
A subscription to JoVE is required to view this content. Sign in or start your free trial.
Method Article
Measuring the Functional Abilities of Children Aged 3-6 Years Old with Observational Methods and Computer Tools
In This Article
Summary
We present a protocol to use a computational tool to record and analyze the functional abilities of children aged 3-6 years old. The protocol facilitates the comparison of these abilities throughout their development and can be used to assess developmental difficulties.
Abstract
The analysis of functional abilities and their development in early childhood (0-6 years old) are fundamental aspects among young children with certain types of developmental difficulties that can facilitate prevention, through programmed interventions adapted to the needs of each user (student or patient). There are, however, few investigations to date, that have analyzed the use of automated tools for recording and interpreting the results of the initial assessment. Here, a protocol is presented to examine the functional abilities in early childhood in young children, aged between 3-6 years old, with intellectual disabilities, but the protocol can also be used for ages 0 to 6 years. The protocol makes use of a computer application, eEarlyCare, that facilitates the interpretation of the results of systematic observations, which are recorded in natural environments by professionals trained in early intervention. The software can be used to analyze 11 functional areas (Food Autonomy, Personal Care and Hygiene, Dressing and Undressing Independently, Sphincter Control, Functional Mobility, Communication and Language, Daily Life Routines, Adaptive Behavior and Attention) and a total of 114 different behaviors. Its use facilitates the analysis of the observed abilities and greatly assists early intervention. Compared to other observational methods, it allows a more efficient use of personal and material resources. The use of the computer application facilitates the recording of the observation results, which helps with organization and reflection on the observations. The software displays the observation results on-screen compared to normal developmental parameters. This information can be referred to for decision-making about the most suitable intervention program for each user (student or patient). Likewise, clustering techniques are applied to analyze the relation between the type of intellectual disabilities and functional development identified with the software, a relation that is intended to serve as a guide for early-care professional intervention.
Introduction
Observation at early ages: what and how to observe
Early childhood assessment in ordinary family contexts and at school is performed using the observational method. Hence, the evaluator must adhere to a precise observational process, the key to an accurate diagnosis and, therefore, to a successful training1. There are many development inventories that provide guidelines for assessment: The Portage Guide2, the Brunet Lézine Scale3, and the Battelle Developmental Inventory4, among others. These tools are based on internationally agreed standards set by the scientific community in the field of human evolutionary development. Although these tools analyze developmental areas (Psychomotor, Cognitive, Communication and Language, and Autonomy and Socialization), recent studies5 have proposed new tools that can also analyze these areas. These studies point out that the observational method from birth provides pointers of immense utility to early intervention and for the early detection of pathologies. However, the observational processes at these ages are complex, as they depend on behavioral observations recorded in natural contexts, which are not always easy to carry out.
Within this framework, the assessment of the acquisition of functional abilities at early ages is of great interest to parents, educators, and therapists alike. Any such assessment is of relevance for children who have been diagnosed or who are at risk of developing some disability. Early detection of developmental disorders is essential for the early diagnosis and intervention. Observational study from birth will provide indicators of this early detection and intervention5. Currently there are various tools (development inventories, scales, tests, etc.) for measuring development at those ages. The instruments that can currently be applied are developmental inventories, some of which are standardized. However, some of those instruments may require knowledge of psychometric techniques and the results are not automatically displayed on screen. For this reason, it is important to develop other tools that are easier to use and interpret.
Preparation of software for recording and interpreting data from the processes of contextual observation processes at early ages
The software development was, therefore, considered of relevance, which would assist the observers (therapist, educator, etc.) to record and to interpret the results of their observations. This protocol and software, eEarlyCare, can be used both in educational centers that work with children with disabilities and in therapeutic intervention centers aimed at this group. This is why from now on the term "user "will be used, which includes both students and patients, depending on the place where the intervention is carried out. In particular, a software that could facilitate the recording and the interpretation of data gathered in natural contexts from the observation of functional abilities among children from 0 to 6 years old. This software, eEarlyCare, is based on the functional abilities scale6 [Scale for the measurement of Functional Abilities in children between 0-6 years old] (SFA); this scale includes the measurement of 11 areas of development (Food Autonomy, Personal Care and Hygiene, Independently and dress and undresses, Sphincter control, Functional mobility, Communication and Language, Interactive symbolic play, Daily life routines, Adaptive behavior). Also, it was in turn, inspired by the Portage Guide2, the Pediatric Evaluation of Disability Inventory (PEDI)7, and the works of Bronson8, as well as Whitebread and Basilio4 on social skills at ages 0-6, the Brunet-Lézine Scale3, developmental inventories for children aged 0-67, and the Assessment Scale of the precursors9 to social skills. This tool is a computer application that is used for registering the results of each user assessment in longitudinal follow-ups (quarterly, monthly, annual, etc.). It is a referential aspect for the therapist with regard to the intervention, and for other professionals who work with children in early childhood with suspected dysfunctionalities. In addition, the software10 can automatically produce comparisons between the development of the functional abilities of different users, regardless of whether they are at the same intervention center, thereby facilitating the definition of common aspects for collaborative work.
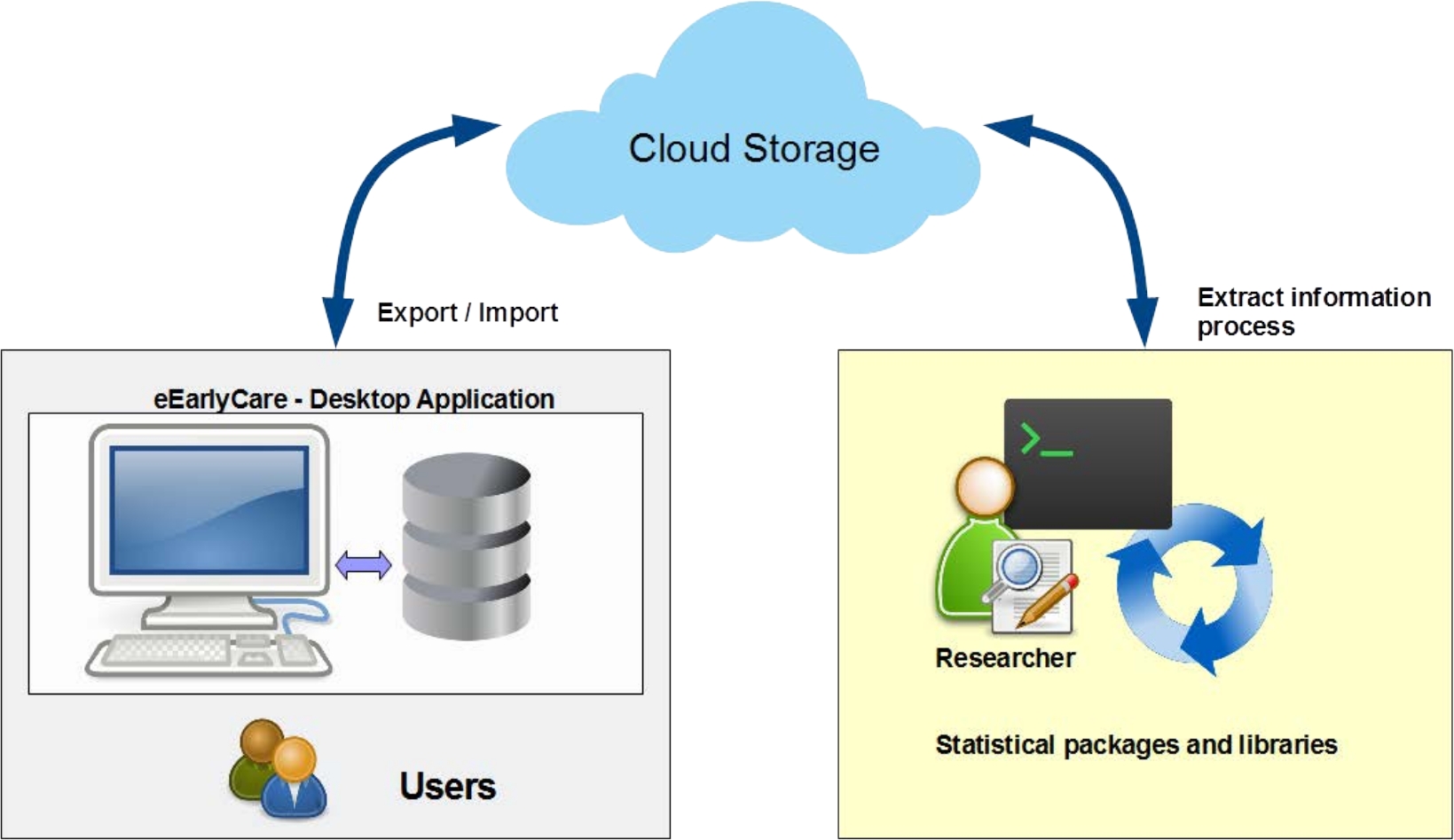
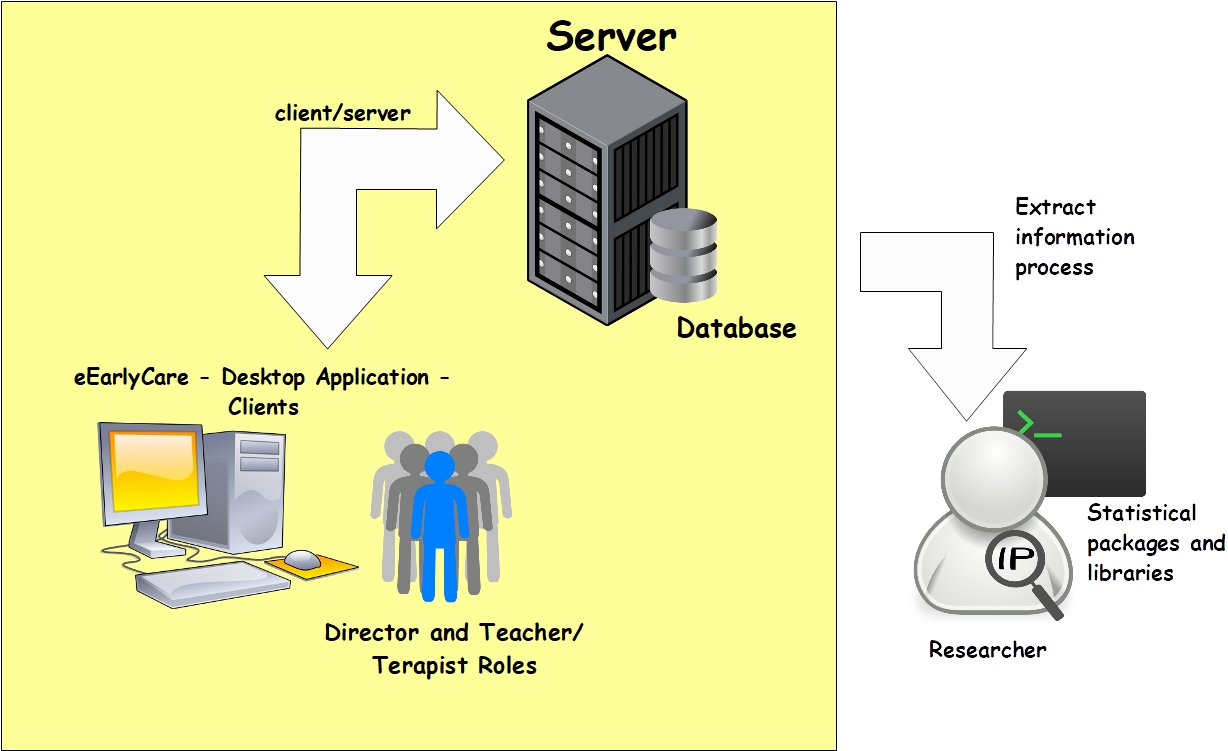
In particular, this software is based on mainstream technologies (e.g., Windows Presentation Foundation Development -WPF-11), a technological innovation that integrates advanced graphics to produce accurate graphic results12 and a positive computer user-experience. The quality of the graphs improves the visualizations and the interactivity available with other tools such as spreadsheets. The application can store the data locally on relational databases and upload the information onto the cloud to be shared. In addition, the classic client-server architecture is also supported. These features make it easy to record the data that are collected from the observations and to process the results for visualization. Also, once registered, it is very easy to export the data. This allows the data to be used in powerful statistical packages to apply data mining techniques, such as supervised (classification and/or regression) and unsupervised (grouping) machine learning.
In this study, the classification techniques are of specific utility for personalized learning13. The architecture can be seen in Figure 1 and Figure 2. In Figure 1, the functionality of cloud storage is used as a safeguard, in case of data security problems and potential loss and corruption of data when exchanged between applications. Additionally, the software can also operate in a classic network-based client-server architecture with a database (Figure 2) with all data exchanges taking place between clients (these are concepts that are used in the field of computer science). These platforms provide authentication mechanisms and restricted access, which ensure privacy and data protection, while facilitating interaction with fully developed applications. The final result is an application interface that is designed14 for early-care professionals, so that they can use Learning Analytics techniques in a simple way and refer to them, in order to follow up the degree of each student’s development in each evaluation area of the scale15.
The application also offers a general profile of each user in each of the functional areas and subareas (Table 1). It also produces a comparison between all users at any one center. In brief, it produces a personalized analysis of the intervention needs of the different users. In addition, it helps early-care professionals with their intervention programs, as it can flag up areas in which users might or might not show similar developmental patterns. All these results guide the type of intervention programs that can be used together, rather than those that have to be designed individually. The data that are linked to this interface are the SFA scores of the users that are measured on a Likert scale from 1 to 5. Those scores can be compared with the maximum developmental age scores linked to each SFA dimension. The software can also link the chronological age of each user to the developmental age of each SFA dimension; a relevant aspect for the detection of intervention areas from among which to prioritize the areas for treatment.
| Functional area | Functional sub-area |
| 1. Food Autonomy | 1. Food Texture |
| 2. Use of utensils | |
| 2. Personal Care and Hygiene | 3. Dental Hygiene |
| 4. Hairstyle | |
| 5. Nasal Care | |
| 6. Handwashing | |
| 7. Face and body wash | |
| 3. Independently dresses and undresses | 8. Dressing and undressing (waist upwards) |
| Dressing and undressing (waist downwards) | |
| 4. Sphincter control | 9. Sphincter control |
| 5. Functional mobility | 10. Upper extremity |
| 11. Transfers in WC | |
| 12. Transfers on a chair | |
| 13. Mobility and bed transfers | |
| 14. Mobility in the bathtub | |
| 15. Mobility indoors | |
| 16. Transport of objects | |
| 17. Outdoor Mobility | |
| 6. Communication and Language | 18. Word comprehension |
| 19. Understanding phrases | |
| 20. Functional use of communication | |
| 7. Resolution of tasks in social contexts | 21. Solving Problems |
| 22. Information about yourself | |
| 8. Interactive and symbolic play | 23. Interactive Play |
| 24. Interaction with the peer group | |
| 25. Play with objects | |
| 9. Daily life routines | 26. Guidance in time |
| 27. Homework | |
| 10. Adaptive behavior | 28. Self-harm behavior |
| 29. heteroagressiveness (harming others) | |
| 30. Destruction of objects | |
| 31. Disruptive behaviour (cry, shout, laugh without reason) | |
| 32. Stereotypes | |
| 11. Attention | 33. Attention |
Table 1: List of functional areas and subareas.

Figure 1: Architecture of the proposal of automation of the correction of the Scale functionality of cloud storage. Please click here to view a larger version of this figure.
{kind=link}

Figure 2: Architecture of the proposal of automation of the correction of the Scale functionality classic network. Please click here to view a larger version of this figure.
{kind=link}
Therapists and intervention professionals can use this assessment protocol and the software implementation for the assessment of functional abilities and their development in early childhood between 0 and 6 years of development. The software can be used with children within that age range, although it is especially useful for children with suspected impaired development of functional abilities. It is likewise especially useful at Special Education Centers. The Research question is whether, having observed the functional abilities of children, the use of a computer tool will facilitate the recording and the interpretation of the results for the therapist.
Access restricted. Please log in or start a trial to view this content.
Protocol
This protocol was performed in compliance with the procedural regulations of the Bioethical Committee of the University of Burgos (Spain). Prior to their participation, both the students and their parents and in some cases legal tutors had all provided their informed consent and had been fully made aware of the objectives of study. No financial compensation was offered for their participation.
1. Participant recruitment
- Recruit children between 0-6 years of age with a history of special educational needs related to alteration in the areas of motor development, cognitive, personal autonomy, and socialization and with moderate to severe intellectual disabilities. A total of 11 participants (7 boys and 4 girls) were recruited for the present study.
- Include children who have been diagnosed with an intellectual disability (moderate or severe) in accordance with the Diagnostic and Statistical Manual of Mental Disorders (DSM-5)16 and attend a Special Education Center for their schooling (Table 2).
NOTE: In each case (depending on the detection of the problem and the place where the intervention is performed), the diagnosis should have been confirmed by a pediatric neurologist at a hospital or a psychologist within a multidisciplinary team, in accordance with DSM-5. Ideally, there should be no fewer than 15 participants, since the insertion of the observation results is laborious.
| Sex | n | Mage | SDage | Rank age (months) | Disability• | Schooling | ||
| degree | ||||||||
| a | b | c | d | |||||
| Boys | 7 | 95.2 | 11.77 | 86-114 | 4 | 3 | 2 | 5 |
| Girls | 4 | 83.5 | 23.56 | 45-112 | 1 | 3 | 2 | 2 |
| NOTE:* Degree of disability: a = moderate intellectual disability; b = severe intellectual disability; Type of Schooling: c = Combined Schooling; d = Schooling in a Specific Special Education Center; M = Mean age in months; SD = Standard Deviation. * The children were diagnosed using the criteria of DSM516 | ||||||||
Table 2: Characteristics of the sample.
- Exclude children with normal development in functional areas (motor, cognitive, personal autonomy and socialization development) and children with an Intellectual functioning limitation.
2. Data collection
- Collect data on the development of the children in different functional areas (Food Autonomy, Personal Care and Hygiene, Dressing and Undressing Independently, Sphincter Control, Functional Mobility, Communication and Language, Daily Life Routines, Adaptive Behavior and Attention).
- Perform the observation using the Scale for the measurement of functional abilities (SFA)5 in children between 0-6 years old (SFA) (Table of Materials) and conduct the observation in a natural context (e.g., school settings).
- Record observations throughout the week in different natural environments that reflect the daily life of the students at the center (Table 1) (e.g., while playing, etc.).
- Let the teacher or the therapist directly attending the children at the educational institutions record the observations. Gather the observations for each functional area.
NOTE: Prior to data observation, three training sessions should be conducted for teachers or therapists. These sessions must be conducted by a psychologist or a professional with experience in early-childhood assessment.
- Let the teacher or the therapist directly attending the children at the educational institutions record the observations. Gather the observations for each functional area.
- Input the results into the software for the assessment of functional abilities in early childhood between 0-6 years old. The details on how to use the software is provided in step 3.
3. Experimental procedure
- Assigning a student to a teacher in the software
NOTE: This step has to be carried out by the director or coordinator of the center where the intervention takes place.- Log in to the software package with a username (professional) and password and select the language: English or Spanish.
- Enter the student data information from the records held by the director of the center.
- Fill in the following fields for each student: Name, Surname, Code, Sex, Date of Birth, Developmental Age, Primary Diagnosis, Secondary Diagnosis, where appropriate, and observations that are relevant to medication data, allergies, and other information of interest to the management of the center.
- Enter the teacher or therapist information from the records held at the center.
- Assign the students to a group with a teacher (or therapist) by clicking on Classroom. Go to the column Students, choose the student to be assigned to the classroom, and click on Teachers and select one.
- Allocate each group of students and their teacher (or therapist) to a classroom by clicking on Teachers, input dates, name, surname, identification code, mail, passwords and observations. Click Accept.
NOTE: The director or coordinator of the center assigns a role for each teacher or therapist to carry out the evaluations of each student or patient (as explained above, it depends on the type of center). The director or coordinator of the center can also consult the evaluations that the teacher or therapist has made.
- Use of the software by the teacher
NOTE: The teacher or therapist performing the assessment can then select an academic year and/or a term. The scale offers the possibility of selecting different functional areas for each term (Table of Materials).- Log in to the software with the username (professional) and the password previously assigned by the director of the center.
- Enter the results of the assessments completed in natural environments for each participant assigned to the classroom.
- Choose a student in the software by clicking on his/her name, and start the assessment of the different functional areas (detailed in step 2.3.1).
NOTE: The teachers or therapists can stop the assessment of each student at any time and continue at another time, having saved the data that they have registered. - Perform the comparative analysis between the development of each user and the expected development at that chronological age.
- Once the data is registered, select the column Evaluation by right clicking. Then select the year and the trimester.
- Select the column Students and select the students of a class of whom to make the evaluation. Select the column Areas clicking on the area or subarea that needs to be evaluated.
- Click on the Maximum tab. It gets the information about the students and the comparison with the development expected for their age.
NOTE: This offers a user (student or patient) or development profile for a given functional area with a comparative link to the highest expected scores for the chronological age of the user (student or patient).
- Compare the different functional areas of each user from the classroom. An analysis of the functional areas of each user can be performed with the software. Following step: once the data is registered, select the column Evaluation by right clicking. Then select the year and the trimester. Select the column Students and select the students of all classes. Select the column Areas and click on the area or subarea to evaluate.
- Click on the Maximum tab. It gets the development of the students and the comparison with the development expected for their age.
- Exporting data from the software
- Select the user data and functional areas, and export the database. Select the column Excel to get the database. Export the database in the statistics program or library of choice.
- Import the data into statistical packages and libraries such as SPSS, Weka, Python's scikit-learn, etc. and perform clustering analysis. Here, analysis with SPSS is detailed as below.
NOTE: Clustering or cluster analysis is an ‘unsupervised’ machine-learning technique, and, within k-means, it is a grouping method, which aims to partition a set of n observations into k groups, in which each observation belongs to the group with the closest mean value. In this experiment, k-means clustering was used to check the clusters of children and their functional development measured with SFA.- Select the option Analyze and Classify followed by the option k-means cluster in the statistical package.
- Select crosstabs under Descriptive Statistics, and the following two variables: the cluster variable of ‘belonging to a group’ and the degree variable (‘moderate’ or ‘severe’).
NOTE: This correspondence is important, because it offers the teacher or therapist information on the homogeneous functional development of users that goes beyond the diagnosis, providing information to propose similar intervention programs in some areas of functional development. This option is expected to facilitate full use of the educational or therapeutic service and its personal and material resources. - Select the Descriptive Statistics option and select crosstabs and the Cohen Kappa Coefficient option.
NOTE: The Cohen Kappa coefficient is a statistic which measures inter-rater agreement for qualitative (categorical) items. It is generally thought to be a more robust measure than simple percent agreement calculations, as k accounts for the possibility of the agreement occurring by chance. This coefficient provides an indicator of the reliability of the relationship found between the diagnostic classification in moderate-to-severe intellectual disabilities and the clustering of the developmental results obtained with the software.
- Use the spreadsheet to generate the spider chart and specific bar graphs for the groups of children with moderate and severe intellectual disabilities.
Access restricted. Please log in or start a trial to view this content.
Results
The present study recruited 11 participants with confirmed diagnoses [both moderate (development quotient = DQ 40-65) and severe (DQ 39-60) intellectual disabilities]. The protocol was tested in a pilot project over 20 months at a Special Education Center. All the diagnoses for this study had been confirmed by a multidisciplinary team in accordance with DSM-5, using the Brunet Lézine Scale, as the degree of affectation was beyond the scope of other scales such as the Wechsler Preschool and Primary Scale of Intellige...
Access restricted. Please log in or start a trial to view this content.
Discussion
When using the software, it is recommended that the teacher or therapist record the development of each child's functional abilities over at least for two sessions. The scale contains 114 items, 11 functional areas, which are divided into 33 functional subareas and the assessment should be the result of observation in natural contexts. In addition, the software allows early-care professionals to record evaluation data with ease and to analyze the data displayed in individual and group graphs, highlighting the develop...
Access restricted. Please log in or start a trial to view this content.
Disclosures
The authors declare that they have no competing financial interests.
Acknowledgements
We wish to thank the Vice-rectorate for Research and Knowledge Transfer of the University of Burgos for making the development of the software possible through the “VI Edición Convocatoria Prueba Concepto: Impulso a la valorización y comercialización de resultados de investigación” [VI Edition of the Call for Proof of Concept: Impulse to the valorization and marketing of research results]. We likewise thank the Educational Programs Area of the Provincial Directorate of Education and to the Special Education Center "Fray Pedro Ponce de León", both in Burgos (Spain), and to the families of the children who agreed to participate in this pilot study with prior informed consent, without whose collaboration the software (eEarlyCare) would not have been possible. The video was edited by Alberto Calvo Rodríguez TVUBU technician and the voice over was done by Caroline Martin, from the Department of English Philology of the University of Burgos.
Access restricted. Please log in or start a trial to view this content.
Materials
| Name | Company | Catalog Number | Comments |
| eEarlyCare software | Authors and University of Burgos. Register number 00/2019/3855 | Computer application to implement SFA | |
| Scale for the measurement of functional abilities in 0-6 years old (SFA) | Authors and University of Burgos. Register number 00/2019/4253 | Scale for the measurement of functional abilities in 0-6 year olds |
References
- Sáiz, M. C. Intervención cognitiva en niños pequeños [Cognitive intervention in early children]. Intervención Temprana: Desarrollo óptimo de 0 a 6 años [Early Intervention: Optimal development from 0-to-6 years old]. Gómez, A., Viguer, P., Cantero, M. J. , Síntesis. Madrid, Spain. 117-133 (2003).
- Bluma, M. S., Shearer, M. S., Frohman, A. H., Hilliard, J. M. Portage Guide to Early Education (2nd Edition). , Cooperative Educational Service Agency. Wisconsin, United States. (1978).
- Josse, D. Escala de desarrollo psicomotor de la primera infancia Brunet-Lézine Revisado [Scale of psychomotor development of early childhood (Brunet-Lézine-Revised)]. Psymtéc. , Madrid, Spain. (1997).
- Newborg, J. Battelle Developmental Inventory, 2nd Edition: Examiner's manual. , Itasca, IL: Riverside, USA. (2005).
- Whitebread, D., Basilio, M. S. Emergencia y desarrollo temprano de la autorregulación en niños preescolares [The emergence and early development of self-regulation in preschool children]. Profesorado. Revista de Currículum y Formación del Profesorado. 16 (1), 1-20 (2012).
- Pérez, Y., Sáiz, M. C. Escala para la medición de habilidades funcionales en edades 0-6 años (EHFI) [Scale for the measurement of functional abilities in 0-to-6-year olds (SFA)]. Registration number 00/2019/4253. , (2018).
- Haley, S. M., Coster, W. J., Ludlow, L. H., Haltiwanger, J. T., Andrellos, P. J. The Pediatric Evaluation of Disability Inventory (PEDI) (2nd ed.). , Pearson Clinical Assessment. Washington, United States. (2012).
- Bronson, M. B. Self-regulation In Early Childhood. , The Guilford Press. NY, United States. (2000).
- Sáiz, M. C., Carbonero, M. A. Metacognitive Precursors: An Analysis in Children with Different Disabilities. Brain Science. 7 (10), 1-14 (2017).
- Sáiz, M. C., Marticorena, R., Arnaiz-González,, Díez-Pastor, J. F. eEarlyCare Computer application. , Burgos, Spain. Registration number 00/2019/3855 (2019).
- Chowdhury, K. Windows Presentation Foundation Development Cookbook. (1st Edition). , Packt Publishing. Birmingham. (2018).
- Nogal, F., Marticorena, R. UBUGrades 2.0. Doctoral Degree dissertation. , Universidad de Burgos. Burgos, Spain. (2018).
- Sáiz, M. C., Marticorena, R., Arnaiz-Gonzalez, Á, Díez-Pastor, J. F., Rodríguez-Arribas, S. Computer application for the registration and automation of the correction of a functional abilities detection scale in early care. Proceeding of INTED2019: 13th annual International Technology, Education and Development Conference. , IATED Academy. Valencia, Spain. 5322-5328 (2019).
- Hartson, R., Pyla, P. S. The UX book: Process and guidelines for ensuring a quality user experience. , Morgan Kaufmann. Amsterdam, Dutch. (2012).
- Bernal, R., Ramírez, S. M. Improving the quality of early childhood care at scale: The effects of "From Zero to Forever". World Development. 118, 91-105 (2019).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5). (5th Edition). , American Psychiatric Association. Arlington, VA, United States. (2013).
Access restricted. Please log in or start a trial to view this content.
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionExplore More Articles
This article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved