
Method Article
A Computer-Based Platform for Aiding Clinicians in Eating Disorder Analysis and Diagnosis
In This Article
Summary
Diagnosing eating disorders in healthcare is challenging. Therefore, the present protocol develops an algorithm based on 949 patient responses to a questionnaire, with the diagnosis displayed on an easy-to-use web-based interface. This system facilitates the accurate diagnosis of eating disorders while excluding those believed to have an eating disorder.
Abstract
Eating disorders (anorexia nervosa, bulimia nervosa, binge-eating disorder, and other specified eating or feeding disorders) have a combined prevalence of 13% and are associated with severe physical and psychosocial problems. Early diagnosis, which is important for effective treatment and prevention of undesirable long-term health consequences, imposes problems among non-specialist clinicians unfamiliar with these patients, such as those working in primary care. Early, accurate diagnosis, particularly in primary care, allows expert interventions early enough in the disorder to facilitate positive treatment outcomes. Computer-assisted diagnostic procedures offer a possible solution to this problem by providing expertise via an algorithm that has been developed from a large number of cases that have been diagnosed in person by expert diagnosticians and expert caregivers. A web-based system for determining an accurate diagnosis for patients suspected to suffer from an eating disorder was developed based on these data. The process is automated using an algorithm that estimates the respondent's probability of having an eating disorder and the type of eating disorder the individual has. The system provides a report that works as an aid for clinicians during the diagnostic process and serves as an educational tool for new clinicians.
Introduction
Dieting and an associated increase in physical activity are the known causes of anorexia nervosa and other eating disorders1. The most common eating disorders mentioned in the diagnostic manual of mental disorders (DSM-5) are anorexia nervosa (AN), bulimia nervosa (BN), binge-eating disorder (BED), and other specified feeding or eating disorder (OSFED)2. These disorders primarily affect females and are accompanied by severe physical and/or psychosocial health complications and distress3. Approximately 13% of females suffer from eating disorders4, and the prevalence of AN in women is estimated at 0.3%-1% throughout their lives, with an even higher percentage of women suffering from BN5.
A multitude of risk factors is associated with specific eating disorders. Dieting during early adolescence and a low body mass index (BMI) increases the risk of AN in females, but early puberty, thin-ideal internalization, body dissatisfaction, negative affect, and social support deficits do not6. Among the factors that predict the onset of BN are weight concerns, body dissatisfaction, drive for thinness, ineffectiveness, low interoceptive awareness, and dieting, but not perfectionism, maturity fears, interpersonal distrust, or BMI6. While there are symptomatic differences between the various types of eating disorders, there is a similarity in the risk factors. This suggests that eating pathology and maladaptive eating behavior (dieting) are common risk factors across all eating disorders.
Indeed, eating pathology is conspicuous in eating disorders. However, the difficulty of defining and quantifying pathological eating behavior, combined with the fact that diagnosis primarily relies on the subjective description of the symptom dimensions, can make the boundaries between diagnoses appear to be unclear7. This issue makes the diagnosis of eating disorders difficult, especially for health practitioners unfamiliar with eating disorder patients, such as primary care physicians.
Health professionals in primary care are often the first to be approached by individuals suffering from an eating disorder. Given the importance of early detection and intervention for a favorable prognosis, care providers must have the tools to help them recognize these disorders. Therefore, a diagnosis must be determined quickly and accurately to prevent delays in their treatment by specialists.
One way of achieving this diagnostic goal is to digitalize and automate questionnaires regarding their symptoms. An added benefit of this method could be that the responses are more truthful since studies suggest patients trust virtual therapists more than human clinicians for discussing mental health issues8. Another potential benefit is increased diagnostic reliability, with some studies suggesting that computer diagnoses can have higher reliability than in-person diagnoses9,10.
In the present protocol, an algorithm has been developed based on the responses to open-end and closed-end questions on physical condition, behavior, emotions, and thoughts by 949 consecutively referred patients (for demographic data, see Table 1). Of the 949 participants, 91.6% (869) were female, 18.0% had AN, 19.0% BN, 13.5% BED, 36.8% OSFED, 6.8% obesity (OB), and 5.9% had no eating disorder (No ED). The algorithm estimates both the probability of having an eating disorder and the conclusion regarding which type of eating disorder the individual has. The questionnaire items are based on DSM-5 criteria for Feeding and Eating Disorders and the diagnostic features of AN, BN, BED, and OSFED. OB (excess body fat) is not included in DSM-5 as a mental disorder. However, there are robust associations between OB and BED2. The questionnaire items are grouped into three categories: (1) Conditions, such as BMI, weight loss/gain during the last year, and self-induced vomiting. (2) Behaviors including eating patterns, dieting, weighing oneself, self-induced vomiting, isolation from friends and family, and avoiding activities. (3) Cognitions/thoughts, such as desired weight, being afraid of losing control, overeating, thoughts about food, believing oneself to be fat when others say you are too thin, and reaction to weight gain. The algorithm is based on an unconditional discriminant analysis that assigns weights to items stepwise, identifying the most discriminating items for each of the five diagnoses. The diagnostic information is displayed on an easy-to-use web-based interface.
Protocol
All work on experimental subjects and patients was approved by the Swedish Ethical Review Authority, Sweden (D. nr: 2019-05505). Before registration in the system, all individuals provided written consent to the storage, handling, and analysis of their data. Patients were referred to the clinic for specialized treatment for eating disorders either by physician's referral or self-referral. Suffering from an eating disorder was the inclusion criteria for the patients.
1. Patient registration by clinicians
NOTE: Patient registration (Figure 1) is completed by a clinician using a developed custom web tool (see Table of Materials).
- Navigate to the web landing page using any modern browser upon patient referral.
- Use an existing account associated with a clinician to log in to the web tool.
- Fill in the patient registration form, including patient ID, social security number, birth date, age, and sex.
- Press the Save button to register a new patient. At this point, the procedure can be paused and then restarted later.
2. Questionnaire for patients
NOTE: The patient fills in the questionnaire on a smart device using a custom app developed in a web tool (see Table of Materials). If the patient is a minor, the questionnaire is filled in by a parent or guardian. Their data is organized in thematic blocks. After the answer to each question is completed, the system presents the next question (Figure 2).
- Open the questionnaire application on a smart device.
- Fill in the social security number for the patients (Figure 3).
- Fill in the first visit date; the current date is used by default.
- Fill in the information corresponding to the patients' weight, height, and age.
- Fill in the information corresponding to behavior such as induced vomiting, snack frequency, and eating rate.
- Fill in the particulars corresponding to cognitive and emotional items such as fear of gaining weight and feelings of body dysmorphia.
- Press the Done button to finish the questionnaire. At this point, the questionnaire can be paused and then restarted later.
3. Risk assessment by clinicians
NOTE: The risk assessment (Figure 4) is retrieved and used by the clinician using a custom web tool (see Table of Materials).
- Navigate to the web landing page using any web browser. Use an existing account to log in to the web tool.
- Search for the patient using the patient's social security number or patient ID.
- Add measured weight and height to the system.
- Press the Result tab to get the algorithmic decision of whether the patient has an ED and, if so, what type of ED.
- Press tab Questions 1-20, or Questions 21-34, to display the questions where the patients' responses deviate from answers by healthy individuals.
- Select a final diagnosis under the Result tab, based on the algorithm and the clinician's expertise.
Results
The patient registration described in step 1 is carried out by a clinician completing the form presented in Figure 1 in the computerized medical records. Once the clinician registers a new patient, the application moves to step 2, which allows the patient to complete the questionnaire. To start the questionnaire, the patient or clinician first needs to input the social security number (or ID) of the patient into the app on a smart device (Figure 3), after which the app displays the first questionnaire item. Figure 2 shows a screenshot of one item from the diagnostic questionnaire. Once a response is selected to a questionnaire item, the application moves to the next item. Patients cannot move back to alter the response of previous questions, and if the questionnaire is prematurely terminated, the responses are still saved, and the user can return to fill in the missing items. Once all questions have been answered, the app is closed automatically.
After the questionnaire has been completed, the risk assessment page presented in Figure 4 is available for the clinician via a web interface. Clinicians can view the recommended diagnosis on the 'Result' page, along with the estimated probability of accuracy from 0-1 (i.e., a 100% range), based on an automatic computation of risk factors of the questionnaire. By pressing either the tab 'Questions 1-20' or 'Questions 21-34', clinicians can view the healthy responses (color turquoise) and the deviating responses (color red) that resulted in the suggested diagnosis (Figure 5). The algorithm (see Table of Materials) estimates both the probability of having an eating disorder and the conclusion regarding which type of eating disorder the individual has. The accuracy of the model is 97.1% for having an ED and 82.8% for ED diagnoses (Table 2). The diagnostic information is displayed on an easy-to-use web-based interface. This information provides clinicians with confidence in their decision if the algorithmic diagnosis agrees with the clinician's own evaluation. If the algorithmic diagnosis does not agree with the clinician's evaluation, the clinician is encouraged to seek a second opinion from other health professionals. The system also allows clinicians to train themselves to become better at diagnosing patients by viewing the specific questions expected to deviate from a healthy individual in the question tabs and by reviewing difficult cases with other health professionals.

Figure 1: An illustration of the patient registration form in the web tool. Please click here to view a larger version of this figure.
{kind=link}

Figure 2: Sample of a single questionnaire item displayed on a smart tablet. Please click here to view a larger version of this figure.
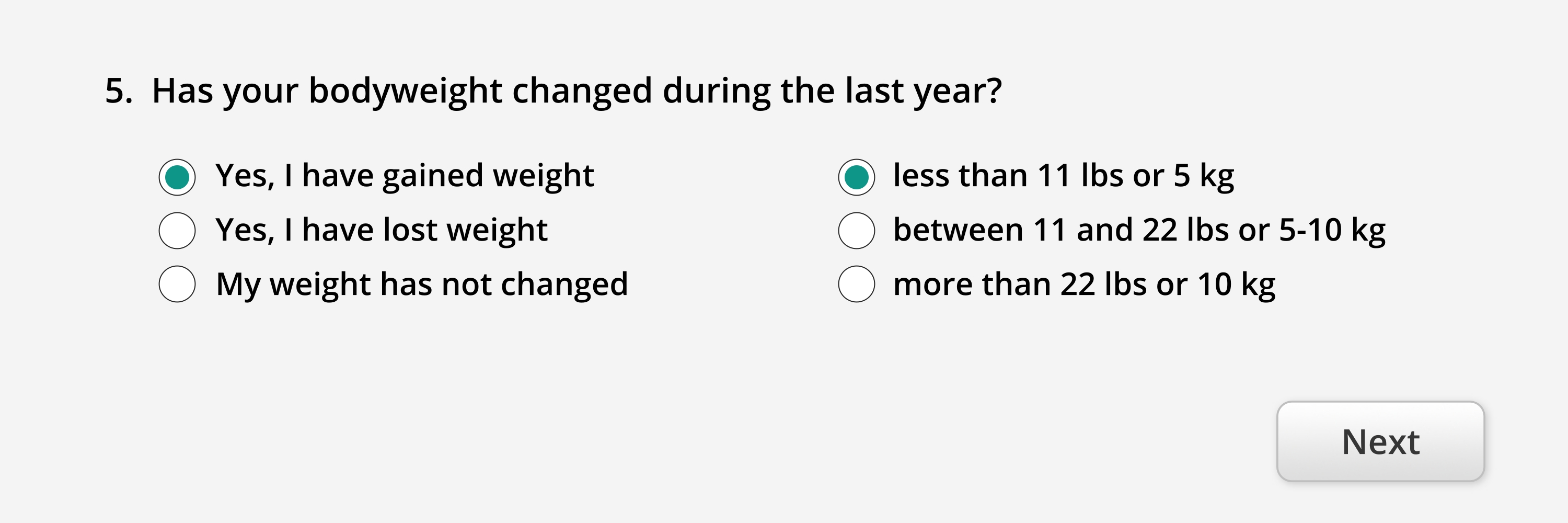{kind=link}

Figure 3: Snapshot of the page asking for the required social security number before completing the diagnosis questionnaire. Please click here to view a larger version of this figure.
{kind=link}

Figure 4: Example of result page with recommended diagnosis and estimated accuracy (in this case 100%) as displayed using the web tool. The result page also shows the date, sex, age, and BMI of the patient. At the top, clinicians can select a diagnosis. Please click here to view a larger version of this figure.
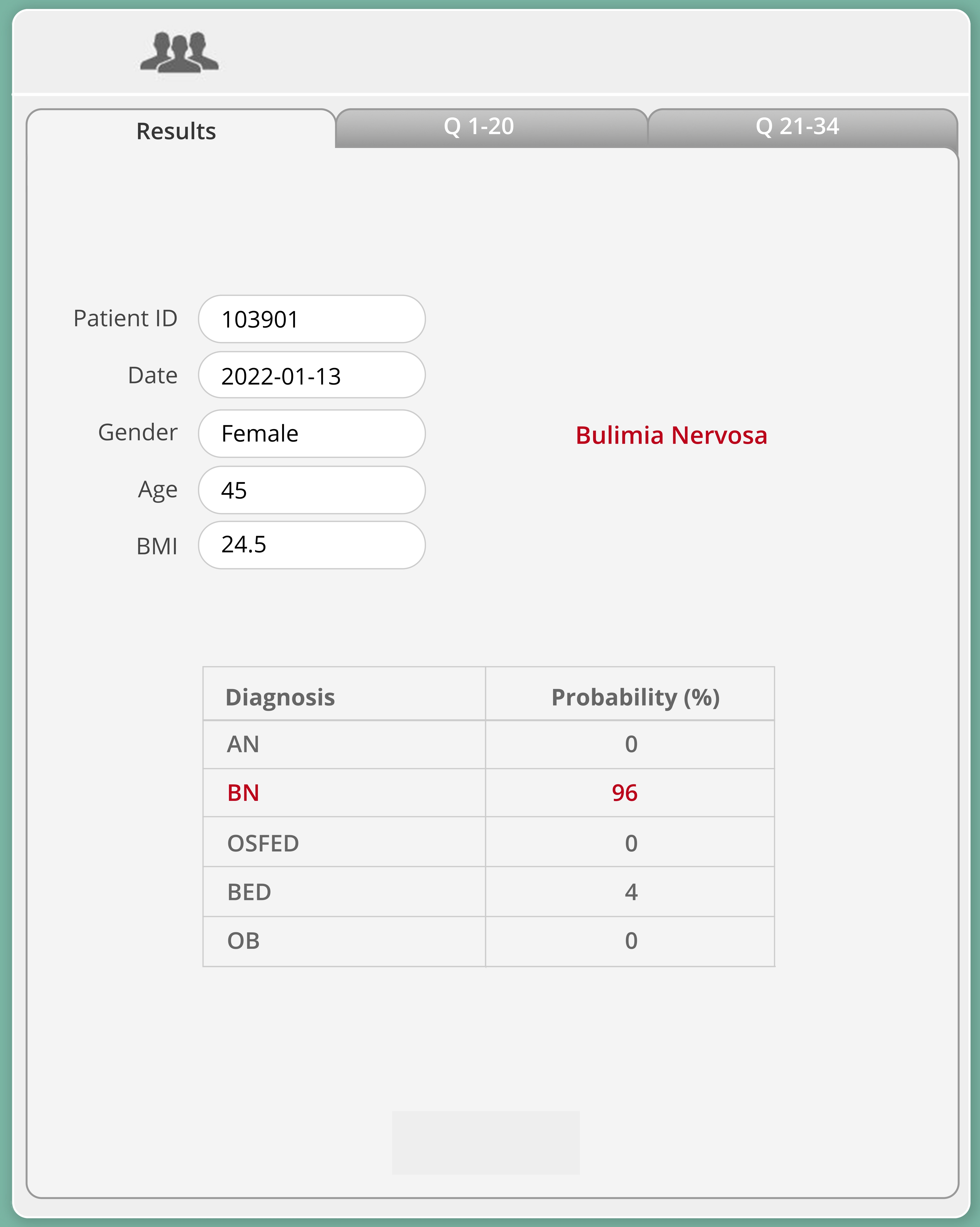{kind=link}

Figure 5: Questionnaire responses and their association with the suggested diagnosis. Red indicates a high association, and teal suggests a low association. Please click here to view a larger version of this figure.
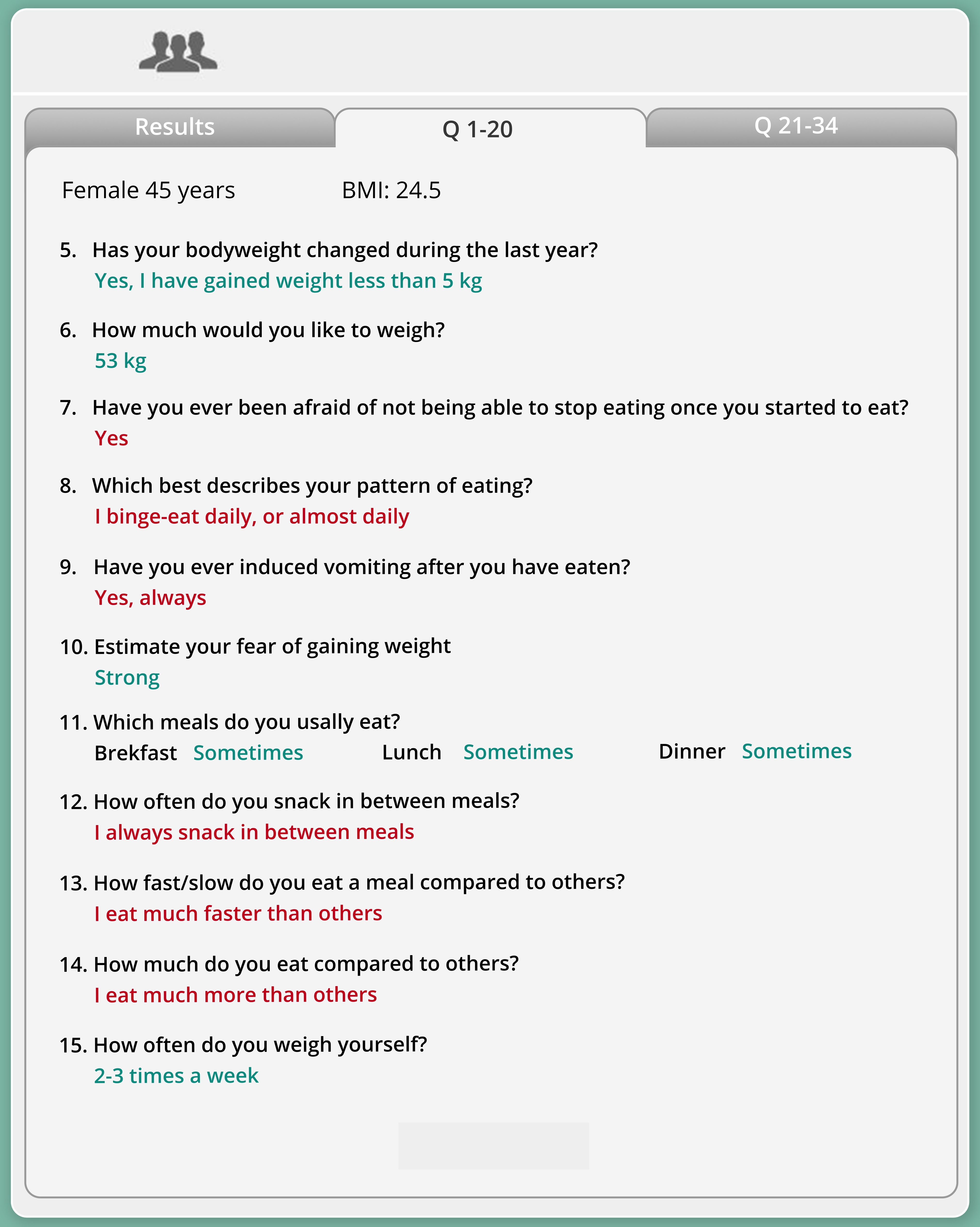{kind=link}
| Female (n = 869) | Male (n = 80) | Total (n = 949) | |
| Age | 21.0 (17.0 - 30.0) | 21.0 (15.0 - 33.5) | 21.0 (17.0 - 30.0) |
| Height | 167.0 (162.0 - 170.0) | 176.5 (169.0 - 183.0) | 167.0 (162.0 - 171.0) |
| Weight | 58.2 (50.0 - 75.0) | 71.5 (57.0 - 97.0) | 59.1 (50.0 - 76.5) |
| BMI | 20.9 (17.8 - 26.7) | 21.3 (18.0 - 31.2) | 21 (17.9 - 27.1) |
Table 1: Demographic data of the 949 patients included for the diagnostic algorithm development. Values are expressed as median (lower quartile - upper quartile).
| Diagnosis | Clinician diagnosis | Algorithm diagnosis | Accuracy (%) |
| AN | 171 | 172 | 87.1 |
| BN | 180 | 181 | 82.2 |
| BED | 128 | 138 | 81.3 |
| OSFED | 349 | 328 | 79.9 |
| OB | 65 | 74 | 90.8 |
Table 2: Number of patients in each ED category diagnosed by a trained clinician and the decision and accuracy of the algorithm.
Discussion
Early and accurate diagnosis of eating disorders is critical to initiating appropriate treatment, improving treatment outcomes, and reducing poor health outcomes1. To determine a diagnosis, clinicians must handle large amounts of psychological and physiological information, and a large amount of data makes diagnosis a time-consuming task with a high risk of misdiagnosis.
The system described here speeds up the decision-making process by providing an automatic questionnaire-based diagnosis. In addition, it allows clinicians to view the specific responses that deviate from the expected responses of a healthy individual. The system was developed with clinicians' needs in mind, which is why the questionnaire is simple enough to be filled in by the patient alone, further reducing the time required by clinicians when considering a diagnosis. For the same reason, responses are saved on input, ensuring the process can be paused at any time. Computer connection issues and other interruptions do not require repeating the entire process.
A limitation to the protocol is that a diagnosis suggestion cannot be calculated unless all questionnaire items have been filled in. Another limitation is that medical measurements, such as blood pressure and peripheral temperature, are not included in the system but must be evaluated by clinicians or medical doctors.
There are several digital tools for eating disorder diagnoses, such as semi-structured electronic interviews11, but there are currently no diagnostic algorithms based on the DSM-5 or the International Classification of Disease, 11th Revision (ICD-11). The primary problem with available approaches is that they do not provide a simple way for clinicians to receive aid in the diagnosis or communicate what constitutes unhealthy responses. The current system is intended for use both in primary care, by health professionals with little knowledge of eating disorders, and in specialist clinics for discussing more complex cases, aiding clinicians in the decision-making process during diagnosis of eating disorders. This system results in improved quality of care, a reduction of time and effort by clinicians, and provides improved efficiency for the clinician in their daily practice.
The diagnostic algorithm is currently based on one questionnaire and allows the system to teach clinicians to diagnose patients better and consult other health professionals in difficult cases. Future development of the system must also include medical data. In addition, the prognostic ability of the algorithm can be improved by refining the questionnaire, replacing redundant, non-informative items with more relevant ones. A longitudinal approach also needs to be considered. If the patient receives appropriate treatment, it is essential to follow their health progression over time. Many items in the questionnaire are still valid for a follow-up approach. However, the questionnaire and algorithm need to be reformulated to create an index to measure health progression.
Disclosures
Complete openness concerning financial arrangements is intended here. Brodin declares that he has no financial interests related to this study. Our research is carried out at the Karolinska Institute, where Södersten is a professor emeritus. The research is translated clinically by Mando Group AB, a company started by Södersten and Bergh, who have 47.5% of the stock each. Professor Michael Leon of the University of California at Irvine has the remaining 5%. Mando Group AB contracts with Region Stockholm every fifth year to treat patients with eating disorders. Mando Group AB signed its first contract in 1997 with Region Stockholm and, since then, its treatment is one of the standards of care offered to the citizens of Stockholm. Mando Group AB won the latest tender and there are now Mandometer Clinics in four Stockholm hospitals. This arrangement is the same as when Region Stockholm contracts with its own clinics to treat patients with all kinds of disease, including eating disorders. That is to say, Region Stockholm provides eating disorders services to the citizens of Stockholm both through a clinic of its own and through Mando Group AB. All healthcare in Sweden is funded through the tax system; private pay is extremely uncommon. It should be added, first, that Mando Group AB is in compliance with the recommendation of the International Committee of Medical Journal Editors on ’Author Responsibilities-Conflicts of Interest', http://www.icmje.org/recommendations/browse/rolesand-responsibilities/. Second, it should also be added that all profit that Mando Group AB has made has been reinvested in research and development and there have been no dividends to stock owners. All of the above is declared in all manuscript submissions and thus far, journals have judged it necessary to publish only some of the details. It seems, however, that the potential ethical problem when scientists translate their research findings into the clinic in a company is not unlike that which arises when any scientist, in an academic setting, is developing a theory and needs further economic funding for his or her work and may receive recognition and financial benefits for the work. The incentive is, in part, economic in this case as well and the ethical ’problem' is similar in both cases. However, the more important incentive is the improvement of the treatment of patients with eating disorders. We are researchers working in an academic setting and like many other medical research institutes today, the Karolinska Institute encourages scientists to translate their research into the clinic in companies that aim to generate financial profits to be used for research and development (https://issuu.com/karolinska_institutet/docs/ki_strategy2030_eng).
Acknowledgements
This work was funded by Region Stockholm.
Materials
| Name | Company | Catalog Number | Comments |
| Computer-Based Platform for Aiding Clinicians in Eating Disorder Analysis and Diagnosis | Mando | Pending assignment | |
| Claris FileMaker Go 19 | Claris | - | For patient registration, custom app for questionnaire, risk assessment |
| iPad 7th generation (2019) | Apple | A2197 |
References
- Treasure, J., Duarte, T. A., Schmidt, U. Eating disorders. Lancet. 395 (10227), 899-911 (2020).
- American Psychiatric Association. . Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. , (2013).
- Smink, F. R. E., van Hoeken, D., Hoek, H. W. Epidemiology of eating disorders: incidence, prevalence and mortality rates. Current Psychiatry Reports. 14 (4), 406-414 (2012).
- Allen, K. L., Byrne, S. M., Oddy, W. H., Crosby, R. D. DSM-IV-TR and DSM-5 eating disorders in adolescents: prevalence, stability, and psychosocial correlates in a population-based sample of male and female adolescents. Journal of Abnormal Psychology. 122 (3), 720-732 (2013).
- Preti, A., et al. The epidemiology of eating disorders in six European countries: results of the ESEMeD-WMH project. Journal of Psychiatric Research. 43 (14), 1125-1132 (2009).
- Stice, E., Gau, J. M., Rohde, P., Shaw, H. Risk factors that predict future onset of each DSM-5 eating disorder: predictive specificity in high-risk adolescent females. Journal of Abnormal Psychology. 126 (1), 38-51 (2017).
- Södersten, P., Brodin, U., Zandian, M., Bergh, C. E. K. Verifying Feighner's hypothesis; anorexia nervosa is not a psychiatric disorder. Frontiers in Psychology. 10, 2110 (2019).
- Lucas, G. M., Gratch, J., King, A., Morency, L. -. P. It's only a computer: Virtual humans increase willingness to disclose. Computers in Human Behavior. 37, 94-100 (2014).
- Hendler, N., Spurgeon, D. Comparison of Clinical Diagnoses Versus Computerized Test Diagnoses using the Maryland Clinical Diagnostics Diagnostic Paradigm (Expert System) for Diagnosing Chronic Pain in the Neck, Back and Limbs. Journal of Anesthesia and Critical Care: Open Access. 6 (5), (2016).
- Richens, J. G., Lee, C. M., Johri, S. Improving the accuracy of medical diagnosis with causal machine learning. Nature Communications. 11 (1), 3923 (2020).
- Dahlgren, C. L., Walsh, B. T., Vrabel, K., Siegwarth, C., Rø, &. #. 2. 1. 6. ;. Eating disorder diagnostics in the digital era: validation of the Norwegian version of the Eating Disorder Assessment for DSM-5 (EDA-5). Journal of Eating Disorders. 8 (1), 1-7 (2020).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved