
A subscription to JoVE is required to view this content. Sign in or start your free trial.
Method Article
Generation and Culturing of High-Grade Serous Ovarian Cancer Patient-Derived Organoids
In This Article
Summary
Patient-derived organoids (PDO) are a three-dimensional (3D) culture that can mimic the tumor environment in vitro. In high-grade serous ovarian cancer, PDOs represent a model to study novel biomarkers and therapeutics.
Abstract
Organoids are 3D dynamic tumor models that can be grown successfully from patient-derived ovarian tumor tissue, ascites, or pleural fluid and aid in the discovery of novel therapeutics and predictive biomarkers for ovarian cancer. These models recapitulate clonal heterogeneity, the tumor microenvironment, and cell-cell and cell-matrix interactions. Additionally, they have been shown to match the primary tumor morphologically, cytologically, immunohistochemically, and genetically. Thus, organoids facilitate research on tumor cells and the tumor microenvironment and are superior to cell lines. The present protocol describes distinct methods to generate patient-derived ovarian cancer organoids from patient tumors, ascites, and pleural fluid samples with a higher than 97% success rate. The patient samples are separated into cellular suspensions by both mechanical and enzymatic digestion. The cells are then plated utilizing a basement membrane extract (BME) and are supported with optimized growth media containing supplements specific to the culturing of high-grade serous ovarian cancer (HGSOC). After forming initial organoids, the PDOs can sustain long-term culture, including passaging for expansion for subsequent experiments.
Introduction
In 2021, approximately 21,410 women in the United States were newly diagnosed with epithelial ovarian cancer, and 12,940 women died of this disease1. Although sufficient advancements have been made in surgery and chemotherapy, over 70% of patients with advanced disease develop chemotherapeutic resistance and die within 5 years of diagnosis2,3. Thus, new strategies to treat this deadly disease and representative, reliable models for preclinical research are urgently needed.
Cancer cell lines and patient-derived xenografts (PDX) created from primary ovarian tumors are the main instruments used in ovarian cancer research. A major advantage of cancer cell lines is their rapid expansion. However, their continual culture results in phenotypic and genotypic alterations that cause the cancer cell lines to deviate from the original primary cancer tumor sample. Due to the existing differences between the cancer cell line and the primary tumor, drug assays that have positive effects in cell lines fail to have these same effects in clinical trials2. To overcome these limitations, PDX models are used. These models are created by implanting fresh ovarian cancer tissue into immunodeficient mice. As they are in vivo models, they more accurately resemble human biological characteristics and, in turn, are more predictive of drug outcomes. However, these models also have significant limitations, including the cost, time, and resources needed to generate them4.
PDOs offer an alternative model for preclinical research that overcomes the limitations of both cancer cell lines and PDX models. PDOs recapitulate a patient's tumor and tumor microenvironment and, thus, provide an in vitro tractable model ideal for preclinical research2,3,5. These 3D models have self-organization capabilities that model the primary tumor, which is a feature that their two-dimensional (2D) cell line counterparts do not possess. Further, these models have been shown to genetically and functionally represent their parent tumors and, thus, are reliable models for studying novel therapeutics and biological processes. In short, they offer long-term expansion and storage capabilities similar to cell lines but also encompass the microenvironment and cell-cell interactions inherent to mouse models4,6.
The present protocol describes the creation of PDOs from patient-derived tumors, ascites, and pleural fluid samples with a higher than 97% success rate. The PDO cultures can then be expanded for multiple generations and used to test drug therapy sensitivity and predictive biomarkers. This method represents a technique that could be used to personalize treatments based on the therapeutic responses of PDOs.
Protocol
All human tissue specimens collected for research were obtained according to the Institutional Review Board (IRB)-approved protocol. The protocols outlined below were performed in a sterile human tissue culture environment. Informed written consent was obtained from human subjects. Eligible patients had to have a diagnosis or presumed diagnosis of ovarian cancer, be willing and able to sign informed consent, and be at least 18 years of age. Tumor tissue (malignant primary tumor or metastatic sites), ascites, and pleural fluid were obtained from consenting patients at the time of their procedure. These specimens were immediately transported to the laboratory and processed for organoid generation using the methods outlined below.
1. Media preparation
- Complete organoid media preparation
- Prepare R-spondin 1/Noggin conditioned medium following a previously published report7.
NOTE: R-spondin-1/Noggin conditioned medium is a more affordable alternative to commercially available recombinant proteins. HEK293T cells stably secreting R-spondin-1 and Noggin via lentivirus-mediated transduction were a generous gift from Ron Bose, Washington University School of Medicine in St. Louis, and Anil Rustgi, New York-Presbyterian/Columbia University Irving Medical Center8,9,10. Commercial conditioned medium could be used as a substitute (see Table of Materials).
- Prepare R-spondin 1/Noggin conditioned medium following a previously published report7.
- To make the complete organoid medium, combine 10% R-spondin 1/Noggin conditioned medium, 50 ng/mL EGF, 10 ng/mL FGF-10, 10 ng/mL FGF2, 1x B27, 10 mmol/L nicotinamide, 1.25 mmol/L N-acetylcysteine, 1 µmol/L prostaglandin E2, 10 µmol/L SB202190, 500 nmol/L A83-01, and 10 µM ROCK inhibitor (see Table of Materials).
NOTE: The medium may be stored at 4 °C for up to 3 months. This medium was adapted from Hill et al.11. The concentrations and ingredients of the medium are the same, with the addition of a ROCK inhibitor. - Prepare organoid base medium by combining 500 mL of an advanced formulation of DMEM/F12 with 1% penicillin-streptomycin, 1x dipeptide, L-alanyl-L-glutamine, and 1x HEPES (10 mM) (see Table of Materials).
2. Harvesting organoids from ascites and pleural fluid
NOTE: Ascites and pleural fluid must be processed as soon as possible for the best yield of organoids. Thaw previously aliquoted BME, DNase I, and DNase I reaction buffer (see Table of Materials) by placing it on ice until the contents are liquefied.
- Obtain ascites and pleural fluid from consenting patients at the time of standard care surgeries or procedures, and transport at room temperature in a travel container to the laboratory.
NOTE: All ascites or pleural fluid processing should be performed in a sterile environment. - Transfer 50 mL of ascites or pleural fluid to 50 mL conical tubes (the number of tubes depends on the volume of ascites obtained). Centrifuge at 1,650 x g for 5 min at 4 °C. After centrifugation, use a glass Pasteur pipette to carefully aspirate the supernatant.
- Continue by adding 50 mL of ascites or pleural fluid to the previously centrifuged pellet, and centrifuge again at 1,650 x g for 5 min at 4 °C. Carefully aspirate the supernatant using a glass Pasteur pipette. Repeat this step until all the ascites or pleural fluid have been processed.
- Prepare a 100 µg/mL DNase I solution by combining 1,000 µL of nuclease-free water, 100 µL of DNase I reaction buffer, and 10 µL of DNase I.
NOTE: The DNase I treatment applied is sufficient to make a single-cell suspension regardless of the presence of cell aggregates in some patient samples12. - Resuspend each cell pellet in 1 mL of 100 µg/mL DNase I solution. Gently add the DNase I solution dropwise, and allow the tube to incubate for 15 min at room temperature.
NOTE: Add a minimum of 1 mL of DNase I solution. If 1 mL is not enough to disturb the pellet, add an additional 1 mL. - After incubation, add 25 mL of organoid base medium (step 1.3) to the cells, and gently invert to mix. Then, centrifuge at 1,650 x g for 5 min at 4 °C. After centrifugation, carefully aspirate the supernatant using a glass Pasteur pipette.
- Resuspend the newly formed cell pellets in pre-warmed 5 mL of 1x red blood cell (RBC) lysis buffer (see Table of Materials). Set the vortex to 458 x g, and vortex the solutions in each conical tube. Once the solutions are homogenous, use a serological pipet to combine the contents of all the conical tubes into a single 50 mL conical tube.
- Incubate the conical tube containing the vortexed solution at room temperature for 5 min. Once incubation is complete, centrifuge at 1,650 x g for 5 min at 4 °C.
NOTE: Examine the pellet. A pink/red pellet indicates the presence of RBCs, which would require the RBC lysis buffer step to be repeated until the pellet is no longer red. - After centrifugation, carefully aspirate the supernatant using a glass Pasteur pipette. Then, wash the pellet with 10 mL of PBS, vortex the solution at 458 x g, and centrifuge at 1,650 x g for 5 min at 4 °C.
- If a large cell pellet is formed, aspirate the PBS using a glass Pasteur pipette, and add 1 mL of organoid base medium (step 1.3) on top of the pellet. Vortex the solution at 458 x g, and transfer 300-400 µL to a microcentrifuge tube. Centrifuge the microcentrifuge tube at 1,650 x g for 5 min at 4 °C.
NOTE: The portion of the cell pellet not placed in the microcentrifuge tube can be frozen down for future use (500 µL of cells to 1 mL of 10% DMSO in FBS). The frozen cell pellet can be stored for weeks at −80 °C and for years if placed in liquid nitrogen13. - Carefully aspirate the organoid base medium (step 1.3) using a glass Pasteur pipette, and resuspend in BME (see Table of Materials) using cold tips.
NOTE: The amount of BME is based on the size of the pellet. It is recommended to use 25% organoid base medium (step 1.3) with resuspended cells to 75% BME. - Plate 40 µL aliquots of the resuspended cell solution onto a 6-well plate. Plate up to five aliquots per well (Figure 1).
- Immediately place the plate in a 37 °C incubator for 20 min to allow the BME to solidify. After incubation, gently add 2 mL of complete organoid medium (step 1.2) into each well.

Figure 1: Plating of patient-derived ovarian cancer organoids. Representative image of the organoid plating. Aliquots of the organoid mixture are carefully plated, ensuring no bubbles are formed. Please click here to view a larger version of this figure.
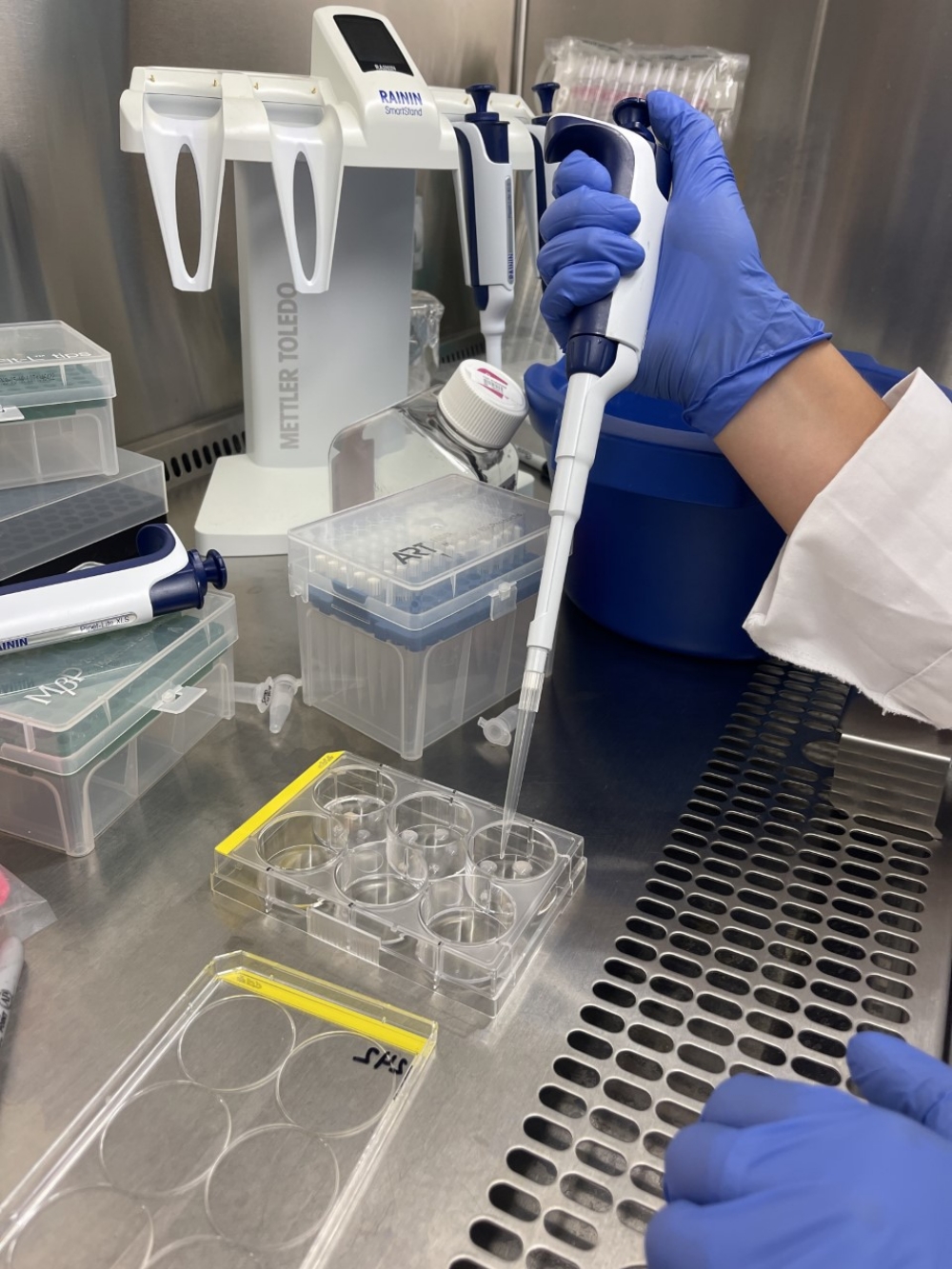{kind=link}
3. Harvesting organoids from tissue
NOTE: Tissue must be processed as soon as possible for the best yield of organoids.
- Collect and transport the tumor on ice in a travel container containing PBS.
- Place the sample on a 10 cm tissue culture dish (Figure 2). Using a disposable scalpel, mince the tissue. Next, using the dull end of a disposable syringe, crush the tissue until a homogenous mixture has been created.
- Using forceps, place the homogenous tissue mixture into a dissociation tube. For every 1-2 mL of homogenized tissue, add 7-8 mL of 1 mg/mL type II collagenase solution (see Table of Materials) in organoid base medium (step 1.3) and 1 mL of DNase I solution. Vortex the solution at 458 x g.
NOTE: The amount of tissue will determine the amount of collagenase solution and the number of tubes needed. - Use the dissociation machine (see Table of Materials) to liquefy the tissue while it is in the collagenase solution. Run the program 37C_h_TDK3 (1 h) until it is a single-cell suspension.
NOTE: The program will need to be rerun if the resulting mixture is not homogenous (i.e., if tissue pieces are still present in the mixture). If the tissue is digested but the solution is viscous, dilute using organoid base medium (step 1.3). - Transfer the homogenized mixture to a new 50 mL conical tube, and add 20-40 mL of organoid base medium (step 1.3). Then, filter the solution through a 100 µm cell strainer into a newly labeled 50 mL conical tube.
- Centrifuge the filtered mixture at 1,650 x g for 5 min at 4 °C. Then, carefully aspirate the supernatant using a glass Pasteur pipette.
- Prepare a 100 µg/mL DNase I solution by combining 1,000 µL of nuclease-free water, 100 µL of DNase I reaction buffer, and 10 µL of DNase I.
NOTE: The DNase I treatment applied is sufficient to make a single-cell suspension regardless of the presence of cell aggregates in some patient samples12. - Resuspend the cells in 1 mL of 100 ug/mL DNase I solution. Gently add the DNase I solution dropwise, and allow the tube to incubate for 15 min at room temperature.
- After incubation, add 25 mL of organoid base medium (step 1.3) to the cells, and gently invert to mix. Then, centrifuge at 1,650 x g for 5 min at 4 °C. After centrifugation, carefully aspirate the supernatant using a glass Pasteur pipette.
- Resuspend the newly formed cell pellet in 5 mL of pre-warmed 1x RBC lysis buffer. Vortex the solutions in each conical tube at 458 x g.
- Incubate the conical tube containing the cell pellet resuspended in the RBC lysis buffer for 5 min. Once the incubation is complete, centrifuge at 1,650 x g for 5 min at 4 °C.
NOTE: Examine the pellet. A pink/red pellet indicates the presence of RBCs, which would require the RBC lysis buffer step to be repeated until the pellet appears white. - After centrifugation, carefully aspirate the supernatant using a glass Pasteur pipette. Then, wash the pellet with 10 mL of PBS, vortex the solution at 458 x g, and centrifuge at 1,650 x g for 5 min at 4 °C.
- If a large cell pellet is formed, aspirate the PBS using a glass Pasteur pipette, and add 1 mL of organoid base medium (step 1.3) on top of the pellet. Vortex the solution at 458 x g, and transfer 300-400 µL to a microcentrifuge tube. Centrifuge at 1,650 x g for 5 min at 4 °C.
NOTE: The portion of the cell pellet not placed in the microcentrifuge tube can be frozen down for future use (500 µL of cells to 1 mL of 10% DMSO in FBS) (step 5.1). The frozen cell pellet can be stored for weeks at −80 °C and for years if placed in liquid nitrogen13. - Carefully aspirate the organoid base medium using a glass Pasteur pipette, and resuspend in BME using cold tips.
NOTE: The amount of BME is based on the size of the pellet. Adding 25% organoid base medium (step 1.3) with resuspended cells to 75% BME is recommended. - Plate the resuspended cell solution onto a 6-well plate in 40 µL aliquots. Plate up to five aliquots per well.
- Immediately place the well plate in the incubator for 20 min. After incubation, gently add 2 mL of complete organoid medium (step 1.2) into each well.

Figure 2: Tumor tissue prior to dissection. Representative image of tumor tissue obtained for organoid generation. Please click here to view a larger version of this figure.
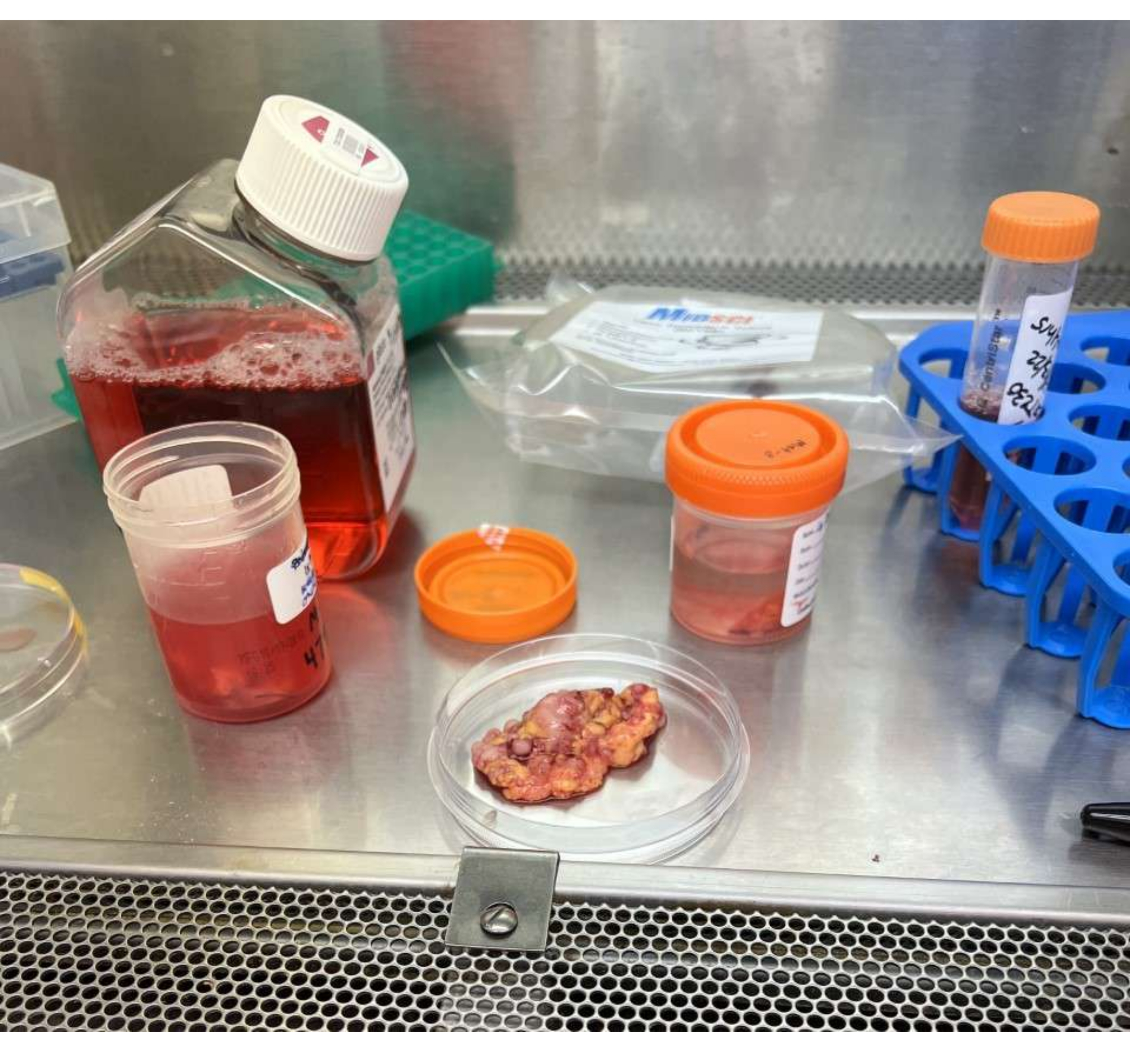{kind=link}
4. Passaging of organoids
NOTE: If the sample is confluent, each organoid well can be passaged weekly to two new wells.
- Utilizing a 1 mL pipette, add 1 mL of organoid base medium (step 1.3) to each well, and pipette the media up and down directly onto the organoid tabs to dissociate it. Collect all the medium containing the resuspended pellets in a 15 mL conical tube.
- Centrifuge the 15 mL conical tube containing the mixture at 1,650 x g for 5 min at 4 °C. Then, carefully aspirate the supernatant using a glass Pasteur pipette.
- Add 1 mL of animal origin-free, recombinant enzyme (see Table of Materials) to the cell pellet, vortex the solution at 458 x g, and transfer to a 1.5 mL microcentrifuge tube. Allow the tube to incubate for 15 min in a 37 °C water bath.
- After incubation, centrifuge at 1,650 x g for 5 min at 4 °C. Then, carefully aspirate the supernatant using a glass Pasteur pipette.
- Resuspend the pellet in BME.
NOTE: The amount of BME is based on the size of the pellet. Adding 25% organoid base media (step 1.3) with resuspended cells to 75% BME is recommended. - Plate the resuspended cell solution into a 6-well plate in 40 µL aliquots. Plate up to five aliquots per well. Once all the aliquots have been plated, immediately place the well plate in the incubator for 20 min. After incubation, gently add 2 mL of complete organoid medium (step 1.2) into each well.
5. Freezing and thawing of organoids
- Freezing of organoids
- Begin with steps 4.1-4.4.
- Resuspend the cell pellet in 0.5-1 mL of recovery cell culture freezing medium (see Table of Materials), and transfer 1 mL to each cryovial.
- Then, place the cryovials in an isopropanol-filled container at −80 °C for up to 2 weeks before transferring them to a liquid nitrogen tank for long-term storage13.
- Thawing of organoids
- Remove the samples from the liquid nitrogen tank, and thaw at 37 °C water bath.
- Once thawed, transfer to a 15 mL conical tube, and centrifuge at 1,650 x g for 5 min at 4 °C. After centrifugation, carefully aspirate the supernatant using a glass Pasteur pipette.
- Resuspend the pellet in BME.
NOTE: The amount of BME is based on the size of the pellet. Adding 25% organoid base media (step 1.3) with resuspended cells to 75% BME is recommended. - Plate the resuspended cell solution onto a 6-well plate in 40 µL aliquots. Place up to five aliquots per well.
- Immediately place the plate in the incubator for 20 min. After incubation, gently add 2 mL of complete organoid medium (step 1.2) to the wells.
6. Embedding and generating formalin-fixed paraffin-embedded (FFPE) slides to evaluate the organoid composition
- After culturing organoids for at least 10 days to ensure adequate size, remove the complete organoid medium from the wells, and add 1 mL of 2% paraformaldehyde fixative (PFA). Incubate at room temperature for 5-10 min.
- After incubation, wash the cultured organoid aliquots 3x for 5 min each time with 1 mL of PBS.
- Remove the PBS from each well, and add 1 mL of warm 2% agar in deionized H2O to each well. When adding the agar, lift the cultured organoid aliquots from the plate using a spatula.
NOTE: It is important not to let the agar harden before lifting the cultured organoid aliquots.- Allow the agar to solidify in the well at room temperature.
- Using a small spatula, free the solidified agar from the well, and store it in a cassette for up to 48 h (see Table of Materials) at 4 °C in 70% ethanol until processing14.
- Embed the samples in paraffin15, cut the slides to a thickness of 5 µm, and stain the slides with hematoxylin and eosin (H&E, see Table of Materials) staining using a standard protocol15.
Results
To generate PDOs, the samples were digested mechanically and enzymatically into single-cell suspensions. The cells were then resuspended in BME and supplemented with specifically engineered media (Figure 3). Organoids are typically established over a time frame of 10 days, after which they demonstrate discrete organoids in culture (Figure 4).
Discussion
Ovarian cancer is extremely deadly due to its advanced stage at diagnosis, as well as the common development of chemotherapy resistance. Many advances in ovarian cancer research have been made by utilizing cancer cell lines and PDX models; however, there is an evident need for a more representative and affordable in vitro model. PDOs have proven to accurately represent the tumor heterogeneity, the tumor microenvironment, and the genomic and transcriptomic features of their primary tumors and, thus, are ideal pre...
Disclosures
The authors have nothing to disclose.
Acknowledgements
We are grateful for the guidance of Ron Bose, MD, PhD, and the assistance of Barbara Blachut, MD, in establishing this protocol. We would also like to acknowledge Washington University's School of Medicine in St. Louis's Department of Obstetrics and Gynecology and Division of Gynecologic Oncology, Washington University's Dean's Scholar Program, and the Reproductive Scientist Development Program for their support of this project.
Materials
| Name | Company | Catalog Number | Comments |
| 1% HEPES | Life Technologies | 15630080 | |
| 1% Penicillin-Streptomycin | Fisher Scientific | 30002CI | |
| 1.5 mL Eppendorf Tubes | Genesee Scientific | 14125 | |
| 10 cm Tissue Culture Dish | TPP | 93100 | |
| 10 mL Serological Pipet | |||
| 100 µm Cell Filter | MidSci | 100ICS | |
| 15 mL centrifuge tubes | Corning | 430052 | |
| 2 mL Cryovial | Simport Scientific | T301-2 | |
| 2% Paraformaldehyde Fixative | Sigma-Aldrich | ||
| 37 °C water bath | NEST | 602052 | |
| 3dGRO R-Spondin-1 Conditioned Media Supplement | Millipore Sigma | SCM104 | |
| 6 well plates | TPP | 92006 | |
| 70% Ethanol | Sigma-Aldrich | R31541GA | |
| A83-01 | Sigma-Aldrich | SML0788 | |
| Advanced DMEM/F12 | ThermoFisher | 12634028 | |
| Agar | Lamda Biotech | C121 | |
| B-27 | Life Technologies | 17504044 | |
| Centrifuge | |||
| Cultrex Type 2 | R&D Systems | 3533-010-02 | basement membrane extract |
| DNase I | New England Bio Labs | M0303S | |
| DNase I Reaction Buffer | New England Bio Labs | M0303S | |
| EGF | PeproTech | AF-100-15 | |
| FBS | Sigma-Aldrich | F2442 | |
| FGF-10 | PeproTech | 100-26 | |
| FGF2 | PeproTech | 100-18B | |
| gentleMACS C Tubes | Miltenyi BioTech | 130-096-334 | |
| gentleMACS Octo Dissociator with Heaters | Miltenyi BioTech | 130-096-427 | We use the manufacturers protocol. |
| GlutaMAX | Life Technologies | 35050061 | dipeptide, L-alanyl-L-glutamine |
| Hematoxylin and Eosin Staining Kit | Fisher Scientific | NC1470670 | |
| Histoplast Paraffin Wax | Fisher Scientific | 22900700 | |
| Microcentrifuge | |||
| Mr. Frosty Freezing Container | Fisher Scientific | 07202363S | |
| N-acetylcysteine | Sigma-Aldrich | A9165 | |
| Nicotinamide | Sigma-Aldrich | N0636 | |
| p1000 Pipette with Tips | |||
| p200 Pipette with Tips | |||
| Pasteur Pipettes 9" | Fisher Scientific | 1367820D | |
| PBS | Fisher Scientific | MT21031CM | |
| Pipet Controller | |||
| Prostaglandin E2 | R&D Systems | 2296 | |
| Puromycin | ThermoFisher | A1113802 | |
| Recombinant Murine Noggin | PeproTech | 250-38 | |
| Recovery Cell Culture Freezing Medium | Invitrogen | 12648010 | |
| Red Blood Cell Lysis Buffer | BioLegend | 420301 | |
| ROCK Inhibitor (Y-27632) | R&D Systems | 1254/1 | |
| SB202190 | Sigma-Aldrich | S7076 | |
| T75 Flask | MidSci | TP90076 | |
| Tissue Culture Hood | |||
| Tissue Embedding Cassette | |||
| TrypLE Express | Invitrogen | 12604013 | animal origin-free, recombinant enzyme |
| Type II Collagenase | Life Technologies | 17101015 | |
| Vortex |
References
- Bray, F., et al. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians. 68 (6), 394-424 (2018).
- Drost, J., Clevers, H. Organoids in cancer research. Nature Reviews Cancer. 18 (7), 407-418 (2018).
- Pauli, C., et al. Personalized in vitro and in vivo cancer models to guide precision medicine. Cancer Discovery. 7 (5), 462-477 (2017).
- Fujii, E., Kato, A., Suzuki, M. Patient-derived xenograft (PDX) models: Characteristics and points to consider for the process of establishment. Journal of Toxicologic Pathology. 33 (3), 153-160 (2020).
- Yang, J., et al. Application of ovarian cancer organoids in precision medicine: Key challenges and current opportunities. Frontiers in Cell and Developmental Biology. 9, 701429 (2021).
- Yang, H., et al. Patient-derived organoids: A promising model for personalized cancer treatment. Gastroenterology Report. 6 (4), 243-245 (2018).
- Karakasheva, T. A., et al. Generation and characterization of patient-derived head and neck, oral, and esophageal cancer organoids. Current Protocols in Stem Cell Biology. 53 (1), 109 (2020).
- Madison, B. B., et al. Let-7 represses carcinogenesis and a stem cell phenotype in the intestine via regulation of Hmga2. PLoS Genetics. 11 (8), 1005408 (2015).
- Sato, T., et al. Single Lgr5 stem cells build crypt-villus structures in vitro without a mesenchymal niche. Nature. 459 (7244), 262-265 (2009).
- Murray, E., et al. HER2 and APC mutations promote altered crypt-villus morphology and marked hyperplasia in the intestinal epithelium. Cellular and Molecular Gastroenterology and Hepatology. 12 (3), 1105-1120 (2021).
- Hill, S. J., et al. Prediction of DNA repair inhibitor response in short-term patient-derived ovarian cancer organoids. Cancer Discovery. 8 (11), 1404-1421 (2018).
- Passarelli, M. C., et al. Leucyl-tRNA synthetase is a tumour suppressor in breast cancer and regulates codon-dependent translation dynamics. Nature Cell Biology. 24 (3), 307-315 (2022).
- Pleguezuelos-Manzano, C., et al. Establishment and culture of human intestinal organoids derived from adult stem cells. Current Protocols in Immunology. 130 (1), 106 (2020).
- Stumm, M. M., et al. Validation of a postfixation tissue storage and transport medium to preserve histopathology and molecular pathology analyses (total and phosphoactivated proteins, and FISH). American Journal of Clinical Pathology. 137 (3), 429-436 (2012).
- Feldman, A. T., Wolfe, D. Tissue processing and hematoxylin and eosin staining. Methods in Molecular Biology. 1180, 31-43 (2014).
- Ooft, S. N., et al. Patient-derived organoids can predict response to chemotherapy in metastatic colorectal cancer patients. Science Translational Medicine. 11 (513), (2019).
- Aisenbrey, E. A., Murphy, W. L. Synthetic alternatives to Matrigel. Nature Reviews Materials. 5 (7), 539-551 (2020).
- Nanki, Y., et al. Patient-derived ovarian cancer organoids capture the genomic profiles of primary tumours applicable for drug sensitivity and resistance testing. Scientific Reports. 10, 12581 (2020).
- Mead, B. E., et al. Screening for modulators of the cellular composition of gut epithelia via organoid models of intestinal stem cell differentiation. Nature Biomedical Engineering. 6 (4), 476-494 (2022).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved