in her right eye. One-day post-surgery (Figure 4), she showed no PAS with the ASOCT (Figure 4C), and BCVA improved to 20/1000 with elevated IOP (32 mmHg). However, 12 weeks after surgery, she showed 360° PAS with the UBM (Figure 4D), and BCVA decreased to 20/1600. At that moment, IOP was uncontrolled over 25 mmHg, and the bullous keratopathy reoccurred.
Case 2
A 75-year-old female was diagnosed with bullous keratopathy and extensive anterior synechia in her left eye from IOP-well-controlled (18 mmHg with three kinds of anti-glaucoma eye drops) malignant glaucoma, which already had lens extraction, anterior vitrectomy, and IOL implantation. BCVA of her left eye was 20/1600. The disappearance of the anterior chamber was observed with ASOCT and UBM (Figure 5).
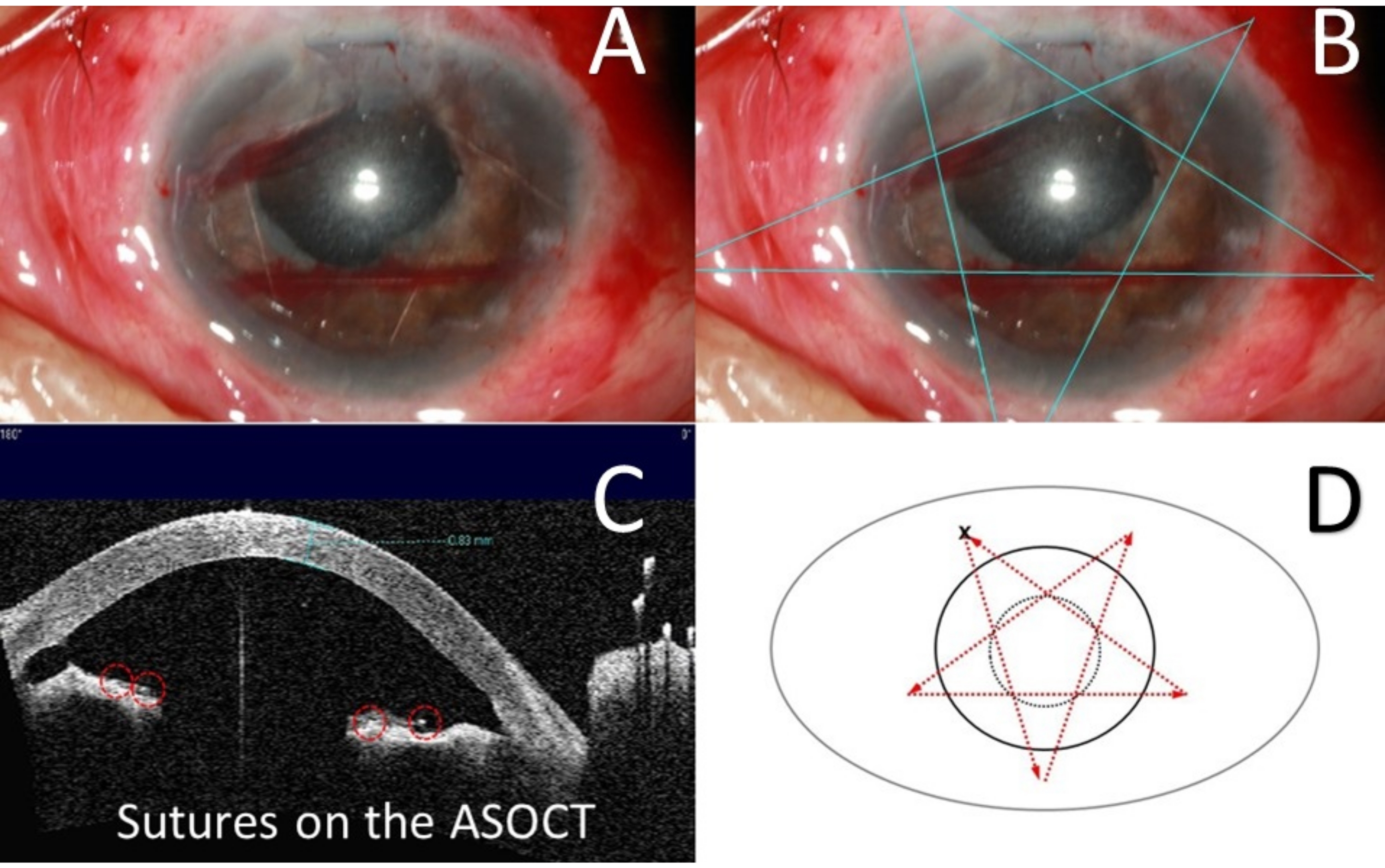
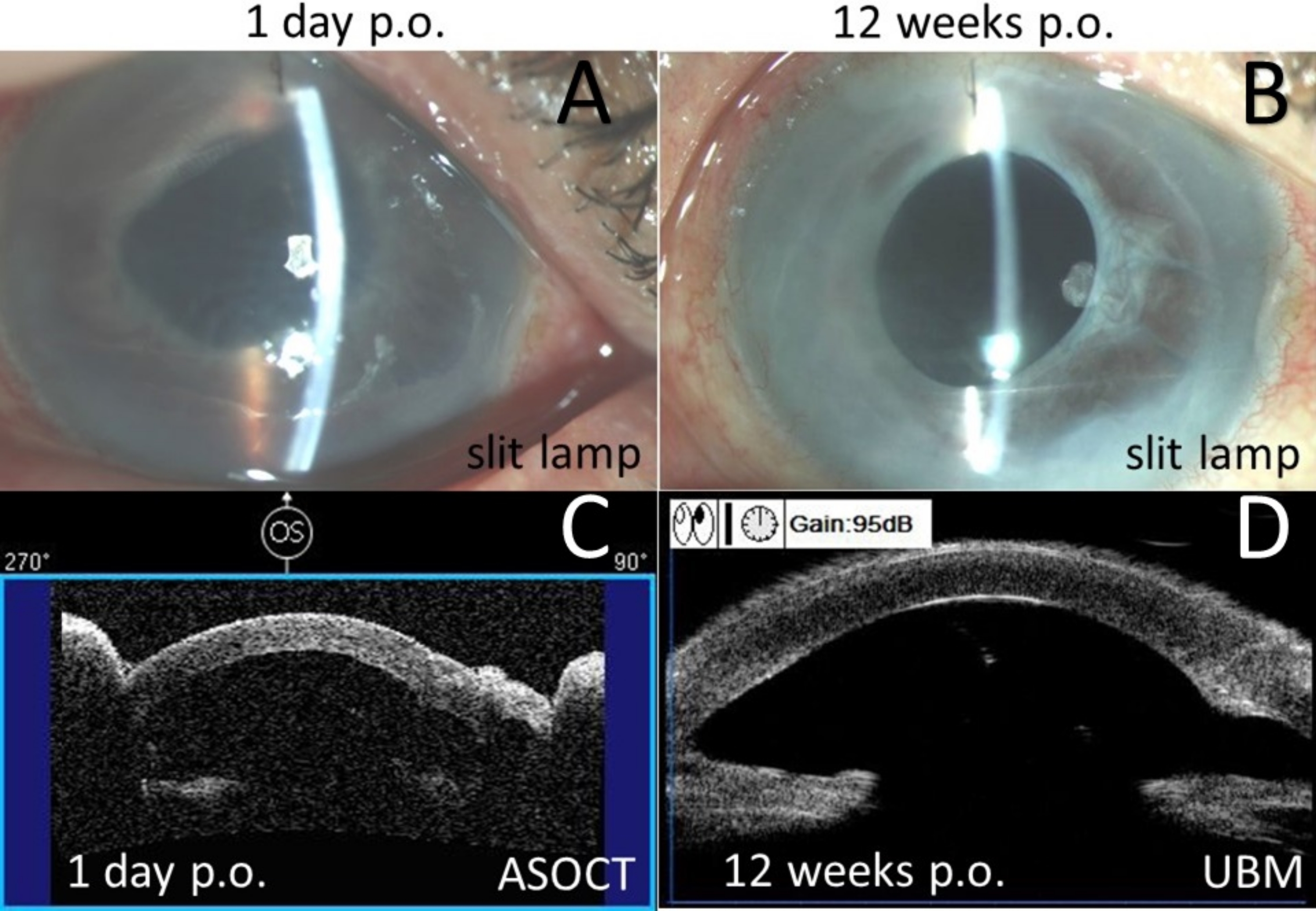
She received PSACP, where pentagram sutures were placed as a barrier in front of the anterior surface of the iris (Figure 6). No PAS was seen with ASOCT or UBM from day 1 till 12 weeks post-surgery (Figure 7). Then, she received DSAEK. On 24 weeks post-PSACP, no corneal edema was observed with ASOCT, and one clock hour PAS was demonstrated with UBM (Figure 8), with BCVA 20/66. IOP remained normal without any medication post-surgery.
Case 3
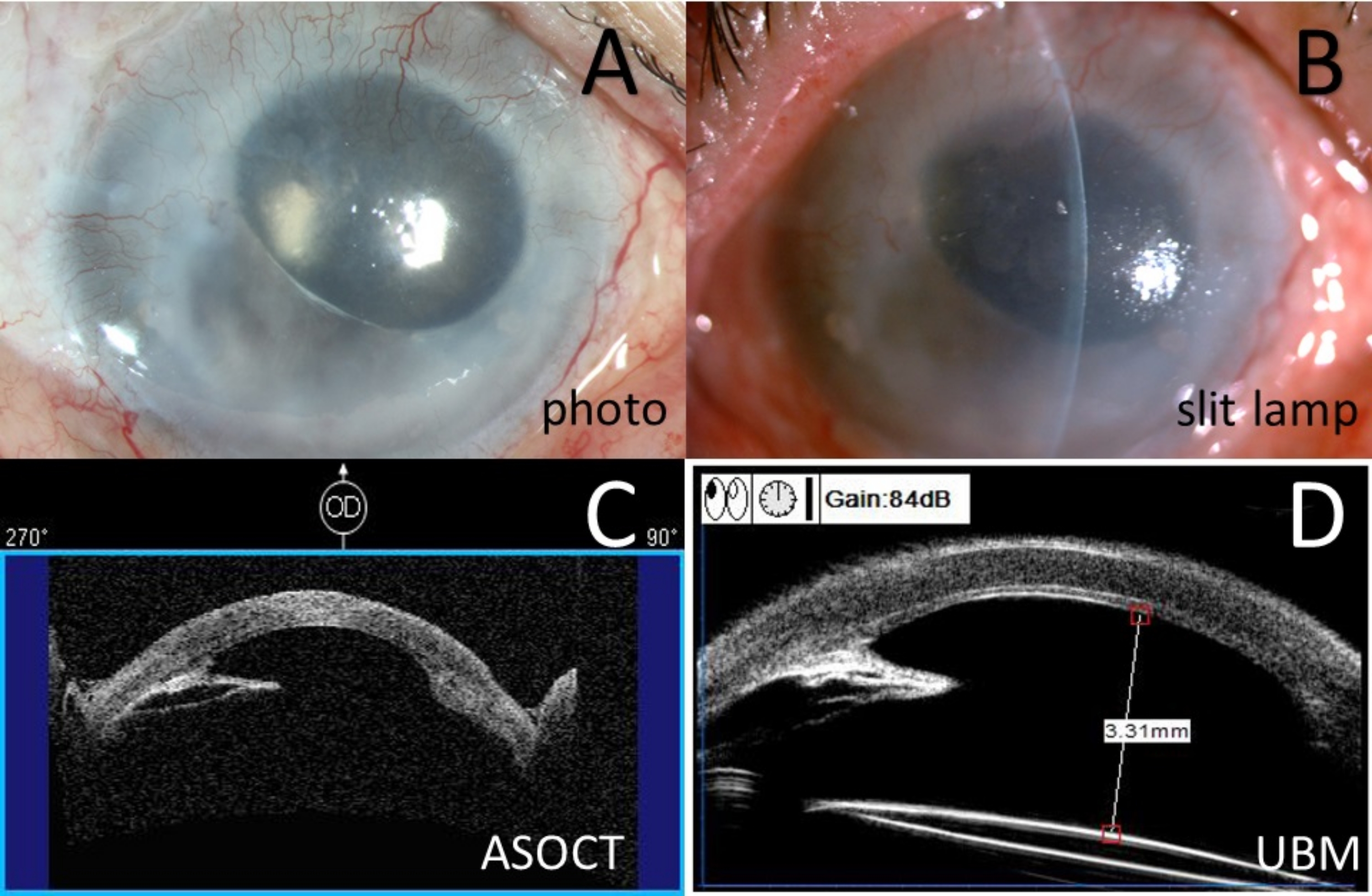
A 69-year-old female was diagnosed with bullous keratopathy and extensive anterior synechia in her right eye from IOP-well-controlled (12 mmHg with four kinds of anti-glaucoma eye drops) malignant glaucoma, which was post lens extraction, anterior vitrectomy, IOL implantation, and DSAEK. The BCVA of her right eye was 20/1600. Extensive PAS was shown with ASOCT and UBM (Figure 9).
She received PSACP and showed 2 clock hours PAS with ASOCT on day 1 post-surgery, and she missed the 12-week-follow-up. As she showed 6 clock hours PAS with UBM in 24 weeks post-surgery (Figure 10), she received PKP. During PKP, the suture was broken accidentally and then removed. On 1-week post PKP, she showed mild edema in the cornea graft and 6 clock hours PAS with the ASOCT (Figure 11) with improved BCVA 20/400. IOP remained normal without any medication post-surgery. Unfortunately, she did not follow up.
Comparisons
BCVA, IOP, cornea or corneal graft, anterior synechia of iris were found in these three patients preoperationally and post-operationally (Table 1 and Table 2). The prognosis of Case 2 and Case 3 was significantly better than in Case 1.

Figure 1: Preoperative examinations for Case 1. (A) Anterior segment photography. (B) Color slit-lamp photography. (C) Anterior segment optical coherence tomography (ASOCT). (D) Ultrasound biomicroscopy (UBM). Please click here to view a larger version of this figure.
{kind=link}

Figure 2: Assessment of anterior synechia of iris for Case 1. (A) Anterior segment optical coherence tomography. (B) Ultrasound biomicroscopy. Red circle: anterior synechia of the iris. Please click here to view a larger version of this figure.
{kind=link}

Figure 3: Schematic representation of the procedure of PSACP for Case 3. (A) Black dashed circle: pupil; black circle: limbus; purple dashed circle: the mark of scleral puncture point; numbers and red arrow: suturing sequence and direction, both ends of the red arrow represent the exact puncture points; X: the surgical knot. (B) Red arrow: suturing position and direction. PSACP = Pentagram Suturing Anterior Chamber Plasty. Please click here to view a larger version of this figure.
{kind=link}

Figure 4: Postoperative examinations for Case 1. (A) Color slit lamp photography on day 1 post-operation. (B) Color slit lamp photography in 12 weeks post-operation. (C) Anterior segment optical coherence tomography (ASOCT) on day 1 post-operation. (D) Ultrasound biomicroscopy (UBM) in 12 weeks post-operation. Please click here to view a larger version of this figure.
{kind=link}

Figure 5: Preoperative examinations for Case 2. (A) Anterior segment photography. (B) Color slit-lamp photography. (C) Anterior segment optical coherence tomography (ASOCT). (D) Ultrasound biomicroscopy (UBM). Please click here to view a larger version of this figure.
{kind=link}

Figure 6: Diagrammatic sketches of PSACP in operation for Case 2. (A) Color photography for sutures. (B) Blueline: pentagram sutures. (C) Anterior segment optical coherence tomography (ASOCT) on day 1 post-operation, red circle: sutures. (D) Black dashed circle: pupil; black circle: limbus; red arrow: suturing direction; X: the surgical knot. PSACP = Pentagram Suturing Anterior Chamber Plasty. Please click here to view a larger version of this figure.
{kind=link}

Figure 7: Postoperative examinations for Case 2. (A) Color slit lamp photography on day 1 post-operation. (B) Color slit lamp photography in 12 weeks post-operation. (C) Anterior segment optical coherence tomography (ASOCT) on day 1 post-operation. (D) Ultrasound biomicroscopy (UBM) in 12 weeks post-operation. Please click here to view a larger version of this figure.
{kind=link}

Figure 8: Postoperative examinations for Case 2 in 24 weeks post PSACP. (A) Color slit lamp photography, yellow arrow: sutures in the anterior chamber. (B) Color slit lamp photography, blue line: pentagram sutures. (C) Anterior segment optical coherence tomography (ASOCT) showed the cornea and endothelium graft. (D) Ultrasound biomicroscopy (UBM). PSACP = Pentagram Suturing Anterior Chamber Plasty. Please click here to view a larger version of this figure.
{kind=link}

Figure 9: Preoperative examinations for Case 3. (A) Anterior segment photography. (B) Color slit-lamp photography. (C) Anterior segment optical coherence tomography (ASOCT). (D) Ultrasound biomicroscopy (UBM). Please click here to view a larger version of this figure.
{kind=link}

Figure 10: Postoperative examinations for Case 3. (A) Color slit lamp photography on day 1 post-operation. (B) Color slit lamp photography in 24 weeks post-operation. (C) Anterior segment optical coherence tomography (ASOCT) on day 1 post-operation. (D) Ultrasound biomicroscopy (UBM) in 24 weeks post-operation. Red circle: sutures. Please click here to view a larger version of this figure.
{kind=link}

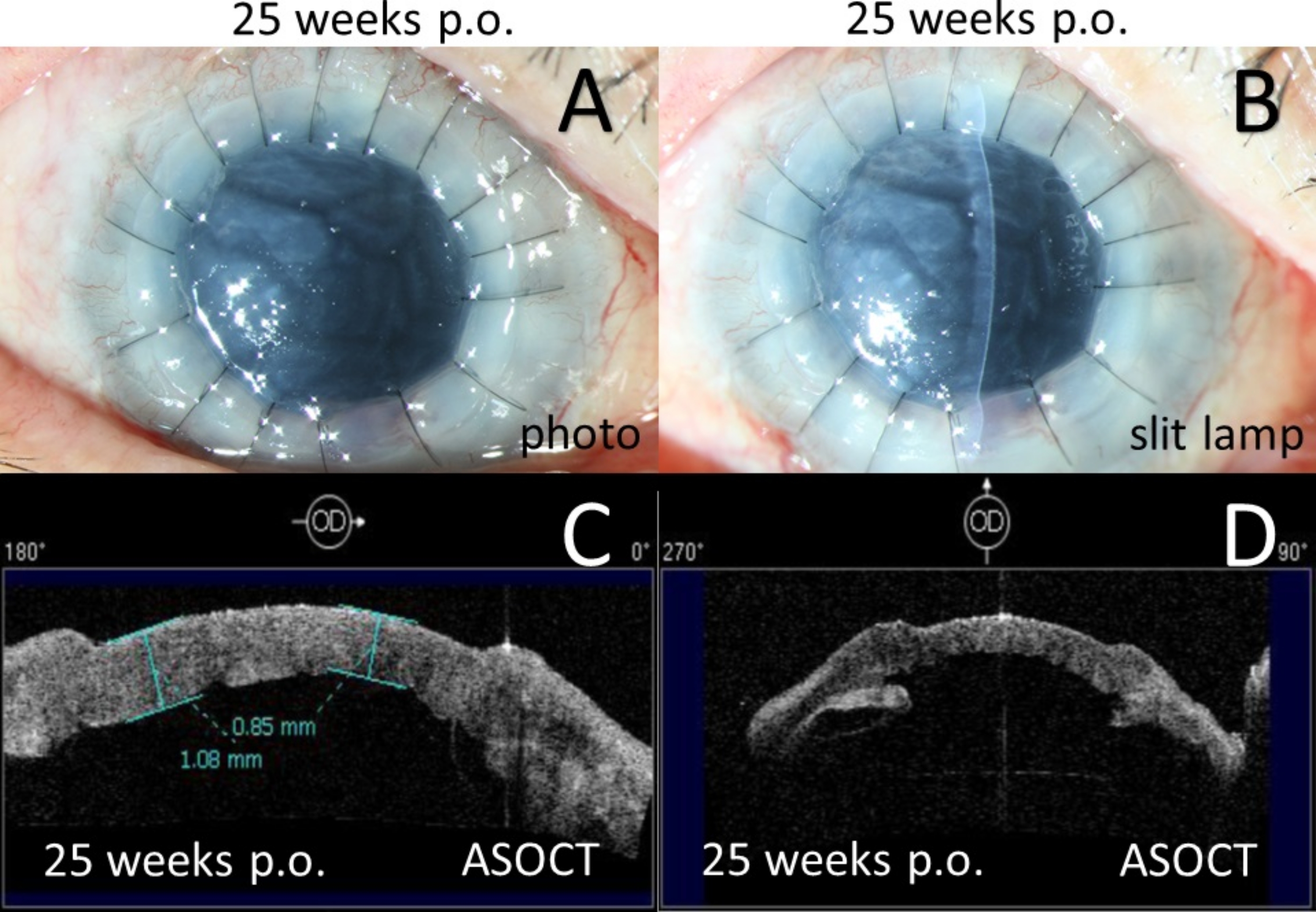
Figure 11: Postoperative examinations for Case 3 in 25 weeks post PSACP. (A) Anterior segment photography in 1 week post PKP. (B) Color slit lamp photography in 1 week post PKP. (C) Anterior segment optical coherence tomography (ASOCT) showed the cornea and graft. (D) Anterior segment optical coherence tomography (ASOCT) showed anterior synechia of the iris. PSACP = Pentagram Suturing Anterior Chamber Plasty. PKP = penetrating keratoplasty. Please click here to view a larger version of this figure.
{kind=link}
| Case | Kind of surgery | BCVA | IOP (mmHg) | Kind of anti-glaucoma eye drops | |||
| Pre-op. | Postop. | Pre-op. | Postop.* | Pre-op. | Postop. | ||
| 1 | CACP+PKP | 20/4000 | 20/1600 | 21 | 25 | 4 | 3 |
| 2 | PSACP, DSAEK | 20/1600 | 20/66 | 18 | 13 | 3 | 0 |
| 3 | PSACP, PKP | 20/1600 | 20/400 | 12 | 14 | 3 | 0 |
Table 1: Visual acuity, intraocular pressure, and medications of the presented cases. BCVA = best-corrected visual acuity; IOP = intraocular pressure; Pre-op. = pre-operational; Postop. = post-operational; CACP = conventional anterior chamber plasty; PKP = penetrating keratoplasty; PSACP = Pentagram Suturing Anterior Chamber Plasty; DSAEK = Descemet's stripping automated endothelial keratoplasty.
| Case | Kind of surgery | Cornea/Corneal graft edema | Anterior synechia of iris (ASOCT) | Anterior synechia of iris (UBM) | |||
| Pre-op. | Postop. | Pre-op. | Postop.* | Pre-op. | Postop. | ||
| 1 | CACP+PKP | Yes | No | 8CH | No | 9CH | 9CH |
| 2 | PSACP, DSAEK | Yes | No | 12CH | No | 12CH | 1CH |
| 3 | PSACP, PKP | Yes | No | 12CH | 2CH | 12CH | 6CH# |
Table 2: Clinical characteristics of cornea and iris of the presented cases. ASOCT = anterior segment optical coherence tomography; UBM = Ultrasound biomicroscopy; Pre-op. = preoperational; Postop. = post operational; CACP = conventional anterior chamber plasty; PKP = penetrating keratoplasty; CH = clock hour; PSACP = Pentagram Suturing Anterior Chamber Plasty; DSAEK = Descemet's stripping automated endothelial keratoplasty. * = 1 day post PSACP. # = 24 weeks post PSACP.
Discussion
Bullous keratopathy with extensive anterior synechia has been considered one of the most challenging clinical problems. Although well-controlled IOP with successful lens extraction and anterior vitrectomy surgery was performed, the iris lens diaphragm was still flabby with the existence of an atrophied and tension-free iris. Case 1 showed that even when PKP was completed, conventional anterior chamber plasty with synechia separation would only partially and temporarily form in the anterior chamber. The main reasons are: (1) the aqueous humor circulation would continuously push and squeeze the atrophied and tension-free iris forward; (2) the effect of "roller" formed in the process of inflammation or restoration would make the iris from PAS to extensive anterior synechia again; (3) the fibration would result in synechia from iris to the cornea.
Keratoplasty with iris-diaphragm IOL implantation was a valuable method to cure the bullous keratopathy with aniridia10,11,12,13,14. To solve such extensive anterior synechia of the iris, iris-diaphragm IOL implantation after removing the iris might work15. However, total iridectomy was a surgery with significant iatrogenic injury, and iris-diaphragm IOL comes at an unaffordable price in China. A new method of forming a stable anterior chamber without recurrent extensive anterior synechia was needed to be explored.
Gentile et al.16 first reported the "# pattern" retention sutures across the anterior chamber to simulate an iris diaphragm. They made the sutures act as a barrier between the silicone oil and aqueous, preventing silicone oil-corneal contact, and this has been effective over 3-6 months. To deal with an atrophied and tension-free iris, there must be enough line segments and points of crossing to prevent the peripheral iris or pupil from moving forward to the cornea. The "# pattern" retention sutures could work well theoretically. But it was a complicated operation with 20 suture segments and 16 points of crossing times of sclerocentesis, which prolonged the operation time and increased the risk of infection. Similarly, this problem was even more severe in the report of Kemal et al.17 with "Chessboard pattern" barrier sutures.
Syed et al.18 and Du et al.19 suggested that improved "Z pattern" retention sutures could prevent silicone oil from moving to the anterior chamber in aphakic eyes with iris loss for 3-6 months. However, the points of crossing within the improved "Z pattern" sutures were not enough to prevent anterior synechia of the iris. Moreover, theoretically, triangle or quadrilateral sutures would be even worse than the improved "Z pattern" sutures.
In the current study, PSACP was invented because pentagram was a magical pattern with 15 line segments and 10 points of crossing, especially drawing with one stroke. Therefore, PSACP could not only use one 10-0 prolene suture alone across the anterior surface of the iris, forming a barrier in front of the iris by the 15 suture segments from the pentagram but also prevent the pupil from moving forward to the cornea by the central five points of crossing and fix the suture to the surface or superficial sclera by the peripheral five points of crossing. With the help of PSACP, the anterior chamber was stable with iris fixation and almost without recurrency of anterior synechia for at least 12 weeks in Case 2. Finally, Case 2 received DSAEK, and the bullous keratopathy was cured.
To our knowledge, DSAEK was one of the best surgeries to cure bullous keratopathy with minimally invasive, time-saving, and fast recovery7,20,21. The operative procedure needed adequate space basis in the anterior chamber. In Case 3, some recurrent anterior synechia resulted in an unstable anterior chamber in 24 weeks post-PSACP, suggesting that the timing of DSAEK was recommended from 4-12 weeks post-PSACP. Furthermore, Case 3 had received DSAEK jet and had also been performed with conventional anterior chamber plasty several times. If DSAEK was performed again, it might bring in more severe inflammation, restoration or fibration, and uncontrolled IOP. Therefore, PKP was finally performed. However, retention sutures were broken accidentally in PKP, and PAS was formed rapidly in 1-week post PKP, implying that PSACP prevented the iris from moving toward the cornea in such a complicated case only to some extent. Care needs to be taken of these sutures during the PKP procedure.
The limitation of this study was that it was a pilot study with only three cases with stringent inclusion and exclusion criteria. The success and benefits of PSACP with subsequent DSAEK or PKP were shown in two instances from only one hospital. Further studies in multi-center with a bigger sample size might be helpful to improve the flow chart.
In summary, iris fixation via PSACP might provide an adequate space basis for DSAEK to help cure the bullous keratopathy caused by a vanished anterior chamber or extensive anterior synechia to some extent. PSACP and DSAEK or PKP might be an effective way to cure the bullous keratopathy with extensive anterior synechia of the iris.
Disclosures
The authors have nothing to disclose.
Acknowledgements
The authors have no one to acknowledge.
Materials
| Name | Company | Catalog Number | Comments |
| 1% crystal violet solution | HEBEI JINZHONG PHARMACEUTIAL CO., LTD. Hebei, PRC | 200709 | |
| 10-0 prolene sutures on an STC-6 needle | Alcon Laboratories, Inc.,Sinking Spring, PA | 13M4AT | |
| 2% lidocaine hydrochloride injection | TIANSHENG PHARMACEUTIAL GROUP CO., LTD. Hubei, PRC | 42021839 | |
| 29-gauge syringe | Becton, Dickinson and Company, NE 68949 | 160404 | |
| Anterior segment optical coherence tomography | Carl Zeiss Meditec, Inc., Dublin, CA | 1000-1238 | |
| Balanced salt solution | Alcon Laboratories,Inc., Fort Worth,TX | 7950191 | |
| Cohesive viscoelastic | Bausch+Lomb Inc., Shandong, CN | 6.92409E+12 | |
| Color slit lamp photography | HAAG-STREIT AG, Gartenstadtstrasse 10, 3098 Koeniz, Switzerland | 6543-2012 | |
| Rebound tonometer (iCare, Type TA01i) | Tiolat Oy, Finland | 44 | |
| Sterile irrigator for single use | SHANDONG WEIGAO GROUP MEDICAL POLYMER CO., LIMITED | (01)06932992101486 | |
| Ultrasound biomicroscopy | Paradigm Medical Industries, Salt Lake City, UT | 5290-2012 |
References
- Tsai, Y. -. Y., Tseng, S. H. Combined trabeculectomy and vitrectomy for pseudophakic malignant glaucoma and extensive peripheral anterior synechia-induced secondary glaucoma. Journal of Cataract & Refractive Surgery. 30 (3), 715-717 (2004).
- Lim, L. S., et al. Acute primary angle closure: configuration of the drainage angle in the first year after laser peripheral iridotomy. Ophthalmology. 111 (8), 1470-1474 (2004).
- Sawada, A., Yamamoto, T. Correlation between extent of preexisting organic angle closure and long-term outcome after laser peripheral iridotomy in eyes with primary angle closure. Journal of Glaucoma. 21 (3), 174-179 (2012).
- Ollerton, A., et al. Long-term pathologic follow-up of obsolete design: Choyce Mark VIII anterior chamber intraocular lens. Journal of Cataract & Refractive Surgery. 38 (2), 368-372 (2012).
- Latifi, G., et al. Effect of phacoemulsification on drainage angle status in angle closure eyes with or without extensive peripheral anterior synechiae. European Journal of Ophthalmology. 23 (1), 70-79 (2013).
- Narang, P., Agarwal, A., Kumar, D. A. Single-pass four-throw pupilloplasty for angle-closure. Indian Journal of Ophthalmology. 66 (1), 120-124 (2018).
- Nakatani, S., Murakami, A. Three-year outcome of Descemet stripping automated endothelial keratoplasty for bullous keratopathy after argon laser iridotomy. Cornea. 33 (8), 780-784 (2014).
- Liarakos, V. S., et al. Endothelial keratoplasty for bullous keratopathy in eyes with an anterior chamber intraocular lens. Journal of Cataract & Refractive Surgery. 39 (12), 1835-1845 (2013).
- Narang, P., Agarwal, A., Kumar, D. A. Single-pass 4-throw pupilloplasty for pre-descemet endothelial keratoplasty. Cornea. 36 (12), 1580-1583 (2017).
- Ozbek, Z., Kaynak, S., Zengin, O. Transscleral fixation of a black diaphragm intraocular lens in severely traumatized eyes requiring vitreoretinal surgery. Journal of Cataract & Refractive Surgery. 33 (8), 1494-1498 (2007).
- Aslam, S. A., Wong, S. C., Ficker, L. A., MacLaren, R. E. Implantation of the black diaphragm intraocular lens in congenital and traumatic aniridia. Ophthalmology. 115 (10), 1705-1712 (2008).
- Li, J., Yuan, G., Ying, L., Yu, B., Dong, X. Modified implantation of black diaphragm intraocular lens in traumatic aniridia. Journal of Cataract & Refractive Surgery. 39 (6), 822-825 (2013).
- Qiu, X., Ji, Y., Zheng, T., Lu, Y. Long-term efficacy and complications of black diaphragm intraocular lens implantation in patients with traumatic aniridia. British Journal of Ophthalmology. 99 (5), 659-664 (2015).
- Qiu, X., Ji, Y., Zheng, T., Lu, Y. The efficacy and complications of black diaphragm intra-ocular lens implantation in patients with congenital aniridia. Acta Ophthalmologica. 94 (5), 340-344 (2016).
- Chorgiewicz, T., et al. Transscleral fixation of black diaphragm intraocular lens in complete aniridia and aphakia due to posttraumatic eye rupture: A pilot study. Journal of Clinical Medicine. 8 (1), 46 (2019).
- Gentile, R. C., Eliott, D. Silicone oil retention sutures in aphakic eyes with iris loss. Archives of Ophthalmology. 128 (12), 1596-1599 (2010).
- Yüksel, K., et al. Silicone oil barrier sutures in aphakic eyes with iris defects. Retina. 36 (6), 1222-1226 (2016).
- Syed, R., Jusufbegovic, D., Schaal, S. A needle-free minimally invasive surgical technique for the placement of silicone oil retention sutures. Retina. 36 (5), 1032-1034 (2016).
- Du, W., Chen, F., Zhu, J., Xie, Z. Application of modified silicone oil retention sutures in traumatic aphakic eyes with iris loss. Retina. , (2019).
- Peng, R. -. M., Hao, Y. -. S., Chen, H. -. J., Sun, Y. -. X., Hong, J. Endothelial keratoplasty: the use of viscoelastic as an aid in reattaching the dislocated graft in abnormally structured eyes. Ophthalmology. 116 (10), 1897-1900 (2009).
- Busin, M., Madi, S., Santorum, P., Scorcia, V., Beltz, J. Ultrathin descemet's stripping automated endothelial keratoplasty with the microkeratome double-pass technique: Two-year outcomes. Ophthalmology. 120 (6), 1186-1194 (2013).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved