
Peripheral Vascular Exam
Обзор
Source: Joseph Donroe, MD, Internal Medicine and Pediatrics, Yale School of Medicine, New Haven, CT
The prevalence of peripheral vascular disease (PVD) increases with age and is a significant cause of morbidity in older patients, and peripheral artery disease (PAD) is associated with cardiovascular and cerebrovascular complications. Diabetes, hyperlipidemia, hypertension, and tobacco use are important disease risk factors. When patients become symptomatic, they frequently complain of limb claudication, defined as a cramp-like muscle pain that worsens with activity and improves with rest. Patients with chronic venous insufficiency (CVI) often present with lower extremity swelling, pain, skin changes, and ulceration.
While the benefits of screening asymptomatic patients for PVD are unclear, physicians should know the proper exam technique when the diagnosis of PVD is being considered. This video reviews the vascular examination of the upper and lower extremities and abdomen. As always, the examiner should use a systematic method of examination, though in practice, the extent of the exam a physician performs depends on their suspicion of underlying PVD. In a patient who has or is suspected to have risk factors for vascular disease, the vascular exam should be thorough, beginning with inspection, followed by palpation, and then auscultation, and it should include special maneuvers, such as determining the ankle brachial index. Maneuvers that make use of a handheld Doppler are demonstrated in a companion video.
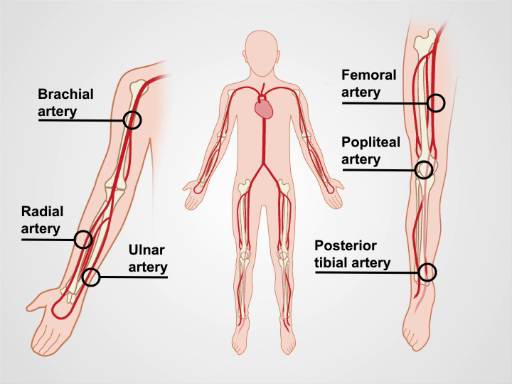
Figure 1. The major arm and leg arteries.
Процедура
1. Preparation
- Wash your hands prior to examining the patient.
- Have the patient put on a gown. This examination should never occur through clothing.
- Check the blood pressure in both arms.
2. The Upper Extremities
- Have the patient lie supine on the exam table, with the head raised to a comfortable position.
- Begin with inspection by exposing the entirety of both arms. Note symmetry, color, hair pattern, size, skin changes, nail changes
Заявка и Краткое содержание
Peripheral vascular disease is an important cause of morbidity, particularly in older patients. The detection and subsequent treatment of PVD can improve quality of life and potentially mitigate cardiovascular and cerebrovascular complications. General screening for peripheral vascular disease of the extremities is not a current recommendation by the US Preventive Service Task Force (USPSTF). However, the USPSTF does recommend ultrasound screening for abdominal aortic aneurysms in males who have smoked and are aged 65 to
Перейти к...
Видео из этой коллекции:

Now Playing
Peripheral Vascular Exam
Physical Examinations I
68.8K Просмотры

General Approach to the Physical Exam
Physical Examinations I
117.6K Просмотры

Observation and Inspection
Physical Examinations I
95.0K Просмотры

Palpation
Physical Examinations I
84.5K Просмотры

Percussion
Physical Examinations I
101.7K Просмотры

Auscultation
Physical Examinations I
62.2K Просмотры

Proper Adjustment of Patient Attire during the Physical Exam
Physical Examinations I
83.4K Просмотры

Blood Pressure Measurement
Physical Examinations I
108.8K Просмотры

Measuring Vital Signs
Physical Examinations I
114.9K Просмотры

Respiratory Exam I: Inspection and Palpation
Physical Examinations I
157.3K Просмотры

Respiratory Exam II: Percussion and Auscultation
Physical Examinations I
212.9K Просмотры

Cardiac Exam I: Inspection and Palpation
Physical Examinations I
176.6K Просмотры

Cardiac Exam II: Auscultation
Physical Examinations I
140.1K Просмотры

Cardiac Exam III: Abnormal Heart Sounds
Physical Examinations I
91.9K Просмотры

Peripheral Vascular Exam Using a Continuous Wave Doppler
Physical Examinations I
38.6K Просмотры
Авторские права © 2025 MyJoVE Corporation. Все права защищены