Systemic Treatment for Postnatal, Juvenile, and Runted Adult Mice by Retrobulbar Sinus Injection
In This Article
Summary
This article provides a protocol and an accompanying video for the retrobulbar sinus injection of up to a total volume of 150 µL for postnatal, juvenile, and runted adult mice. This procedure is particularly well suited for the injection of small mice (15 g) when tail vein injection is not feasible.
Abstract
While tail vein injections are frequently used as a systemic route of delivery in adult mice, retrobulbar injections are an alternative method for systemic delivery with fewer limitations. First, tail vein injections (TVIs) are limited to adult mice where the size of the tail vein is suitable for access. Being restricted to treating adult mice can be problematic when dealing with mouse models that do not survive to adulthood. Second, TVIs are not feasible for mouse models with growth retardation phenotypes where the mice never achieve the size of adult wildtype mice. Therefore, retrobulbar injections can be successfully used to treat both young and small adult mice. Lastly, retrobulbar injections are performed under anesthesia, which is less stressful on the mice than TVIs that are commonly performed without anesthesia. This article presents a protocol and detailed instructions for retrobulbar injections that can be used for systemic delivery to small and young mice.
Introduction
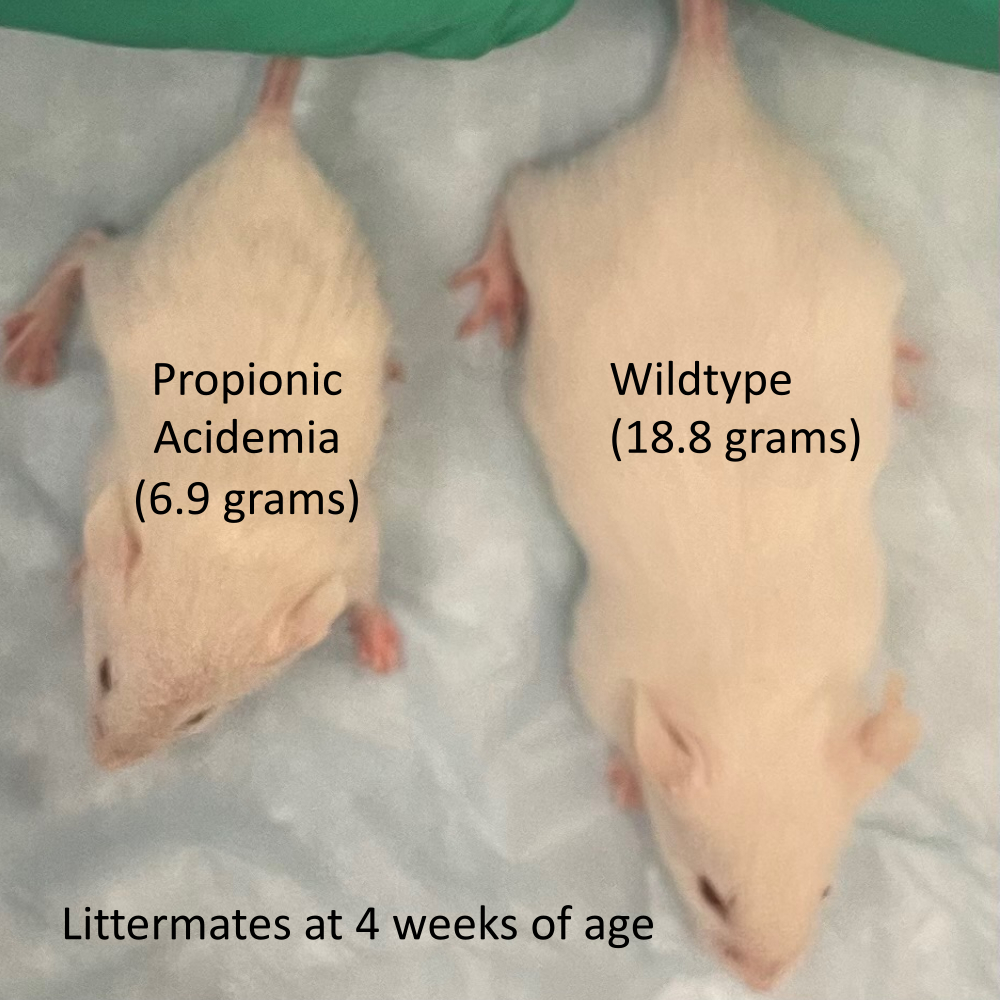
Murine models of genetic diseases are commonly used to demonstrate the efficacy of small molecule, genetic, and cell therapies1. In mice, the most widely used method to replicate systemic delivery to humans is the tail vein injection (TVI), which is typically performed in adult mice at approximately 6-8 weeks of age to ensure the vein is large enough to access. TVI has been successfully used in numerous preclinical proof-of-principle studies of genetic diseases, such as hemophilia, that have supported human clinical trials for gene therapy2. However, many murine models of genetic disease have growth and/or early lethality phenotypes, which prevent them from reaching the age or size of an adult mouse (Figure 1). Treating such mice via TVI can be extremely difficult, if not impossible, depending on the age of lethality and/or the maximum size the animals can achieve.
In contrast, systemic delivery of a therapeutic agent by retrobulbar (frequently and incorrectly referred to as retro-orbital) sinus injection can be done quite readily in mice regardless of age or size3. Retrobulbar injections of adeno-associated virus (AAV) have been used successfully in young growth-retarded murine models of genetic disease, such as methylmalonic acidemia (MMA) and Niemann-Pick type C disease4,5,6,7,8. (This procedure can also be used to inject neonates3,4,9,10; however, this technique is not detailed in this protocol or the accompanying video.) Even highly toxic substances like doxorubicin can be delivered safely by retrobulbar injection11,12. Unlike TVI, mice are anesthetized during retrobulbar sinus injections, which makes the procedure less stressful on the mouse and easier on the operator who does not have to physically restrain the mouse13,14. An additional concern is that TVI frequently use a heat lamp to dilate the tail vein, which could potentially cause dehydration in young mice and could be problematic in murine models of genetic disease that are more suspectable to heat-related stress. Another problem that can arise when using TVI is that the tail vein can be particularly challenging to visualize on highly pigmented mice. However, like TVI, retrobulbar sinus injections result in a wide systemic biodistribution15,16.
Protocol
This protocol and the accompanying video are for the retrobulbar injection space of postnatal, juvenile, and runted adult mice by retrobulbar sinus injection; the protocol has been approved by the National Human Genome Research Institute's Institutional Animal Care and Use Committee (ACUC) under protocol number G-03-4. Other institutions may have different requirements and restrictions, and this protocol may need to be modified for approval in your institute. Obtain approval from your institution's ACUC before performing this or any other animal procedure.
1. Pre-injection preparation
- Dilute the AAV to the desired injection volume and concentration with sterile phosphate-buffered saline (PBS) in a sterile 1.5 mL microcentrifuge tube for each injection. Add an extra 50% volume for each injection to allow for accurate filling of the single-use sterile syringe.
NOTE: Here we are diluting an AAV8-CAG-eGFP reporter to deliver a dose of 1 × 1013viral genomes per kg of body mass (vg/kg) in a volume of 50 μL. The amount of AAV in the 50 μL to be injected is calculated using the weight of the animal at the time of injection. In this video, AAV is being injected via the retrobulbar route to replicate systemic delivery in humans. Other gene therapy vectors (i.e., lentivirus, adenovirus), RNA therapies, and small molecules can be delivered systemically using this procedure. - Ensure that the table-top laboratory animal anesthesia system (LAAS) is properly set up and functioning correctly in accordance with the manufacturer's instructions.
NOTE: If an alternative anesthesia method is used, ensure that anethesia is prepared prior to beginning injections. The retrobulbar injection procedure should be compatible with most anesthesias (e.g., an injectable chemical restraint like ketamine and xylazine). - Prior to filling the single-use sterile syringe (here, an insulin syringe, 31 G, 8 mm long, 3/10 mL capacity), move the plunger up and down several times to ensure the plunger can be depressed smoothly. Then, fill the syringe to the desired volume, ensuring there are no air bubbles.
NOTE: Volumes up to 150 µL can be injected; our lab typically injects a volume of 50 µL.
2. Mouse sedation via administration of isoflurane gas with a laboratory animal anesthesia system (LAAS)
- Ensure that gas is only flowing to the induction chamber. Close the two-way stopcock to the non-rebreathing (NRB) circuit.
- Turn on the green oxygen flow knob on the front of the flow meter so that there is a flow rate of 1 L/min.
- Turn isoflurane to ≤4% by depressing the lever at the top of the vaporizer and turning the dial to the desired concentration.
- Place the mouse in the clear induction chamber. Watch the animal's breathing and movement carefully. Once the animal is recumbent, turn the vaporizer knob down to 2-2.5% of isoflurane.
- Open the two-way stopcock to the NRB circuit attached to the face mask and close the gas flow to the induction box.
- Remove the animal and place it in the NRB circuit's face mask.
- Turn down the isoflurane concentration setting to 1.5%-1.75%, as determined by reaction to stimuli (e.g., toe-pinch or paw-squeeze).
- Always continuously monitor the mouse's breathing and mucous membrane color (if possible). If the animal's breathing becomes labored or the mucous membrane color is not pink, turn down the anesthetic concentration.
- Keep the animal warm throughout the entire procedure. Use a handwarmer wrapped in a paper towel that is placed underneath the underpad and located directly underneath the mouse.
- Turn off the oxygen and the vaporizer after completion of the procedure.
3. Injection of the animal
- If right-handed, inject the mouse's right eye and position the mouse on its left side with the snout pointing towards the right hand. If left-handed, inject the mouse's left eye and position the mouse on its right side with the snout pointing towards the left hand.
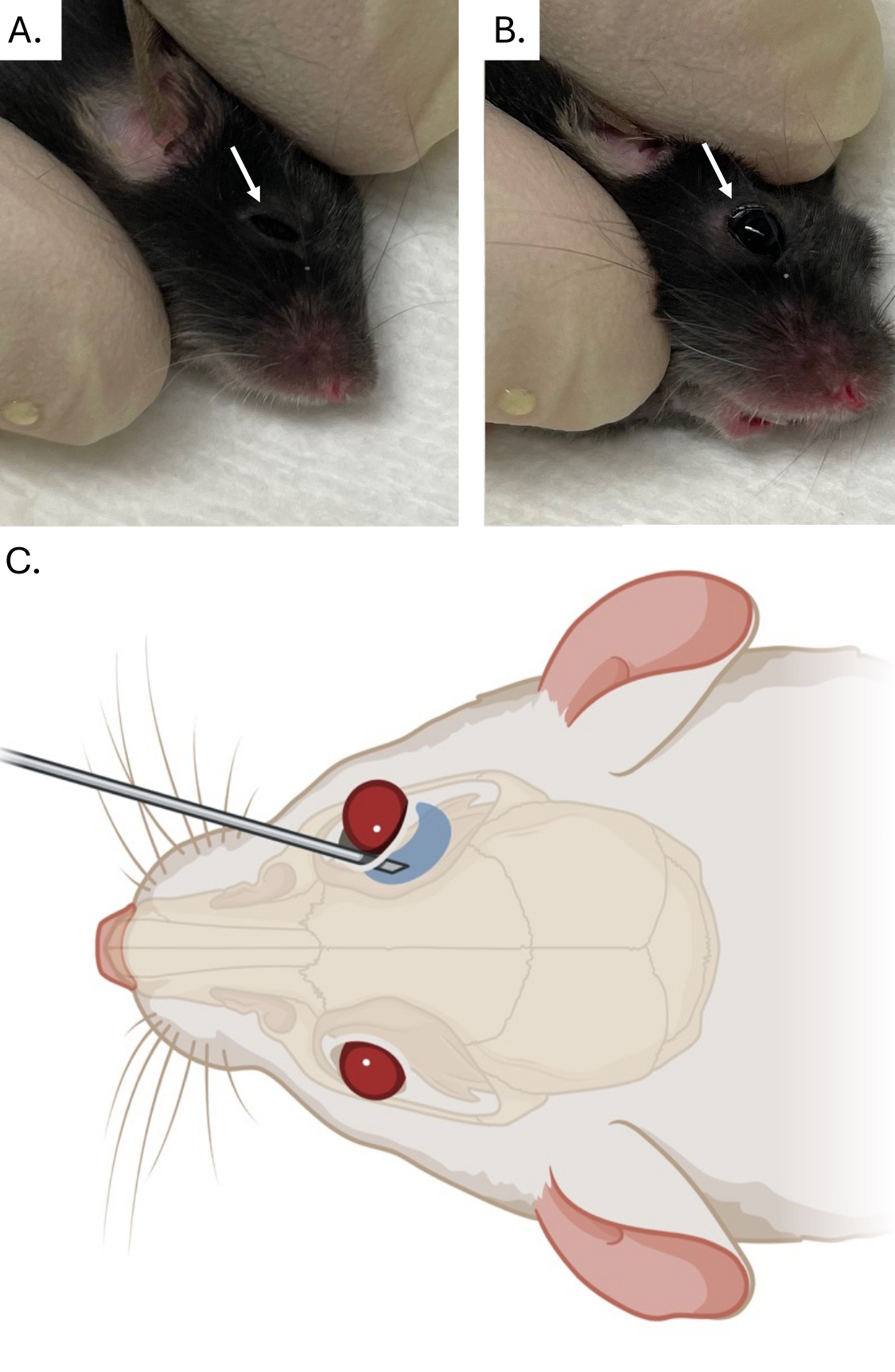
- Apply one or two drops of ophthalmic anesthetic to the eyeball, which is to be injected. Then, remove any excess ophthalmic anesthetic solution using a sterile absorbent gauze pad. Apply gentle pressure with fingertips to the skin dorsal and ventral to the eye to partially protrude the mouse's eyeball from the socket (Figure 2A,B).
NOTE: Be careful not to apply excessive pressure to surrounding cervical vessels when protruding the eye as this will impede blood flow and injection. In addition, applying pressure to the trachea could prevent the mouse from breathing. Ensure the mouse can breathe throughout the procedure. - Keep the needle in a bevel-down position at an angle of approximately 30° and placed into the medial canthus (Figure 2C).
NOTE: The depth of the needle placement to reach the retrobulbar sinus will vary based on the size of the animal. Having the needle in the bevel-down position during the injection decreases the risk of ocular damage. Be careful not to place the needle too deep and puncture the eye socket. The injection should take less than a minute. - Slowly and smoothly apply pressure to the syringe plunger to deliver the injectate. This will reduce the chance of extravasation.
- Remove the needle slowly and smoothly.
- Remove the face mask from the mouse to allow for recovery from anesthesia.
4. Post injection
- Turn off the oxygen and the vaporizer after completion of the procedure.
- Use sterile gauze to remove blood if residual bleeding occurs.
- Ensure the mouse is in a warm area (approximately 37 °C), but not excessively hot, to prevent hypothermia during recovery from anesthesia.
- Observe the mouse in isolation until completely recovered before returning the mouse to the cage and rack.
NOTE: Isolating the mouse during recovery prevents cage mates from injuring the sedated mouse during recovery.
Representative Results
Retrobulbar sinus injection has been used successfully to systemically deliver small molecules, antibodies, and adeno-associated virus (AAV)4,5,9,15,16. In Figure 3, the liver of a PBS (vehicle)-treated mouse and an AAV8-treated mouse liver are shown as an example of AAV injection and expression following a retrobulbar injection. AAV8, like many naturally occurring AAV vectors, is liver trophic. Therefore, substantial liver transduction is expected in a mouse that received a systemic dose of 5 × 1012vg/kg17. The large number of hepatocytes expressing methylmalonyl-CoA mutase (MMUT) RNA seen in Figure 3, which is being expressed by the AAV transgene, indicates a successful retroorbital injection.

Figure 1: A growth retarded mouse with propionic acidemia. This is an example of the extreme growth retardation that can occur in murine models of genetic disease. Please click here to view a larger version of this figure.
{kind=link}

Figure 2: Images and diagram of retrobulbar sinus injection. (A) Image of finger placement on fur to protrude eyeball (indicated by white arrow). (B) Image of eyeball (indicated by white arrow) protrusion after application of downward pressure on the fur prior to needle placement and injection. (C) Diagram of needle bevel orientation (bevel down relative to eyeball), needle angle (30°), and retrobulbar sinus needle placement. Please click here to view a larger version of this figure.
{kind=link}

Figure 3: RNA in situ hybridization after retrobulbar sinus Injection with AAV8. Images of (A) 10x vehicle-treated liver, (B) 10x AAV8-treated liver, (C) 20x vehicle-treated liver, and (D) 20x AAV8-treated liver stained for MMUT RNA. Mice with methylmalonic acidemia were treated with a dose of 5 × 1012 vg/kg of AAV8-LPS-MMUT or a vehicle control (PBS) at 1 month of age. Liver tissue was collected 1 month post treatment. MMUT RNA stained brown (black arrows indicate areas of positive staining). Liver counterstained with hematoxylin. Scale bars = 100 µm 10x for images, 50 µm for 20x images (B). Abbreviations: AAV = adeno-associated virus; LPS = Liver-specific promoter; MMUT = methylmalonyl-CoA mutase. Please click here to view a larger version of this figure.
{kind=link}
Discussion
While retrobulbar injection is a reliable method to deliver small molecules, proteins, and genomic therapies, practicing the technique with a dye is necessary to ensure that reliable and replicable systemic delivery is achieved. The use of a dye is highly recommended for practicing retrobulbar injections in mice before using this delivery route in experiments. Dyes can be visually checked in the mouse tissues to ensure consistent systemic delivery.
In our demonstration of the retrobulbar injection technique, isoflurane gas was used to anesthetize the mice prior to the procedure. Other forms of anesthesia can be used prior to the procedure, but it is important to ensure that the mouse does not recover from the sedation before the injection is completed. Fortunately, the actual injection usually takes less than a minute and the time for which the mouse needs to be fully anesthetized is brief. The mouse should be completely sedated during the injection, and anesthesia should be readministered if the mouse becomes conscious prior to the injection. Since there are risks associated with using anesthesia, the duration of time the mouse is sedated should be minimized. We have not had issues using isoflurane to sedate small sick mice with methylmalonic and propionic acidemia. However, some mouse models may be more sensitive to sedation and certain anesthesia. This potential problem should be considered prior to attempting to use sedation in a study. Lastly, the use of sedation in combination with the retrobulbar injection greatly reduces the apparent distress the mouse exhibits during the injection process in comparison to TVI where sedation is not commonly used.
We have not observed any postinjection-related issues, although infection is a potential risk with any injection. To reduce the chance of infection a sterile single-use disposable syringe and sterile PBS to dilute the purified AAV are used. All mice in our animal facility are checked daily for signs of potential health issues and receive veterinary care to address any health issues when warranted.
The alternative to retrobulbar sinus injection and the more widely used method of systemic delivery to juvenile and adult mice is TVI. TVI and retrobulbar sinus injection result in a similar biodistribution in the case of small molecules and antibodies, and by extrapolation, the same would be expected for viral vectors15,16. However, no examples comparing the systemic delivery of gene therapy vectors by TVI and retrobulbar sinus injection could be found in the literature. In our opinion, retrobulbar sinus injections are easier to perform in mice with a decreased growth phenotype and/or early lethality.
TVI is often considered to be more analogous to systemic delivery in humans, despite humans having a retrobulbar sinus but not having a tail. In one aspect, the retrobulbar sinus injection is like human systemic delivery in that the injectant enters the upper venous system the same as if an injectant was delivered to a human by a peripherally inserted central catheter (PICC Line) or an intravenous catheter placed in the arm. Conversely, the injectant enters the lower venous system of a mouse after tail vein injection. Unfortunately, neither one of these methods exactly replicates the method(s) used for systemic delivery in humans, but both are effective methods of systemic delivery in mice.
Disclosures
The authors have nothing relevant to this publication to disclose.
Acknowledgements
We appreciate the assistance of the NHGRI mouse facility staff, the NCI Molecular Pathology Lab, and especially Andrew Warner. R.J.C. is supported by the Intramural Research Program of the NHGRI through 1ZIAHG200318-16 and this work was partially funded by the National Center for Advancing Translational Sciences (NCATS). Figure 2C was created with BioRender.
Materials
| Name | Company | Catalog Number | Comments |
| AAV8-CAG-eGFP | Univ. Penn. Vector Core | Special order | alternative sources of AAV reporters and alternative AAV reporters are available |
| Barrier (Filter) Tips, 20 μL size | ThermoFisher | AM12645 | for diluting AAV to disire injection volume and concentration |
| Barrier (Filter) Tips, 100 μL size (sterile) | ThermoFisher | AM12648 | for diluting AAV to disire injection volume and concentration |
| Dual Prodedure Circuit | VetEquip | 921400 | alternative anesthesia method can be used |
| Gilsen PIPETTEMAN Classic P20 pipette | Gilson | F123600 | for diluting AAV to disire injection volume and concentration |
| Gilsen PIPETTEMAN Classic P100 pipette | Gilson | F123615 | for diluting AAV to disire injection volume and concentration |
| Hand warmers (HOTHANDS) | ULINE | S-1497B | to keep mouse warm while anesthesized |
| Insulin syringes, 31 G, 8 mm length, 3/10 mL capacity | Becton Dickson | 328438 | used in video; one syringe per injection |
| Isoflurane (Fluriso) | VETONE | 502017 | alternative anesthesia can be used |
| Medline Protection Plus Disposable Underpads | ThermoFisher | 23-666-062 | to place mouse on durring injection |
| Oak Ridge Phlebotomy Sharps Container With Transparent Lid | ThermoFisher | 22-730-434 | for needle disposal |
| Phosphate buffered saline PBS, pH 7.4 | Gibco | 10010023 | To dilute AAV to desired concencentration and volume |
| Snap Cap Low Retention Microcentrifuge Tubes (sterile) | ThermoFisher | 3451 | for diluting AAV to disire injection volume and conentration |
| Sterile gauze sponge 4"x"4 | Covidien | 3033 | |
| Table-Top laboratory animal anesthesia system (LAAS) | VetEquip | 901806 | alternative anesthesia method can be used |
| Trecaine Hydrochloride Ophthalmic (0.5%) | Ocenanside Pharmaceuticals | AK102D5DS | local anesthetic |
| Tuberculin syringe with a 27.0 G (or smaller) | Any | N/A | alternative to insulin syringe used in video |
| VetEquip’s User Guide and Operating Manual for table top and mobile Laboratory Animal Anesthesia System. | VetEquip | chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://www.vetequip.com/pdfs/LAAS%20Manual.pdf | link to users guide and manual |
References
- Perlman, R. L. Mouse models of human disease: An evolutionary perspective. Evol Med Public Health. 2016 (1), 170-176 (2016).
- Samelson-Jones, B. J., George, L. A. Adeno-associated virus gene therapy for hemophilia. Annu Rev Med. 74, 231-247 (2023).
- Yardeni, T., Eckhaus, M., Morris, H. D., Huizing, M., Hoogstraten-Miller, S. Retrobulbar injections in mice. Lab Anim (NY). 40 (5), 155-160 (2011).
- Chandler, R. J., et al. Systemic gene therapy for methylmalonic acidemia using the novel adeno-associated viral vector 44.9. Mol Ther Methods Clin Dev. 27, 61-72 (2022).
- Chandler, R. J., et al. Systemic aav9 gene therapy improves the lifespan of mice with niemann-pick disease, type c1. Hum Mol Genet. 26 (1), 52-64 (2017).
- Venturoni, L. E., et al. Growth advantage of corrected hepatocytes in a juvenile model of methylmalonic acidemia following liver directed adeno-associated viral mediated nuclease-free genome editing. Mol Genet Metab. 137 (1-2), 1-8 (2022).
- Ilyinskii, P. O., et al. Immtor nanoparticles enhance aav transgene expression after initial and repeat dosing in a mouse model of methylmalonic acidemia. Mol Ther Methods Clin Dev. 22, 279-292 (2021).
- Davidson, C. D., et al. Improved systemic aav gene therapy with a neurotrophic capsid in niemann-pick disease type c1 mice. Life Sci Alliance. 4 (10), e202101040 (2021).
- Chandler, R. J., et al. Systemic gene therapy using an aav44.9 vector rescues a neonatal lethal mouse model of propionic acidemia. Mol Ther Methods Clin Dev. 30, 181-190 (2023).
- Rocha-Ferreira, E., et al. A neonatal rodent model of retroorbital vein injection. J Vis Exp. (204), e65386 (2024).
- Bohnert, B. N., Artunc, F. Induction of nephrotic syndrome in mice by retrobulbar injection of doxorubicin and prevention of volume retention by sustained release aprotinin. J Vis Exp. (135), e57642 (2018).
- Bohnert, B. N., et al. Retrobulbar sinus injection of doxorubicin is more efficient than lateral tail vein injection at inducing experimental nephrotic syndrome in mice: A pilot study. Lab Anim. 53 (6), 564-576 (2019).
- Meijer, M. K., Spruijt, B. M., Van Zutphen, L. F., Baumans, V. Effect of restraint and injection methods on heart rate and body temperature in mice. Lab Anim. 40 (4), 382-391 (2006).
- Nohara, M., Tohei, A., Sato, T., Amao, H. Evaluation of response to restraint stress by salivary corticosterone levels in adult male mice. J Vet Med Sci. 78 (5), 775-780 (2016).
- Schoch, A., Thorey, I. S., Engert, J., Winter, G., Emrich, T. Comparison of the lateral tail vein and the retro-orbital venous sinus routes of antibody administration in pharmacokinetic studies. Lab Anim (NY). 43 (3), 95-99 (2014).
- Steel, C. D., Stephens, A. L., Hahto, S. M., Singletary, S. J., Ciavarra, R. P. Comparison of the lateral tail vein and the retro-orbital venous sinus as routes of intravenous drug delivery in a transgenic mouse model. Lab Anim (NY). 37 (1), 26-32 (2008).
- Zincarelli, C., Soltys, S., Rengo, G., Rabinowitz, J. E. Analysis of aav serotypes 1-9 mediated gene expression and tropism in mice after systemic injection. Mol Ther. 16 (6), 1073-1080 (2008).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
ABOUT JoVE
Copyright © 2025 MyJoVE Corporation. All rights reserved