
Method Article
Erken Viral Giriş Tespiti için Tahliller ve Antiviral Bileşiklerin Değerlendirilmesi
Bu Makalede
Özet
Here, we present a protocol that examines specific steps of the viral entry to identify and evaluate novel antiviral agents.
Özet
Cell-based systems are useful for discovering antiviral agents. Dissecting the viral life cycle, particularly the early entry stages, allows a mechanistic approach to identify and evaluate antiviral agents that target specific steps of the viral entry. In this report, the methods of examining viral inactivation, viral attachment, and viral entry/fusion as antiviral assays for such purposes are described, using hepatitis C virus as a model. These assays should be useful for discovering novel antagonists/inhibitors to early viral entry and help expand the scope of candidate antiviral agents for further drug development.
Giriş
Viral infections are a constant threat to the public health and a significant cause of epidemic diseases, morbidity, and deaths worldwide. Specific modes of control against viral infections include vaccine development and antiviral therapies. While vaccine efforts have proven successful in immunizing against several viruses, many viral pathogens remain without a protective vaccine including dengue virus (DENV), human cytomegalovirus (HCMV), hepatitis C virus (HCV), human immunodeficiency virus (HIV), and respiratory syncytial virus (RSV)1-5. Antivirals, on the other hand, play an important role for the management of these viral infections when prophylactic vaccines are unavailable. However, to date, only few licensed and cost-effective antiviral drugs are available compared to the number of viral pathogens that threatens the public health. More importantly, due to an increase in global travel and rapid urbanization, the situation is aggravated by risks of epidemic outbreaks from emerging/re-emerging viral infections that are being introduced into non-indigenous areas6. Recent outbreaks caused by severe acute respiratory syndrome (SARS) virus, influenza viruses (H1N1, H5N1, H3N2, and H7N9), DENV, West Nile virus (WNV), measles virus (MV), Middle East Respiratory Syndrome (MERS) virus, and Ebola virus6-12 are among the examples reflecting the need for antivirals development when immunization and/or therapeutics are unavailable. In addition, there is always a potential risk of generating drug-resistant infections with currently used antivirals. Thus, the continuous development and expansion of the scope of antivirals to these emerging/re-emerging viral infections are necessary to provide better management strategies and safeguard the public health.
Most antiviral therapies consist of direct acting antivirals (DAAs) which target a specific viral protein or cofactor that mediates important steps in the viral life cycle. For example, the nucleoside analogue Acyclovir inhibits herpesvirus DNA polymerase, protease inhibitors Boceprevir and Telaprevir antagonize the HCV NS3, and Oseltamivir and Zanamivir are neuraminidase inhibitors that block the release of influenza virus particles from infected cells13-15. There are however very few licensed viral entry inhibitors including Enfuvirtide, which targets HIV gp41 to prevent fusion, and Maraviroc, which blocks the HIV co-receptor CCR5, thereby preventing viral entry16. Exploring novel antagonists/inhibitors to viral entry could help provide additional therapeutics for prophylactic or therapeutic use, such as in combination with other antivirals with a different mechanism of action to better manage viral infections17-19.
Identification of antivirals can involve structure-guided drug design and candidate drug screening-based strategy. Methods for assessing antiviral activity of test agents include biochemical assays of enzymatic activity and evaluation by cell-based systems20-23. In cell-based systems, the viral life cycle can be dissected into distinct stages of infection, such as entry events (attachment, fusion, uncoating), the replication phase (viral genome replication and protein translation), and virion egress (assembly, maturation, and release). Since the assays can be adapted to investigate each specific stage using various tools and methods, this approach allows identification/examination of potential candidate antivirals with a specific mechanism of action targeting the distinct stage analyzed. For instance, to analyze drug effect specifically on the free virus particles prior to binding to the host cell, a ‘viral inactivation assay’ can be performed. In this assay, the virus is allowed to incubate with the test drug and then diluted to titrate out the drug before infecting a cell monolayer. Additional steps such as viral attachment and entry/fusion stages can also be analyzed individually, by shifting the temperature during the infection. For many enveloped viruses, viral entry/fusion at the host cell membrane is greatly facilitated at 37 °C, but is typically precluded at 4 °C which does not affect virus binding24-29. Finally, the use of reporter viruses or cell systems could facilitate these studies and permit a high-throughput analysis.
We previously employed the cell-based approach and dissected the early entry of various enveloped viruses for the examination of antiviral compounds that potentially antagonize viral entry30,31. Herein, the various methods used, including viral inactivation, viral attachment, and viral entry/fusion assays, are described.
Protokol
Not: hücre kültürü ve virüs enfeksiyonu ile ilgili tüm prosedürler işlenen örneklerin biyogüvenlik düzeyi için uygun olan sertifikalı biyogüvenlik davlumbaz yapılan emin olun. Protokolleri tarif edilmesi amacıyla, Gaussia lusiferaz raportör-etiketli HCV model virüs 32 olarak kullanılır. Temsili sonuçlar bağlamında bileşikler chebulagic asit (chlA) ve punicalagin (PUG) 31 adım erken viral girişi sırasında, hücre yüzeyi glikozaminoglikanların viral glikoprotein etkileşimleri hedef aday antiviral olarak kullanılır. Birçok virüs 30,31,33,34 girişi ile müdahale edilmesi bilinmektedir Heparin, bu bağlamda, bir pozitif kontrol tedavisi olarak kullanılır. Temel viroloji teknikleri arka plan, virüslerinin üretilmesi ile, virüs titresinin belirlenmesi ve plak oluşturucu birim enfeksiyöz doz (PFU) ekspresyonu için, oluşturucu birim (FFU) ya da enfeksiyon (MOI) çokluğu odak okuyucu yeniden olduğu35 referans yönlendirildiler. Önceki örnekler ve temsili sonuçlarda görüldüğü virüs için kullanılan optimum koşullar için okuyucu Tablo 1, Şekil 1A ve Şekil 2A'da yer alan referanslar 30-32,36-39 ve detayları adlandırılır.
1. Hücre Kültürü, Bileşik Hazırlama ve Bileşim Sitotoksisite
- Virüs enfeksiyonu sistemi için ilgili hücre hattı büyütün (Tablo 1) analiz edilecek. HCV için, Dulbecco değiştirilmiş Eagle ortamı,% 10 fetal sığır serumu (FBS) ile desteklenmiş (DMEM), 200 U / ml penisilin G, 200 ug / ml streptomisin içinde Huh-7,5 hücrelerin büyümesine ve 0,5 ug / ml amfoterisin B
- Kendi çözücüler kullanılarak Test bileşikleri ve kontroller hazırlayın: örneğin, chlA ve dimetil sülfoksit içinde PUG (DMSO) çözülür; Steril çifte damıtılmış su içinde heparin hazırlar. Sonraki tüm seyreltilerde için, kültür ortamı kullanın.
Not: Son concentTest bileşiği, tedavi DMSO oranı deneylerde% 1'den az olduğu; % 1 DMSO karşılaştırma deneylerinde, bir negatif kontrol tedavisi olarak dahil edilir. - Örneğin XTT olarak reaktif belirleyici hücre canlılığı ile viral enfeksiyon için hücreler üzerinde test bileşiklerinin (örneğin, chlA ve PUG) sitotoksisitesini belirlemek (2,3-bis [2-metoksi-4-nitro-5-sülfofenil] -5-fenilamino) -karbonil] -2H-tetrazolyum hidroksit):
- HCV için, bir 96-çukurlu plaka içinde Huh-7,5 hücreler (çukur başına 1 x 10 4 hücreleri) tohum ve bir tek tabaka elde etmek üzere% 5 CO2 inkübatöründe O / N 37 ° C'de inkübe edin.
- Üç kopya halinde kültür çukurlarına DMSO kontrolü (% 1) ya da test bileşimleri chlA ve PUG artan konsantrasyonlarda (ör., 0, 10, 50, 100 ve 500 uM) uygulayın.
- Daha sonra, 72 saat süre ile 37 ° C'de inkübe plaka içinde orta atmak ve iki kez fosfat tamponlu tuzlu su içinde 200 ul (PBS) hücreleri yıkayın.
- Assayin 100 ul ekleg her oyuğa XTT tabanlı in vitro toksisite deneyi kiti çözeltisi ve XTT formazan üretimini sağlamak için, başka bir 3 saat daha 37 ° C'de inkübe edin.
- 492 nm dalga boyunda bir test bir mikroplaka okuyucu ve 690 nm'lik bir referans dalga boyu ile absorbans belirler.
- . Test bileşiklerinin absorbans ve solvent kontrolü bakın (ex% 1 DMSO 'gibi'% 100 'At' × gibi / hücre canlılığı (%) At = ve aşağıdaki formül kullanılarak hücrelerin hayatta yüzdesini hesaplayın sırasıyla) tedaviler. Üreticinin protokolüne göre olan, GraphPad Prizmasında gibi bir analitik yazılım test bileşikleri% 50 hücresel sitotoksisite (CC 50) konsantrasyonunu belirler.
Viral Enfeksiyon 2. Saati
Not: viral enfeksiyonun okuma kullanılan virüs sistemine bağlıdır ve plak tahlilleri ya da mea gibi yöntemleri içerebilirmuhabir-etiketli virüslerden muhabiri sinyalleri suring. Lusiferaz raportör etkinliği göre muhabir-HCV enfeksiyonunu belirlemek için bir yöntem aşağıda tarif edilmektedir.
- Enfekte kuyulardan süpernatantlar toplayın ve 4 ° C'de 5 dakika boyunca bir mikrosantrifüj içinde 17,000 xg'de belirler.
- Gaussia lusiferaz deney kiti lusiferaz alt-tabaka, 50 ul test süpernatan 20 ul karıştırın ve, imalatçı firmanın talimatlarına göre, bir lüminometre ile ölçün.
- Üreticinin protokolüne göre, GraphPad Prism yazılımı algoritmaları kullanarak, HCV enfeksiyonuna karşı test bileşiklerinin% 50 etkili konsantrasyon (EC 50), viral inhibisyon (%) belirlemek için, nispi ışık birimleri (RLU) log 10 olarak, HCV enfektivitesini ifade edebilir ve hesaplar.
3. Viral İnaktivasyonu Testi
Not: Çeşitli virüsler için kuluçka süresi örnek olarak ve viral dozunŞekil 1A listelenen yeniden. Virüsün yüksek konsantrasyonlar da MOI / PFU artırarak test edilebilir.
- Tohum Huh-7,5, 96-çukurlu plaka içindeki hücreler (oyuk başına 1 x 10 4 hücreler) ve bir tek tabaka elde etmek üzere bir% 5 CO2 inkübatöründe 37 ° C'de O / N inkübe edin.
- Test bileşikleri veya kontroller inkübe (nihai konsantrasyonlar: chlA = 50 uM; PUG = 50 uM; heparin = 1000 ug / ml; DMSO =% 1) 37 ° C (Şekil 1A HCV partikülleri ile, Uzun Vadeli ' ) bir 1: 1 oranında elde edildi. Örneğin, 1 x 10 4 FFU ihtiva eden bir 100 ul virüs aşı için bir 100 uM chlA çalışma seyreltme 100 ul; Bu 50 uM'lik nihai bir konsantrasyonda chlA tedavi verir.
- Virüs-ilaç karışımı test bileşiklerinin için "alt terapötik" (etkisiz) konsantrasyonu sulandırmak. Örneğin, HCV karşı chlA ve PUG etkisiz konsantrasyonu 1 mcM 31 olan; bu nedenleBu (% 2 FBS ile hücre kültürü ortamı) bazal ortam içinde 9.8 ml ile gerçekleştirilebilir virüs ilaç karışımı bir 50-kat seyreltme gerektirir.
Not: alt terapötik konsantrasyonuna seyreltme test bileşikleri ve konak hücre yüzeyi arasında önemli bir etkileşim önler ve hücre içermeyen viryonları üzerindeki tedavi etkisinin incelenmesine olanak tanır. Bu seyreltme, özellikle viral enfeksiyona karşı test bileşiklerinin anti-viral doz yanıtı bağlıdır, ve bu belirli tahlil 31 gerçekleştirmeden önce belirlenir unutmayın. - Karşılaştırma için, test bileşikleri ile virüs karışımı hemen alt terapötik konsantrasyonu enfeksiyon öncesinde (Şekil 1A 'Kısa Dönem') ila (inkübasyon süresi) seyreltin.
- Ve viral izin vermek için 37 ° C'de 3 saat süreyle inkübe edilir, Huh-7,5 hücre mono tabakasında üzerine seyreltilmiş HCV ilaç karışımı, 100 ul ilave edin (nihai MOI = 0,01 virüs miktarı 1 x 10 2 FFU şimdi de)adsorpsiyon.
- Enfeksiyonu takiben, seyreltilmiş inokulum çıkarıp hafifçe iki kez 200 ul PBS ile kuyu yıkayın.
Not: hücrelerini kaldırarak önlemek için hafifçe yıkar gerçekleştirin. - Her bir oyuğa bazal ortam 100 ul uygulayın ve 72 saat boyunca 37 ° C'de inkübe edin.
- 2 'de tarif edildiği gibi lusiferaz aktivitesi için supernatant analiz etmek sureti ile elde edilen enfeksiyon analiz edin. Viral Enfeksiyon okunması '.
4. Viral ataşman Deneyi
Not: Çeşitli virüsler için kuluçka süresi ve viral doz örnekleri arasında, Şekil 2A'da yer alan 'ataşman' vardır. Virüsün yüksek konsantrasyonlar da MOI / PFU artırarak test edilebilir.
- Tohum Huh-7,5, 96-çukurlu plaka içindeki hücreler (oyuk başına 1 x 10 4 hücreler) ve bir tek tabaka elde etmek üzere bir% 5 CO2 inkübatöründe 37 ° C'de O / N inkübe edin.
- 4 ° C de fo plakalarda hücredeki tekli katmanlara önceden soğukr, 1 saat.
- HCV aşı ile hücreleri (MOI = 0.01) ve test bileşikleri veya kontroller Co-muamele (nihai konsantrasyonlar: chlA = 50 uM; DMSO =% 1 PUG = 50 uM; heparin = 1000 ug / ml) 4 ° C'de 3 saat. Örneğin, 1 x 10 2 FFU ihtiva eden bir 90 ul virüs aşı için, 500 uM chlA çalışma seyreltme 10 ul; Bu chlA 50 uM'lik bir son konsantrasyon elde tedavi ve MOI'da HCV enfeksiyonu = 0.01, hücre tek tabaka elde edilir.
Not: bağlayıcı virüs için izin verir, ancak en verimli 37 ° C'de meydana girişi engeller beri 4 ° C'de deneyi yürütmek için önemlidir. Sıcaklık 4 ° C de muhafaza edilmesini sağlamak için, buz üzerinde virüs ve test bileşiklerinin ilave bir 4 ° C buzdolabında izleyen inkübasyon gerçekleştirin. - Süpernatantı ve yavaşça iki kez buz gibi soğuk 200 ul PBS ile hücre mono tabakasının yıkayın.
Not: hücrelerini kaldırarak önlemek için hafifçe yıkar gerçekleştirin <./ li> - Her bir oyuğa bazal ortam 100 ul uygulayın ve 72 saat boyunca 37 ° C'de inkübe edin.
- 2 'de tarif edildiği gibi lusiferaz aktivitesi için supernatant analiz etmek sureti ile elde edilen enfeksiyon analiz edin. Viral Enfeksiyon okunması '.
5. Viral kayıt / Füzyon Analizi
Not: kuluçka dönemleri ve çeşitli virüsler için viral doz Örnek Şekil 2A 'Giriş / Fusion' listelenmiştir. Virüsün yüksek konsantrasyonlar da MOI / PFU artırarak test edilebilir.
- Tohum Huh-7,5, 96-çukurlu plaka içindeki hücreler (oyuk başına 1 x 10 4 hücreler) ve bir tek tabaka elde etmek üzere bir% 5 CO2 inkübatöründe 37 ° C'de O / N inkübe edin.
- 1 saat süre ile 4 ° C 'de plakalarda hücredeki tekli katmanlara önceden soğuk.
- 3 saat boyunca 4 ° C 'de HCV ile hücreleri (MOI = 0.01) Infect. Örneğin, 1 x 10 2 FFU ihtiva eden bir 100 ul virüs inokulum kullanın.
Not: addin gerçekleştirBuz üzerinde viral inokülüm ve 4 ° C buzdolabı izleyen inkübasyon tion viral bağlanmayı değil girişini sağlayacak 4 ° C'de, bir ısıyı sürdürmek için. - Süpernatantı ve yavaşça iki kez buz gibi soğuk 200 ul PBS ile hücredeki tekli katmanlara yıkayın.
Not: hücrelerini kaldırarak önlemek için hafifçe yıkar gerçekleştirin. - (Nihai konsantrasyonlar:; PUG = 50 uM; heparin = 1000 ug / ml; chlA = 50 uM DMSO =% 1) test bileşikleri veya kontroller ile kuyu tedavi ve 3 saat boyunca 37 ° C'de inkübe edin. Örneğin, ortam 90 ul 500 uM chlA çalışma seyreltme 10 ul karıştırın ve kuyu tedavi; Bu 50 uM'lik nihai bir konsantrasyonda chlA tedavi verir.
Not: 37 ° C, 4 ° C kayma geç viral giriş / füzyon olgusuna kolaylaştırır ve bu nedenle bu özel adım test, bileşiklerin etkisinin değerlendirilmesine olanak sağlamaktadır. - İlacı içeren süpernatant aspire olmayan içselleştirmiş kaldırmaksitrat tamponu (50 mM sodyum sitrat, 4 mM potasyum klorür, pH 3.0) ya da PBS 200 ul ya da yıkama ile hücre dışı virüs. 72 saat boyunca 37 ° C'de inkübe edilmeden önce, bazal ortam 100 ul uygulanır.
- 2 'de tarif edildiği gibi lusiferaz aktivitesi için supernatant analiz etmek sureti ile elde edilen enfeksiyon analiz edin. Viral Enfeksiyon okunması '.
Sonuçlar
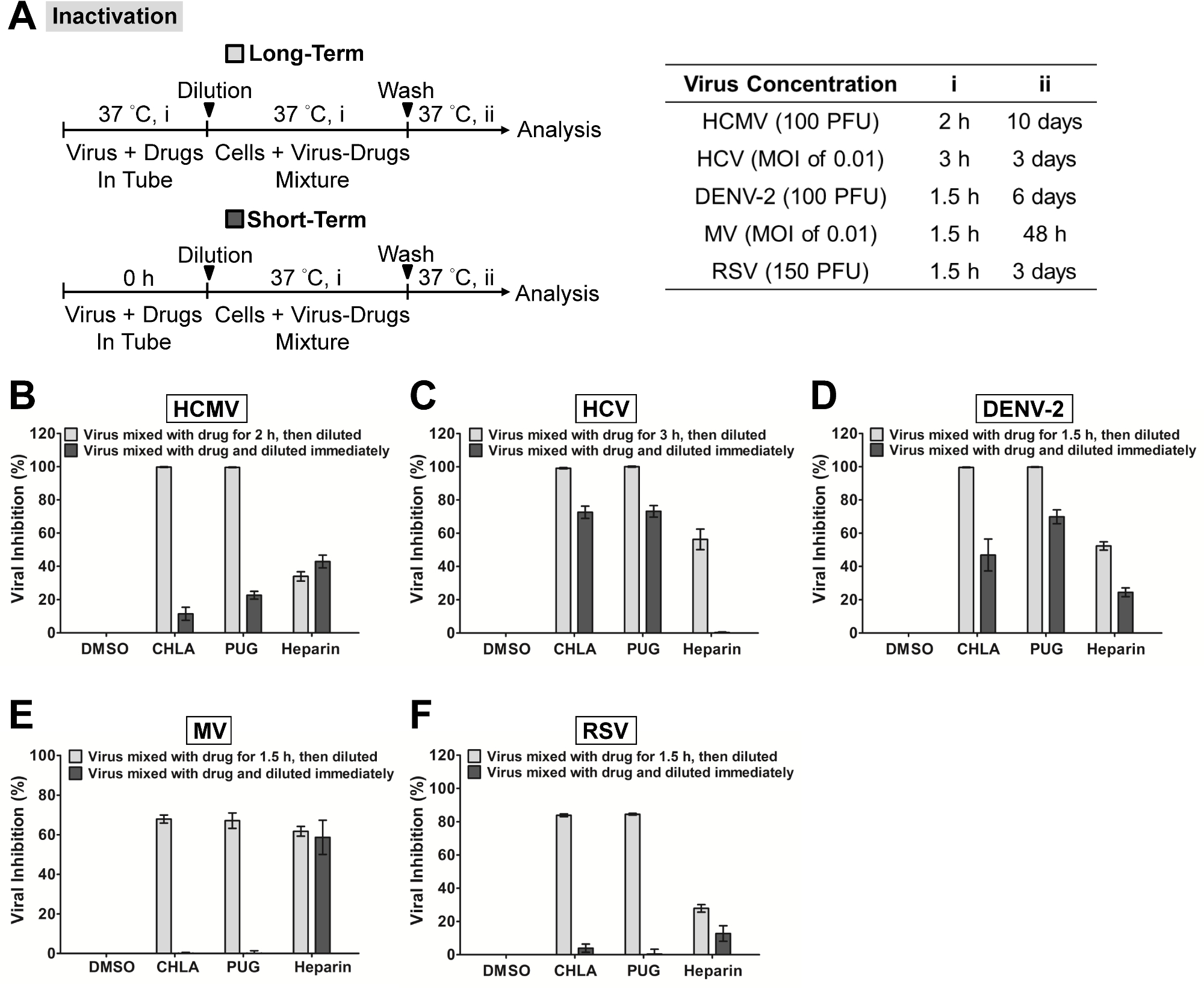
Şekil 1'de, 'viral inaktivasyon deneyi' iki özel doğal bileşikler chlA ve PUG hücre serbest halde farklı zarflı virüsler inaktive ve sonraki enfeksiyonu önlemek olabilir olup olmadığını incelemek için yapıldı. Bu bileşiklerin sitotoksisitesi ve antiviral dozu tepkisi mekanik çalışma 31 gerçekleştirmeden önce tespit edilmiştir. Virüs test bileşikleri ile ön-muamele edilmiştir ve sonra virüs-ilaç karışımları her bir virüs sistemi için ilgili hücre tek tabaka üzerine aşılamadan önce alt terapötik konsantrasyonlarda seyreltilmiştir. Şekil 1 'de gösterildiği gibi, chlA ve PUG hem sonraki enfeksiyona hücre tek katmanının korumalı olmayan etki ile sonuçlanan, hücresiz virionlar ile etkileşim ortaya çıktı. % 80 blok MV ve RSV karşı gözlendi - 60 ise iki test bileşikleri, HCMV, HCV ve DENV-2'ye karşı neredeyse% 100 inhibisyon elde etti. Bu sonuçlar, suggeest chlA ve PUG onları inaktive ve enfektivitesini nötralize ederek bu serbest virüs partikülleri üzerinde doğrudan etkisi olduğunu.
Şekil 2'de, eki ve giriş / füzyon deneyleri HCMV, HCV, NV-2, MV ve RSV bu erken viral giriş ile ilgili olaylara karşı chlA ve PUG etkisini araştırmak amacıyla yapılmıştır. ChlA ve PUG Hem etkili bir ortaya çıkan viral enfeksiyon (: açık gri çubuklar Şekil 2'de, 'Ek') üzerine inhibisyonu ile gösterildiği gibi ilgili konakçı hücre üzerine incelenen virüslerin bağlanmasını engellemiştir. Her iki bileşiğin virüs eki üzerindeki önleyici etkisi, HCMV 'nin (Şekil 2B), HCV (Şekil 2C) karşı benzer, NV-2 (Şekil 2B) ve 90 arasında değişen, RSV (Şekil 2F), -% 100. Öte yandan, PUG tw gelen inhibisyon oranı ile, MV bağlanması (Şekil 2E) karşı chlA daha etkili olduğu ortaya çıktı80 -% 50 arasında değişen o bileşikleri. Birçok virüs girişini HCMV'nin da inhibe eki, NV-2, RSV, reklam MV engellemek için bilinen, ancak HCV karşı daha az etkili oldu kontrolü tedavisi heparin. Bunu takip eden 'viral giriş / füzyon deneyi' chlA ve PUG virüs girdi / füzyon aşamasında kendi faaliyetini muhafaza olup olmadığını inceledik (Şekil 2 'Entry / Fusion': koyu gri çubuklar). İlgili hücre tek tabaka üzerinde% 90 koruyucu etki - 50 verimli, - Yine chlA ve PUG hem etkin bir muayene virüsler (F Şekil 2B) viral giriş / füzyon adımını bozduğu gözlendi. Heparin da kuvvetli inhibe giriş / DENV-2 ve RSV enfeksiyonlarının füzyon, ancak HCMV, HCV ve MV (
| Virüs | Hücre Tipi |
| HCMV | HEL |
| HCV | Huh-7.5 |
| NV-2 | Vero |
| MV | CHO-SLAM |
| RSV | HEp-2 |
Tablo 1:. Viral enfeksiyon için konukçu hücre türü için temsili sonuçlarda tarif edilen her viral enfeksiyon sistemi için kullanılan hücre tipi gösterilir. Hücreleri ile ilgili ilave detaylar referans 31 bulunabilir.

Şekil 1. deney bileşikleri chlA ve PUG viral enfeksiyonların inaktivasyonu farklı virüs uzun bir süre için deney bileşikleri ile muamele edilmiştir. (1.5 inkübe - titrasyon önce 3 saat, hafif gri çubuklar) ya da kısa bir süre (hemen seyreltildi; koyu gri alt terapötik konsantrasyonları bir seyreltme öncesinde 37 ° C 'de çubuklar)yon ve ilgili konakçı hücreler üzerinde enfeksiyonun sonraki analiz. Nihai virüs konsantrasyonu ile (sol tarafta), deney (A) Şeması (PFU / göz veya İB), uzun vadeli bir virüs ilacın inkübasyon süresi, (i), ve (ii) daha sonra inkübasyon süresi sağdaki tabloda her bir virüs için belirlenmiştir. (B) HCMV, (C) HCV için analizler, (D), NV-2 (E) OG, ve (F) RSV her ek panelinde gösterilir. Sonuçlar Üç bağımsız deneyden ortalama (SEM) standart hataları ± araçlar virüsü enfeksiyonunun DMSO negatif kontrol tedavisi ve gösterilen veriler karşı çizilmiştir. Bu rakam referansı 31 modifiye edilmiştir. Bu rakamın büyük halini görmek için lütfen buraya tıklayınız.
{kind=link}

Şekil 2. Virüs eki ve giriş / füzyon karşı test bileşikleri chlA ve PUG antiviral aktiviteleri değerlendirme. (A) gösterilen deney prosedürü, virüs konsantrasyonu (PFU / göz veya İB) ve test bileşikleri ile toplama ve işlem süresi, (i, ii, iii) şemaları ve ilişkili tablolar, her bir virüs için sunulmaktadır. Virüs bağlanma analizi (açık gri çubuklar), farklı hücre tiplerinin mono tabakaları, 1 saat boyunca 4 ° C'de önceden soğutulmuş olan, daha sonra 4 ° C de, ilgili virüsler ve test bileşikleri ile birlikte muamele edilmiş (1,5-3 saat i) daha sonra inkübasyon için inoculates ve test bileşikleri yıkamadan önce (37 ° C, ii) ve virüs enfeksiyonu incelenmesi. Virüs giriş / füzyon analizi (koyu gri çubuklar) olarak, aşılanmış hücre mono tabakaları, 1 saat boyunca 4 ° C'de önceden soğutulmuş ve daha sonra 1.5, 4 ° C de, ilgili virüs ile meydan - 3 saat, (i). Bundan sonra hücreler,yıkandı ve sıcaklık viral giriş / füzyon olgusuna kolaylaştırmak için 37 ° C'ye kaydırılır (ii) 'sırasında ek bir inkübasyon süresi için, test bileşikleri ile muamele edildi. İnkübasyonun sonunda, hücre dışı virüs ya sitrat tampon maddesi (pH 3.0) ya da PBS yıkama ile uzaklaştırılmış ve hücreler virüs bulaşması analizi için, (iii) kuluçkalanmıştır. (B) HCMV, (C) HCV için sonuçlar, (D), NV-2 (E) OG, ve (F) RSV her ek panelinde gösterilir. Veriler, virüs enfeksiyonunun DMSO negatif kontrol tedavisi karşı çizilmiştir ve üç bağımsız deneyden ortalama ± SEM olarak sunulmuştur. Bu rakam referansı 31 modifiye edilmiştir. Bu rakamın büyük halini görmek için lütfen buraya tıklayınız.
{kind=link}
Tartışmalar
In this report the methods to identify and evaluate antiviral compounds based on a mechanistic approach of dissecting the early viral entry events were described. Specifically, the assays allowed us to examine the effect of test compounds on free virus particles, viral attachment, and viral entry/fusion. Critical steps were implemented to distinctly evaluate the drug effect on the specific stage of early viral entry. For instance, in the ‘viral inactivation assay’, the dilution of the virus-drug mixture to sub-therapeutic concentration prevents significant interaction between the test compound and the host cell surface by ‘titrating out’ the drug. This ensures that the inhibitory effect observed on the subsequent infection of the host cell is due to a direct interaction between the test compound and the cell-free virions, rather than an effect from the test compound on host cell membrane or membrane-associated molecules, including viral receptors30. Similarly, the shift in temperature between 4 °C (which allows for virus binding but not entry) and 37 °C (which facilitates virus entry/fusion) in the ‘viral attachment assay’ and ‘viral entry/fusion assay’ are crucial to determine the test compound’s effect on each of these specific events. This is feasible due to the temperature sensitivity of enveloped viruses during these steps in the infection24-29. It is therefore important that the assays are performed at the indicated temperature to ensure the accuracy of the results; for example, by carrying out the experiment on ice to maintain at 4 °C and by placing the sample directly in a 37 °C incubator for the temperature shift. In addition, the use of negative (ex. DMSO solvent for drug preparation) and positive (ex. heparin treatment) controls also help further establish the assays’ accuracy. The utility and applicability of such methods have been demonstrated in many antiviral studies26,30,31,40,41. Note that while heparin is included as a control for all three assays in the context of the representative results, it typically blocks the initial virus binding rather than the ensuing fusion/entry step (as reflected by the data in Figure 2). Additional controls could also be used, such as neutralizing antibodies directed against the virus (for viral inactivation assay), antibodies that mask the cell surface receptors for the virus (for viral attachment assay), and membrane fusion inhibitors (for viral fusion/entry assay).
The assays described in this report, which are specific to the early stages of the viral infection, are useful in terms of application as secondary tests to characterize the mechanism of action of candidate drugs from primary screens which typically target the viral infection more broadly. Alternatively, they could also be incorporated in primary screens if one is specifically looking for inhibitors of early viral entry, including virus inactivating agents, viral attachment antagonists, and inhibitors to viral entry/fusion. In this case, their use allows a more focused and precise screen analysis for the identification of mechanism-specific antiviral candidates, which, in turn, would expedite downstream drug development.
The use of cell-based assays in identifying antiviral agents provides several important advantages compared to biochemical assays, including revealing potential off-target effects (such as cytotoxicity) and adding physiological relevance to the bioactivity of the test agents42. These issues are important considerations for deciding whether a candidate agent is of value for continuation in subsequent phases of drug development. Similarly, the early viral entry-specific assays described in this report allow examination of the drug effect on the distinct viral entry stage at the cellular level, and more specifically in the context of an authentic viral infection in vitro. The results obtained from such assays would therefore help better predict the antiviral efficacy of the test compounds and also identify potentially unwanted off-target effects against the host cell. One potential limitation though, is that an in vitro cell-based assay may not completely reflect the actual in vivo entry step in the context of a natural viral infection. Nonetheless, the assays presented in this protocol do serve as an analytical platform for mechanism-based identification and evaluation of novel antiviral agents.
The development of reporter viruses or reporter cell systems to quantitate the amount of viral infection has greatly facilitated cell-based screening and evaluation of antiviral compounds. Examples include the use of recombinant viruses carrying a reporter gene or by means of recombinant human cell lines containing a reporter gene driven by the specific virus promoter31,43. In this report, the infection from luciferase-tagged HCV can be easily monitored by quantitating the reporter signal, thus facilitating data analysis. By incorporating these useful reporter-based tools, the early viral entry assays described here can essentially be adapted into high-throughput format for mechanism-based screening of small molecule libraries.
In conclusion, a protocol was described for assays dissecting the early viral entry as a means of identifying and evaluating mechanism-specific antiviral compounds. Such assays would be useful for discovering novel antagonists/inhibitors to viral entry and help expand the scope of antiviral agents for development as prophylactic and/or therapeutic treatments.
Açıklamalar
The authors declare that no competing interests exist.
Teşekkürler
This study is supported by funding from Taipei Medical University Hospital (102TMU-TMUH-19) and the Ministry of Science and Technology of Taiwan (MOST103-2320-B-038-031-MY3).
Malzemeler
| Name | Company | Catalog Number | Comments |
| DMEM | GIBCO | 11995-040 | |
| FBS | GIBCO | 26140-079 | |
| Penicillin-Streptomycin | GIBCO | 15070-063 | |
| Amphotericin B | GIBCO | 15290-018 | |
| DMSO | Sigma | D5879 | |
| In vitro toxicology assay kit, XTT-based | Sigma | TOX2 | |
| PBS pH 7.4 | GIBCO | 10010023 | |
| Microplate reader | Thermo Scientific | 89087-320 | |
| Microcentrifuge | Thermo Scientific | 75002420 | |
| BioLux Gaussia luciferase assay kit | New England Biolabs | E3300L | |
| Luminometer | Promega | GloMax-20/20 | |
| Sodium citrate, dihydrate | Sigma | 71402 | |
| Potassium chloride | Sigma | P5405 |
Referanslar
- Munier, C. M., Andersen, C. R., Kelleher, A. D. HIV vaccines: progress to date. Drugs. 71, 387-414 (2011).
- Rothman, A. L. Immunity to dengue virus: a tale of original antigenic sin and tropical cytokine storms. Nat Rev Immunol. 11, 532-543 (2011).
- Sung, H., Schleiss, M. R. Update on the current status of cytomegalovirus vaccines. Expert Rev Vaccines. 9, 1303-1314 (2010).
- Torresi, J., Johnson, D., Wedemeyer, H. Progress in the development of preventive and therapeutic vaccines for hepatitis C virus. J Hepatol. 54, 1273-1285 (2011).
- Wright, M., Piedimonte, G. Respiratory syncytial virus prevention and therapy: past, present, and future. Pediatr Pulmonol. 46, 324-347 (2011).
- Christou, L. The global burden of bacterial and viral zoonotic infections. Clin Microbiol Infect. 17, 326-330 (2011).
- Cascio, A., Bosilkovski, M., Rodriguez-Morales, A. J., Pappas, G. The socio-ecology of zoonotic infections. Clin Microbiol Infect. 17, 336-342 (2011).
- Grais, R. F. Measles vaccination in humanitarian emergencies: a review of recent practice. Confl Health. 5, 21 (2011).
- Gautret, P. Emerging viral respiratory tract infections-environmental risk factors and transmission. Lancet Infect Dis. 14, 1113-1122 (2014).
- Sampathkumar, P. Middle East respiratory syndrome: what clinicians need to know. Mayo Clin Proc. 89, 1153-1158 (2014).
- Burd, E. M. Ebola Virus: a Clear and Present Danger. J Clin Microbiol. 53, 4-8 (2015).
- Bishop, B. M. Potential and Emerging Treatment Options for Ebola Virus Disease. Ann Pharmacother. , (2014).
- Arduino, P. G., Porter, S. R. Oral and perioral herpes simplex virus type 1 (HSV-1) infection: review of its management. Oral Dis. 12, 254-270 (2006).
- Mitrasinovic, P. M. Advances in the structure-based design of the influenza A neuraminidase inhibitors. Curr Drug Targets. 11, 315-326 (2010).
- Soriano, V. Directly acting antivirals against hepatitis C virus. J Antimicrob Chemother. 66, 1673-1686 (2011).
- Haqqani, A. A., Tilton, J. C. Entry inhibitors and their use in the treatment of HIV-1 infection. Antiviral Res. 98, 158-170 (2013).
- Melby, T., Westby, M. Inhibitors of viral entry. Handb Exp Pharmacol. , 177-202 (2009).
- Vanderlinden, E., Naesens, L. Emerging antiviral strategies to interfere with influenza virus entry. Med Res Rev. 34, 301-339 (2014).
- Antoine, T. E., Park, P. J., Shukla, D. Glycoprotein targeted therapeutics: a new era of anti-herpes simplex virus-1 therapeutics. Rev Med Virol. 23, 194-208 (2013).
- Pawlotsky, J. M., Chevaliez, S., McHutchison, J. G. The hepatitis C virus life cycle as a target for new antiviral therapies. Gastroenterology. 132, 1979-1998 (2007).
- Beyleveld, G., White, K. M., Ayllon, J., Shaw, M. L. New-generation screening assays for the detection of anti-influenza compounds targeting viral and host functions. Antiviral Res. 100, 120-132 (2013).
- Kilianski, A., Baker, S. C. Cell-based antiviral screening against coronaviruses: developing virus-specific and broad-spectrum inhibitors. Antiviral Res. 101, 105-112 (2014).
- Caillet-Saguy, C., Lim, S. P., Shi, P. Y., Lescar, J., Bressanelli, S. Polymerases of hepatitis C viruses and flaviviruses: structural and mechanistic insights and drug development. Antiviral Res. 105, 8-16 (2014).
- Frey, S. Temperature dependence of cell-cell fusion induced by the envelope glycoprotein of human immunodeficiency virus type 1. J Virol. 69, 1462-1472 (1995).
- Tscherne, D. M. Time- and temperature-dependent activation of hepatitis C virus for low-pH-triggered entry. J Virol. 80, 1734-1741 (2006).
- Madan, R. P. Molecular umbrellas: a novel class of candidate topical microbicides to prevent human immunodeficiency virus and herpes simplex virus infections. J Virol. 81, 7636-7646 (2007).
- Haywood, A. M., Boyer, B. P. Time and temperature dependence of influenza virus membrane fusion at neutral pH. J Gen Virol. 67 (Pt 12), 2813-2817 (1986).
- Haywood, A. M., Boyer, B. P. Sendai virus membrane fusion: time course and effect of temperature, pH, calcium, and receptor concentration). Biochemistry. 21, 6041-6046 (1982).
- Wang, G., Hernandez, R., Weninger, K., Brown, D. T. Infection of cells by Sindbis virus at low temperature. Virology. 362, 461-467 (2007).
- Lin, L. T. Hydrolyzable tannins (chebulagic acid and punicalagin) target viral glycoprotein-glycosaminoglycan interactions to inhibit herpes simplex virus 1 entry and cell-to-cell spread. J Virol. 85, 4386-4398 (2011).
- Lin, L. T. Broad-spectrum antiviral activity of chebulagic acid and punicalagin against viruses that use glycosaminoglycans for entry. BMC Microbiol. 13, 187 (2013).
- Marukian, S. Cell culture-produced hepatitis C virus does not infect peripheral blood mononuclear cells. Hepatology. 48, 1843-1850 (2008).
- Baba, M., Snoeck, R., Pauwels, R., de Clercq, E. Sulfated polysaccharides are potent and selective inhibitors of various enveloped viruses, including herpes simplex virus, cytomegalovirus, vesicular stomatitis virus, and human immunodeficiency virus. Antimicrob Agents ChemotheR. 32, 1742-1745 (1988).
- Barth, H. Cellular binding of hepatitis C virus envelope glycoprotein E2 requires cell surface heparan sulfate. J Biol CheM. 278, 41003-41012 (2003).
- Flint, S. J., Enquist, L. W., Racaniello, V. R., Skalka, A. M. . Principles of Virology. , (2008).
- Brown, M. G. Dramatic caspase-dependent apoptosis in antibody-enhanced dengue virus infection of human mast cells. J Leukoc Biol. 85, 71-80 (2009).
- Huang, Y., Cyr, S. L., Burt, D. S., Anderson, R. Murine host responses to respiratory syncytial virus (RSV) following intranasal administration of a Protollin-adjuvanted, epitope-enhanced recombinant G protein vaccine. J Clin Virol. 44, 287-291 (2009).
- Isaacson, M. K., Compton, T. Human cytomegalovirus glycoprotein B is required for virus entry and cell-to-cell spread but not for virion attachment, assembly, or egress. J Virol. 83, 3891-3903 (2009).
- Leonard, V. H., et al. Measles virus blind to its epithelial cell receptor remains virulent in rhesus monkeys but cannot cross the airway epithelium and is not shed. J Clin Invest. 118, 2448-2458 (2009).
- Ciesek, S. The green tea polyphenol, epigallocatechin-3-gallate, inhibits hepatitis C virus entry. Hepatology. 54, 1947-1955 (2011).
- Lin, L. T. Saikosaponin b2 is a naturally occurring terpenoid that efficiently inhibits hepatitis C virus entry. J Hepatol. 62, 541-548 (2015).
- Atkins, C., Evans, C. W., White, E. L., Noah, J. W. Screening methods for influenza antiviral drug discovery. Expert Opin Drug Discov. 7, 429-438 (2012).
- Zhang, J. Identification of novel virus inhibitors by influenza A virus specific reporter cell based screening. Antiviral Res. 93, 48-54 (2012).
Yeniden Basımlar ve İzinler
Bu JoVE makalesinin metnini veya resimlerini yeniden kullanma izni talebi
Izin talebiThis article has been published
Video Coming Soon
JoVE Hakkında
Telif Hakkı © 2020 MyJove Corporation. Tüm hakları saklıdır