
El cerebro dividido
Visión general
Fuente: Laboratorios de Jonas T. Kaplan y Sarah I. Gimbel, University of Southern California
El estudio de cómo el daño cerebral afecta funcionamiento cognitivo ha sido históricamente una de las herramientas más importantes para la Neurociencia cognitiva. Mientras que el cerebro es una de las partes más protegidas del cuerpo, hay muchos eventos que pueden afectar el funcionamiento del cerebro. Problemas vasculares, tumores, enfermedades degenerativas, infecciones, traumas de la fuerza bruta y Neurocirugía son sólo algunas de las causas de daño cerebral, que puede producir diferentes patrones de lesiones tisulares que afectan al cerebro funcionando en diferentes maneras.
La historia de la neuropsicología está marcada por varios casos bien conocidos que llevaron a los avances en la comprensión del cerebro. Por ejemplo, en 1861 Paul Broca observó como daño a la izquierda lóbulo frontal dio lugar a la afasia, un trastorno del lenguaje adquirido. Como otro ejemplo, mucho sobre la memoria se ha aprendido de los pacientes con amnesia, como el famoso caso de Henry Molaison, conocido por muchos años en la literatura de la neuropsicología como "H.M.", cuya lóbulo temporal la cirugía llevó a un profundo déficit en la formación de ciertos tipos de nuevas memorias.
Mientras que la observación y pruebas de pacientes con daño cerebral focal ha proporcionado Neurociencia con perspicacia en el funcionamiento del cerebro, mucho cuidado debe tenerse en el diseño de pruebas para revelar la naturaleza específica de lo déficit. También, porque el cerebro es una compleja red de neuronas interconectadas, daños a la región del cerebro de uno pueden afectar funcionamiento en regiones lejos del daño. Para demostrar cómo el daño cerebral puede afectar las conexiones entre regiones del cerebro, este video analiza el caso del cerebro denominada split.
El cuerpo calloso es un haz grande de fibras que conecta los hemisferios izquierdos y derecho del cerebro. Es uno de los más grandes tractos de materia blanca en el cerebro y puede ser fácilmente reconocida en una vista sagital de la línea media del cerebro. En la década de 1960, neurocirujanos descubrieron que cortar el cuerpo calloso podría ser un tratamiento acertado para algunos tipos de epilepsia, que implica la actividad de los nervios incontrolable que se separa a través del cerebro. Personas que se sometieron a la operación de división tenían sus dos hemisferios separados quirúrgicamente, tal que los hemisferios izquierdos y derecho ya no eran capaces de comunicarse. Esta condición permitió experimentadores probar las funciones del hemisferio derecho e izquierdo independientemente, para aprender sobre las capacidades relativas y sobre la naturaleza de la comunicación entre ellos.
Este video muestra como se prueba un paciente produzca para revelar algunas de las diferencias entre los dos hemisferios del cerebro y ver algunas consecuencias dramáticas de tal desconexión. Las versiones originales de estos experimentos fueron desarrolladas por Michael Gazzaniga y colegas1, 2 y más tarde fueron elaboradas por otros; 3 la versión presentada aquí incorpora la más reciente modernización de la metodología.
Procedimiento
1. paciente y control de la captación de
- Hay una gran variedad de pacientes con síndromes de desconexión, incluyendo callosotomies quirúrgica completa y parcial y condiciones congénitas, tales como agenesia del cuerpo calloso (ACC), en la que el cuerpo calloso no se desarrolla completamente. Hay varias extensiones que conectan los dos hemisferios; el más grande es el cuerpo calloso, pero algunas fibras cruzan en la comisura anterior, comisura hipocampal y comisura posterior.
Tenga en cuenta que estas variedades de desconexión pueden conducir a diferentes resultados conductuales en estas pruebas. - Para los efectos de este experimento, preseleccionar el paciente mediante el uso de neuroimágenes para confirmar la ausencia de fibras de conexión.
- MRI estándar y proyección de imagen de difusión, que puede utilizarse para tractos de materia blanca imagen, son particularmente útiles. Sabiendo que las fibras de conexión están presentes en el paciente ayuda a la interpretación de los resultados. En esta demostración, un paciente con una callosotomía completa ha sido seleccionado.
- Asegúrese de que el paciente ha sido informado completamente de los procedimientos de investigación y ha firmado todos los formularios de consentimiento apropiado.
- Reclutar a 20 participantes de la misma edad y género que el paciente, con inteligencia, con puntuaciones en la escala de inteligencia adultos de Wechsler (WAIS).
2. recolección de datos
- Para presentar estímulos visuales en el hemisferio izquierdo o derecho solamente, los estímulos deben presentarse adecuadamente a un campo de visión. Tenga en cuenta que esto no es equivalente a la presentación de los estímulos a un ojo. Proyectos de cada ojo a ambos hemisferios del cerebro; por ejemplo, la parte del ojo izquierdo que se ve el campo visual izquierdo es procesada por el hemisferio derecho, pero la parte del ojo izquierdo que procesa el campo visual derecho es vista por el hemisferio izquierdo. Por lo tanto, para presentar una imagen para el hemisferio izquierdo, presente enteramente en el campo visual derecho, que es a la derecha de donde mira el paciente.
- Para lograr esta lateralización, utilizar una mentonera para mantener los ojos aproximadamente 22 pulgadas de la pantalla del ordenador. Colocar la barbilla del paciente cómodamente dentro de la mentonera, frente a la pantalla.
- Tiene una pequeña Cruz permanezcan en el centro de la pantalla para proporcionar una localización para el paciente fijar sus ojos.
- Instruir al paciente para mantener su fijación en esta cruz durante todo el experimento, así como las imágenes aparecen a la izquierda o derecha de él.
- Explicar al paciente que cuando aparece una imagen, debe decir el nombre del objeto en voz alta.
- Presentamos las imágenes de objetos bien conocidos brevemente a la izquierda o derecha de la pantalla para proyectar a los hemisferios izquierdos o derecho del cerebro, respectivamente. se presentan 50 imágenes en orden aleatorio de un conjunto de objetos que incluyen dibujos fácilmente reconocibles, como una manzana, una pelota, una escoba y un pollo.
- Presentar las imágenes de menos de 150 ms asegurar la correcta lateralización. Esto es tiempo suficiente para ver el estímulo, pero lo suficientemente rápido, así que el paciente no es capaz de mover los ojos para ver el estímulo de la visión central.
- Pida al paciente que nombre los objetos presentados en la pantalla en voz alta y grabar sus respuestas. Esto es una prueba de capacidad lingüística verbal y debe revelar las diferencias en el discurso la capacidad entre los hemisferios.
- Si el paciente es incapaz de nombrar a cualquiera de los objetos, pida al paciente que dibuje el objeto, sin mirar el papel, con la mano ipsilateral a (en el mismo lado) del estímulo. Esto sirve como medida del conocimiento del estímulo no lingüístico.
- La mano ipsilateral al estímulo es controlada por el hemisferio que vio el estímulo. Por ejemplo, cuando el estímulo se presenta en el campo visual izquierdo, es procesada por el hemisferio derecho. El hemisferio derecho es en gran parte responsable por el control de la mano izquierda.
- Asegúrese de que el paciente no se mira en su mano mientras se dibuja para mantener el aislamiento del estímulo a un hemisferio.
- Cuando el paciente termina de dibujar un objeto, pedirles que mira el objeto y decir lo que es en voz alta. Esto confirma que el paciente conoce el nombre del objeto cuando se presenta en visión central, incluso si no son capaces de nombre cuando se presenta a un solo hemisferio.
- Repita el procedimiento para cada participante de control.
3. Análisis de los datos
- Para analizar el rendimiento del paciente, comparar los datos del campo medio izquierda y derecha visual con los demás. Para ello, tabular el número de respuestas correctas e incorrectas en cada campo visual y prueba la probabilidad de obtener una diferencia tan grande como el observado usando una prueba de Chi-cuadrado de independencia.
- Comparar los datos del paciente con los datos de edad, género y población control comparable de inteligencia para determinar el déficit en el comportamiento del paciente. Para ello, compile el puntaje de campo visual izquierdo y derecho del campo visual de cada persona por separado y comparar las distribuciones con un análisis de varianza de medidas repetidas test (ANOVA).
Resultados
Por lo general, los pacientes callosotomía exhiben una anomia de objetos presentados en el medio-campo visual izquierdo. Anomia es la incapacidad para nombrar objetos. Objetos presentados al derecha del campo visual, sin embargo, se nombran con una alta precisión (figura 1).
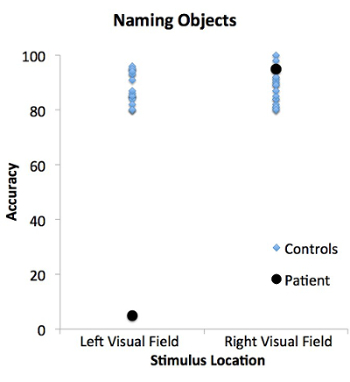
Figura 1: Paciente y control de rendimiento en la tarea de objetos nombres de estímulos presentados en los campos visuales izquierdos y derecho. El paciente (círculos negros) no es capaz de verbalmente nombre objetos presentados en el campo visual izquierdo, pero es capaz de nombrar objetos en el campo visual derecho. En contraste, la población de control (diamantes azules) nombrar objetos presentados en los campos visuales izquierdos y derecho.
Algunos pacientes pueden ser capaces de dibujar con éxito los objetos ante el campo visual izquierdo, aunque verbalmente no se nombran los ()figura 2).
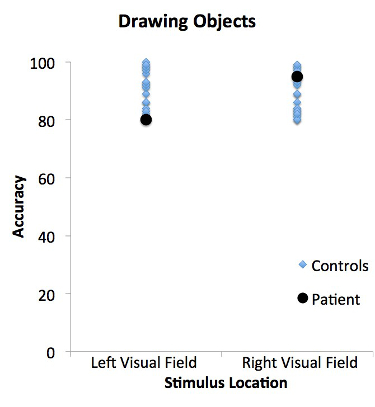
Figura 2: Paciente y control de rendimiento en la tarea de los objetos dibujo de estímulos presentados en los campos visuales izquierdos y derecho. El paciente (círculos negros) y la población control (diamantes azules) son capaces de dibujar los objetos presentados en los campos visuales izquierdos y derecho. Rendimiento del paciente no difiere de los controles emparejados.
En este caso, el paciente generalmente dice que no han visto nada. Esto es porque el hemisferio izquierdo, que es controlar el discurso, no ha visto la imagen visual. Sin embargo, el hemisferio derecho, que ha visto el objeto, puede reconocerlo pero es incapaz de generar discurso. Puesto que el hemisferio derecho es en gran medida en el control de la mano izquierda, el paciente es capaz de dibujar el objeto con la mano izquierda. Este resultado muestra una disociación entre la capacidad de reconocer un objeto y la capacidad para nombrar verbalmente un objeto.
La población control, con callosa de cuerpos intactos, pueden nombrar y dibujar los objetos presentados en el campo visual derecho o izquierdo. Esto es porque la información puede pasar libremente de un hemisferio a otro, lo que permite el intercambio de información entre las regiones del cerebro.
Aplicación y resumen
El caso de la paciente produzca revela la especialización relativa de los dos hemisferios cerebrales. Muchas de estas especializaciones se pueden demostrar también en personas sanas con comisuras intactas usando técnicas similares. Por ejemplo, las personas tienden a reconocer palabras más rápidamente cuando se presentan brevemente en el campo visual derecho comparado cuando se presentan en el campo visual izquierdo. Este experimento muestra también que incluso cuando dos regiones del cerebro sanas, daños a las conexiones entre las diferentes regiones pueden afectar el comportamiento.
Sin embargo, es importante recordar si bien el cerebro dividido la prueba demuestra las diferencias entre los dos hemisferios cerebrales en el cerebro intacto, los dos hemisferios están continuamente interactuando con los demás y trabajan en conjunto. Para aislar un estímulo a un campo visual requiere equipo especializado que puede presentar estímulos muy brevemente y de la fijación central. Puesto que la visión central es procesada por ambos hemisferios, y los ojos suelen analizar un entorno, no es una situación que suele encontrarse en la vida cotidiana.
Referencias
- Gazzaniga, M. S., Bogen, J. E., & Sperry, R. W. (1962). Some functional effects of sectioning the cerebral commissures in man. Proc Natl Acad Sci U S A, 48, 1765-1769.
- Gazzaniga, M. S., Bogen, J. E., & Sperry, R. W. (1965). Observations on visual perception after disconnexion of the cerebral hemispheres in man. Brain, 88(2), 221-236.
- Zaidel, E., Zaidel, D., & Bogen, J. E. (1990). Testing the commussurotomy patient. In A. Boulton, G. Baker, & M. Hiscock (Eds.), Neuromethods (pp. 147-201). Clifton, NJ: Humana Press.
Tags
Saltar a...
Vídeos de esta colección:

Now Playing
El cerebro dividido
Neuropsychology
68.4K Vistas

Mapas de motor
Neuropsychology
27.5K Vistas

Perspectivas de la neuropsicología
Neuropsychology
12.0K Vistas

Toma de decisiones y la Iowa Gambling Task
Neuropsychology
32.7K Vistas

Función ejecutiva en el trastorno del espectro autista
Neuropsychology
17.8K Vistas

Amnesia Anterógrada
Neuropsychology
30.3K Vistas

Correlatos fisiológicos de reconocimiento de la emoción
Neuropsychology
16.3K Vistas

Potenciales acontecimiento-relacionados y la tarea de Oddball
Neuropsychology
27.5K Vistas

Idioma: La N400 en incongruencia semántica
Neuropsychology
19.6K Vistas

Aprendizaje y la memoria: la tarea de recordar-sabe
Neuropsychology
17.2K Vistas

Medición de las diferencias de materia gris con Morfometría basada en Voxel: el cerebro Musical
Neuropsychology
17.3K Vistas

Descodificación de imágenes auditivas con análisis Multivoxel
Neuropsychology
6.4K Vistas

Atención visual: fMRI Control atencional basado en la investigación del objeto
Neuropsychology
42.0K Vistas

Utilizando imágenes de Tensor de difusión en la lesión cerebral traumática
Neuropsychology
16.8K Vistas

Uso de TMS para medir la excitabilidad motora durante la observación de la acción
Neuropsychology
10.2K Vistas
ACERCA DE JoVE
Copyright © 2025 MyJoVE Corporation. Todos los derechos reservados