
Method Article
Measuring the Influence of Magnetic Vestibular Stimulation on Nystagmus, Self-Motion Perception, and Cognitive Performance in a 7T MRT
In This Article
Summary
In this article, we describe the experimental setup, material, and procedures to assess reflexive eye movements, self-motion perception, and cognitive tasks under magnetic vestibular stimulation, as well as the anatomical orientation of the vestibular organs, in a 7 Tesla Magnetic resonance tomography (7T-MRT) scanner.
Abstract
Strong magnetic fields induce dizziness, vertigo, and nystagmus due to Lorentz forces acting on the cupula in the semi-circular canals, an effect called magnetic vestibular stimulation (MVS). In this article, we present an experimental setup in a 7T MRT scanner (MRI scanner) that allows the investigation of the influence of strong magnetic fields on nystagmus as well as perceptual and cognitive responses. The strength of MVS is manipulated by altering the head positions of the participants. The orientation of the participants' semicircular canals with respect to the static magnetic field is assessed by combining a 3D magnetometer and 3D constructive interference in steady-state (3D-CISS) images. This approach allows to account for intra- and inter-individual differences in participants’ responses to MVS. In the future, MVS can be useful for clinical research, for example, in the investigation of compensatory processes in vestibular disorders. Furthermore, it could foster insights into the interplay between vestibular information and cognitive processes in terms of spatial cognition and the emergence of self-motion percepts under conflicting sensory information. In fMRI studies, MVS can elicit a possible confounding effect, especially in tasks influenced by vestibular information or in studies comparing vestibular patients with healthy controls.
Introduction
Strong magnetic fields, i.e., above 1 T, are known to induce dizziness, vertigo, and nystagmus, an effect called magnetic vestibular stimulation (MVS)1,2,3. The vestibular system is located in the inner ear and measures acceleration around rotational axes (yaw, pitch, and roll) with three semi-circular canals and acceleration along translational axes (naso-occipital, inter-aural, and head-vertical) with two macula organs, the utricle, and saccule4 (see Figure 1A). The emergence of the MVS effect can be explained by an ionic current-induced Lorentz force acting on the cupula of the semi-circular canals of the vestibular system1,2.
The effect of MVS increases with higher field strengths3,5. The stimulation is caused by two different components. Firstly, moving the participant into the bore through the B0 field of the MRI scanner results in a dynamic magnetic field that elicits Lorentz forces acting on the cupula. Secondly, the static magnetic field of the MRI scanner in which the participants lie without movement during the experiments also causes a constant Lorentz force. Thus, in all experiments using MRI scanners, the vestibular system of the participant is constantly stimulated by the static magnetic field. This includes all fMRI studies, especially those in ultra-high magnetic fields (> 3 T).
Nystagmus is elicited by being moved or moving, as well as by resting statically in a strong magnetic field. The motion-related forces cause strong nystagmus, which decays after a couple of minutes6. The nystagmus elicited under static magnetic fields is weaker and gradually decreases over time but does not disappear completely during exposure. The direction of the nystagmus depends on the polarity of the magnetic field and reverses upon withdrawal from the magnetic field6,7,8. MVS acts predominately on the horizontal and superior canals, resulting in reflexive eye movements, i.e., mostly horizontal and torsional nystagmus and, to a lesser extent, vertical nystagmus9. In bilateral vestibular patients, no nystagmus can be observed1, and in unilateral vestibular patients, more pronounced vertical nystagmus components are present10. As the nystagmus is involuntary, it is a well-suited measure for the strength of the vestibular stimulation. Nystagmus can be suppressed by visual fixation; therefore, eye movements must be assessed in complete darkness.
Non-veridical self-motion perception, dizziness, and vertigo are often described by participants while being moved into or out of the bore, especially in field strengths above 3 T. The percepts of self-motion have been mostly described as rotations in roll and, to a lesser extent, in yaw and pitch plane7 (see Figure 1A). While nystagmus persists over the length of the exposure, self-motion perception usually disappears after 1-3 min7. The constant part of the MVS is per se an interesting stimulation since it allows for prolonged vestibular input that is not accompanied by conscious self-motion perception.
From studies using caloric or galvanic vestibular stimulation, passive motion, or microgravity, it is known that vestibular information can influence performance in spatial tasks11,12 and its neural correlates13. Being moved or moving inside strong magnetic fields has been reported to influence cognitive performance14,15. One study found that MVS could possibly lead to symptoms of derealization due to non-veridical self-motion perception16. However, studies investigating the influence of resting statically in magnetic fields have not shown conclusive results regarding neuropsychological tasks, except a replicated deterioration in visual accuracy17,18,19,20. Recently, first evidence has been found that MVS can alter spatial attention by inducing a neglect-like bias21. This raises the question of whether MVS can impact performance in behavioral tasks measuring higher cognitive functions. For example, it is unclear to what extent MVS influences spatial reasoning, i.e., the ability to mentalize objects and own-body rotations.
Neuroimaging studies analyzing resting-state activity have shown that MVS can induce changes in default mode networks3,22, which can be explained by subject-specific anatomical orientation of the vestibular organs relative to the magnetic field direction23. In regard to fMRI experiments, the effects of MVS must be carefully considered in the design of the study. Moreover, MVS could interfere with galvanic or vestibular stimulation used in fMRI experiments. It could act as a confounder in neuroimaging studies comparing participants with intact and dysfunctional vestibular systems, as the effects of MVS are absent in bilateral vestibular patients1.
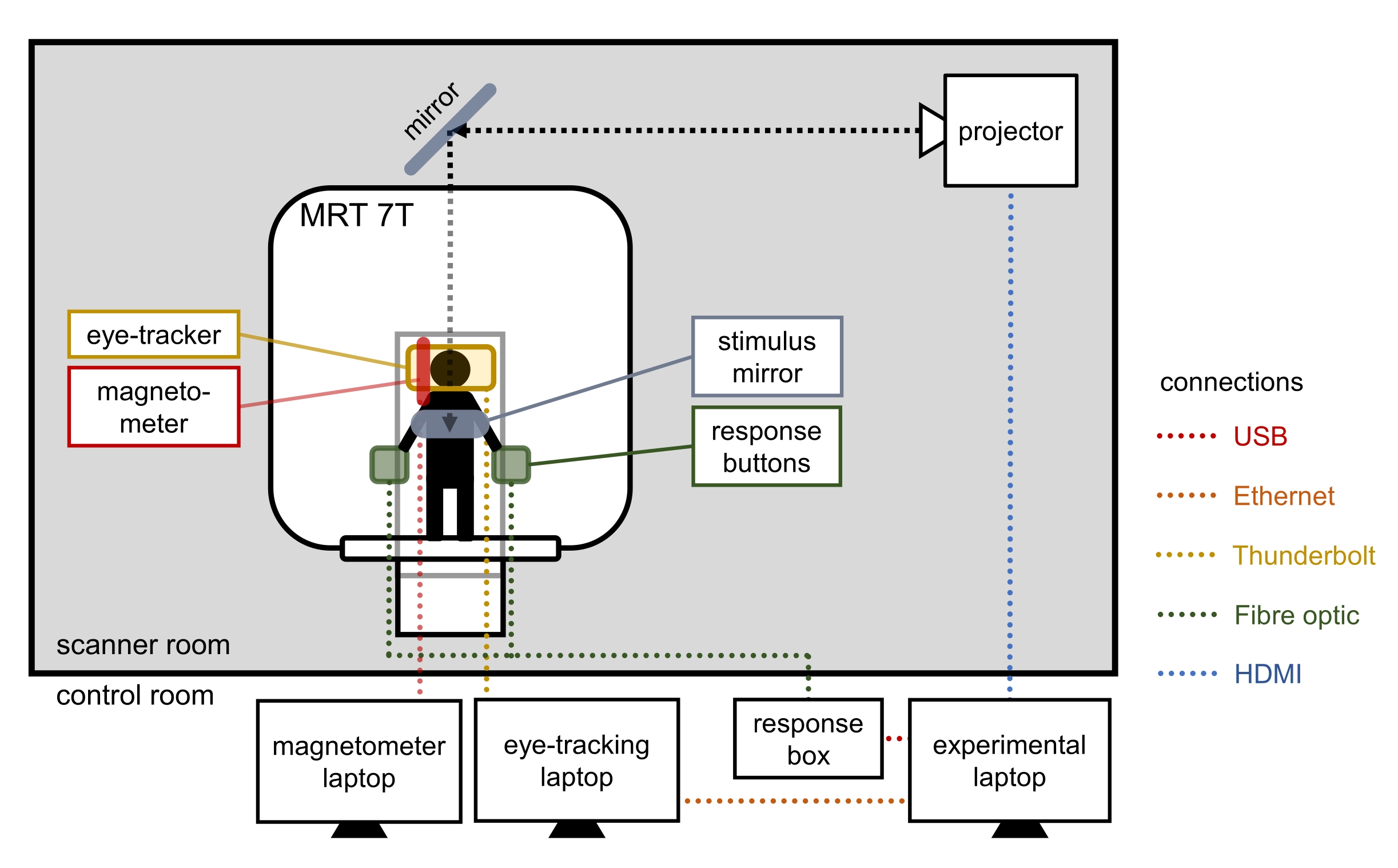
To assess the effects of MVS and compare different strengths of MVS within participants, we here describe an experimental and technical setup to measure nystagmus, self-motion perception, cognitive performance, and the anatomical position of the canals inside a 7 T MRI scanner (see Figure 2). The described setup can be adapted and used for experiments to specifically investigate vestibular and higher cognitive functions under MVS or to assess and control for the possible confounding effects of MVS in fMRI studies.
Interestingly, the strength of MVS can be modulated by changing the head position and, therefore, changing the orientation of the vestibular end organs with respect to the direction of the magnetic field. The effect of MVS can be reduced in most participants by tilting the head forward toward the body (chin to chest)1,24. Thus, changing the head position in the pitch axis allows the comparison of measurable MVS effects under different stimulation strengths.
In this procedure, the strength of MVS was manipulated within participants by comparing measurements between two head positions (see Figure 1B). In the condition that should elicit stronger MVS, the participant was lying supine in the scanner with an approximately earth-vertical orientation of Reid's plane (supine position). In the condition that should elicit weaker MVS, the participant's head was tilted approximately 30° in pitch to the front (tilted position). It is theoretically possible to compare the supine position to a null position where no nystagmus is present1. However, the required pitch tilt for the null position is different for each participant and time-consuming to determine, as this requires several instances of repositioning and moving the participant in and out of the scanner to test the position. This may not be feasible for most study designs. The two head positions, supine and tilted, allow for comparing different measures, e.g., self-motion perception or performance in tasks between and within participants.

Figure 1: Axes and planes of head position in the magnetic field. (A) Head-vertical (HV), inter-aural (IA), and naso-occipital (NO) axis of the head. The direction of the magnetic field (B0) aligns with the head-vertical axis (HV) when participants lie inside the bore in a supine position31. (B) The two head positions during the experiment, with the supine position (lying straight) known to elicit stronger MVS in most participants than the tilted position (head tilted upward in the pitch plane at approximately 30°). Please click here to view a larger version of this figure.
{kind=link}
To determine how the vestibular organs were oriented during the experimental runs without imaging, we attached a 3D magnetometer to the participants' heads and measured the orientation of the probe with respect to the Z-axis of the magnetic field (Figure 3B). The orientation of the vestibular organs in the magnetic field was assessed with a high-resolution anatomical 3D-CISS sequence. During image acquisition, the magnetometer was replaced with a water pipette (Figure 3D). This allowed for extracting the orientation of the magnetometer relative to the direction of the Z-axis of the magnetic field and aligning it to the inner ear structures. We can then draw conclusions about the orientation of the vestibular organs throughout the duration of the experiment.
Nystagmus was tracked with MRI-suitable goggles (Figure 3C). MVS elicits not only horizontal and sometimes vertical but also torsional nystagmus; therefore, it is recommended to use software that also enables the tracking of torsional eye movements9,25.
Self-motion percepts can be assessed during perception7 (while entering and exiting the bore) and after the self-motion percepts vanish, e.g., with questionnaires. It is important to instruct the participants well, as verbally reporting non-veridical self-motion is often difficult for participants. We indicate in the protocol where the self-motion perception and cognitive performance could be measured but do not specify the tasks or questionnaires, as they strongly depend on the research question. We, however, provide example questionnaires and paradigms26.

Figure 2: Technical setup of the experiment. Please click here to view a larger version of this figure.
{kind=link}
In summary, MVS can be used to investigate the influence of vestibular stimulation on nystagmus, perception, and cognitive processes, as well as to study habituation processes in patients with vestibular dysfunction. The effect of the static magnetic field on the cupula remains constant throughout the exposure to the magnetic field. As this simulates a constant rotational acceleration, MVS is an interesting and suitable method to investigate vestibular function and its influence on perception and cognition27,28. It can be used to specifically address research questions concerning the influence of vestibular information on higher cognitive functions, such as spatial reasoning. It serves as a suitable noninvasive model for unilateral failure of the vestibular system, which enables the study of compensatory processes that may arise in vestibular patients28. Furthermore, it is important to consider the confounding effects of MVS in fMRI studies, as behavioral and neural correlates can be altered by vestibular stimulation and also interfere when investigating vestibular patients in a strong static magnetic field.
Protocol
The following steps were part of a study that conformed to the Declaration of Helsinki and was approved by the ethics committee of the Canton Bern, Switzerland (2019-02468). All participants gave their written informed consent prior to study participation.
NOTE: It is recommended to assess participants' vestibular function before the MVS experiment with standard vestibular diagnostic tests such as questionnaires (e.g., dizziness handicap inventory29), bithermal caloric tests, rotatory pendular tests, head impulse tests (HIT), subjective visual vertical (SVV), vestibular evoked myogenic potentials (c-VEMP), ocular vestibular myogenic potentials (o-VEMP), dynamic visual acuity (DVA), and/or dynamic posturography.
1. Preparation of the experimental setup in the scanner room (Figure 2)
CAUTION: All materials brought inside the scanner room must be MRI safe.
- Connect the experimental computer and the eye-tracking computer with a crossover ethernet cable to enable the synchronization of data collection.
- Connect the response buttons operated by the participant with the experimental computer via the response box.
- Switch on the projector connected to the experimental computer.
- Connect the magnetometer device to the magnetometer computer by plugging it into the USB connector.
NOTE: The 3D magnetometer must be suitable and calibrated for ultra-high field strength. In the software used in this study, the following settings were chosen: Units = Tesla, Range = 20.00, Acquisition rate = 100.00 Hz. - Connect the eye-tracking goggles to the eye-tracking computer with a shielded firewire cable.
NOTE: Unless the cable is long enough, the eye-tracking computer screen must be seen from inside the scanner room to enable adjustments of the eye-tracking goggles. If necessary, use an external screen placed in front of the window between the MRI room and the control room. - Open the eye-tracking software9,25.
2. Preparation of the participant for entering the MRI scanner
CAUTION: The following steps are critical for participant and staff safety.
- Let the participant read and sign the informed consent.
- Confirm that participant does not meet MRI exclusion criteria. Provide MRI-safe clothing, remove metallic objects (e.g., piercings), and provide a pregnancy test (if applicable).
NOTE: For MR safety criteria, see https://mr-gufi.de/index.php/dokumente. The criteria vary between research sites. - Remove contact lenses, eyeshadow, and mascara thoroughly (for better eye-tracking).
3. Informing the participant about experimental procedures and tasks
- Explain the experimental procedure and give instructions about the tasks. Let the participant complete practice trials (if applicable).
- If self-motion perception is assessed, inform the participant about specific translation and rotation axes (see Figure 1A). Use memorable terms for the specific movements, e.g., "barbecue rotation" for rotations in yaw (around the head-vertical axis) in the supine position26.
4. Preparation of eye-tracker and magnetometer measurements
- Put an elastic headband and EEG cap on the participant's head (e.g., an MRI-safe EEG cap without electrodes) (see Figure 3A).
- Fix the magnetometer behind one ear (must be in the range of the 3D-CISS sequence images) by pulling it under the elastic headband and the EEG cap. Fix it appropriately with adhesive tape (see Figure 3B).
- Put on the eye-tracking goggles over the EEG cap (see Figure 3C).
- Let the participant insert ear plugs.
- Adjust the eye-tracking parameters on the goggles (left/right centering, up/down centering, focus) and in the software (left/right centering, up/down centering, pupil size, contrasts, iris pattern) to ensure good tracking.

Figure 3: Preparation of the participant. (A) Elastic headband and EEG cap (without electrodes) for fixing the magnetometer. (B) The magnetometer is placed behind one ear. (C) Eye-tracking goggles are mounted. (D) The magnetometer probe is removed and replaced with a water pipette for imaging. Please click here to view a larger version of this figure.
{kind=link}
5. Recording the eye-tracking calibration file
NOTE: Calibration would be most precise if done before every run and in the position in which the participant is moved into the scanner. The here-reported procedure is less precise but was chosen due to time and technical constraints.
- Let the participant sit 1 m in front of calibration stimuli (measure the eye-stimulus distance with, for example, a tape measure).
- Adjust the eye-tracking parameters in the software (pupil size, contrasts, iris pattern) for good tracking.
- Press Record to start data acquisition.
- Let the participant look at every dot for 1 s (five dots in total, three in a row, one above the middle, one beneath the middle, distance of dots 10 cm) with verbal instruction: left, down, mid, up, right.
- Press Stop to stop data acquisition.
6. Measuring spontaneous nystagmus before entering the scanner
NOTE: Measurements are most precise when taking place outside the magnetic field in the supine position. This could be carried out with a detachable MRI bed. If not available, as in the setup used in this study, a position outside the 50 mT line (dashed line on the floor) should be chosen. The strength of the magnetic field at the position of the measurement can be assessed with the magnetometer (0.02 T in the setup used here).
- Put the goggles cover on and ensure the participant cannot see any light. Otherwise, let participant cover their head with black fabric to eliminate any light coming in.
- Adjust the eye-tracking parameters in the software (pupil size, contrasts, iris pattern) for good tracking. Tell the participant to open their eyes widely.
- Press Record to start data acquisition.
- Measure the eye movements for at least 30 s. Readjust the eye-tracking parameters if necessary.
- Press Stop to stop data acquisition.
- Take the goggles cover off.
7. Positioning the participant for the experiment
- Let the participant lie down on the scanner bed.
- Adjust the head-tilt position of the participant according to the first condition (either supine or tilted upward in the pitch plane at approximately 30°) by using appropriate cushions.
- Place the mirror over the participant's head and adjust it so the screen is inside the participant's field of view.
- Give the participant the response buttons for each hand; if necessary, fix them with tape.
- Let the participant practice putting on and taking off the cover of the goggles so that this can be done in the dark inside the bore; the participant should repeat this for as long as necessary and finish with the cover on the goggles.
NOTE: This step can lead to the displacement of the goggles, which can affect measurements regarding the position of the eyes. If possible, perform a calibration after this step. - Repeat the instructions for the first task and ask the participant if the instructions are understood.
- Adjust the eye-tracking parameters either on the goggles or in the software (pupil size, contrasts, iris pattern) for good tracking.
- Adjust the MRI bed's starting position with the help of the MRI scanner's laser cross to ensure the participant's inner ear structures will be in the center of the bore during the experiment.
8. Moving the participant into the scanner
- If applicable, start the self-motion perception paradigm by pressing Run and entering the participant and trial information in the experimental software on the experimental computer.
- Start the eye-tracking measurements (in the setup used here, this was started by the self-motion perception paradigm) by pressing Record in the eye-tracking software. Tell the participant to open their eyes widely.
- Start the magnetometer measurements by pressing Record in the magnetometer software.
- Tell the participant that the run is starting.
- Inside the scanner room, start to move the participant into the bore.
- After 3 min, percepts of self-motion should have vanished in most participants. Therefore, tell the participants to take the goggles' cover off if visual stimuli need to be presented (e.g., a questionnaire).
NOTE: Eye-tracking can also be continued for a longer time with covered eyes. - If applicable, present a self-motion questionnaire on the screen by starting it by pressing Run on the experimental computer and letting the participant answer via response buttons.
9. Presenting a paradigm with a cognitive task
- If applicable, present a paradigm with a cognitive task on the screen by starting it by pressing Run on the experimental computer and letting the participant answer via response buttons. Assess the magnetometer orientation during this time.
NOTE: Now, different tasks can be implemented for the participant to conduct. Let the participant take the cover of the goggles on and off to change between eye-tracking and screen-based paradigms.
10. Moving the participant out of the scanner
- Let the participant put the cover of the goggles on.
- Repeat steps 8-9 (except step 8.5., which is "move the participant out of the bore")
11. Switch the head position
- Switch the head position to the position not yet assessed using the appropriate cushions (either supine or tilted) and repeat steps 8.2-11.
NOTE: If an appropriate MRI bed is available, an interesting variation could be to move participants into the bore with their feet first, as reversed entry into the bore reverses the field direction relative to the inner ear.
12. Assessment of the orientation of the vestibular organs
- Remove the mirror and goggles without displacing the magnetometer.
- Install the head coil.
- Remove the probe of the magnetometer and replace the probe with a pipette filled with water without displacing the cover of the magnetometer (see Figure 3D).
- Place the participant's head inside the head coil without displacing the magnetometer.
- Move the participant into the scanner.
- Acquire a 3D-CISS sequence for structural inner ear imaging.
NOTE: In this study, the following parameters were used: a slice thickness of 0.4 mm; a field of view of 179 mm × 179 mm; a flip angle of 60°; a repetition time (TR) of 8.29 ms; and an echo time (TE) of 3.81 ms. The acquisition time of this 3D-CISS was 10 min 53 s. Different sequences have been used in other studies23,30. - Move the participant out of the MRI scanner.
13. End of study
- Remove the pipette, cap, headband, and ear plugs, and leave the scanner room with the participant.
- If applicable, let the participant fill out a questionnaire (e.g., self-motion perception, experienced differences between conditions, other experiences).
- Debrief the participant about the investigated research questions (e.g. measuring effects of MVS on nystagmus, self-motion perception and cognitive tasks by manipulating head position in reference to the magnetic field).
Results
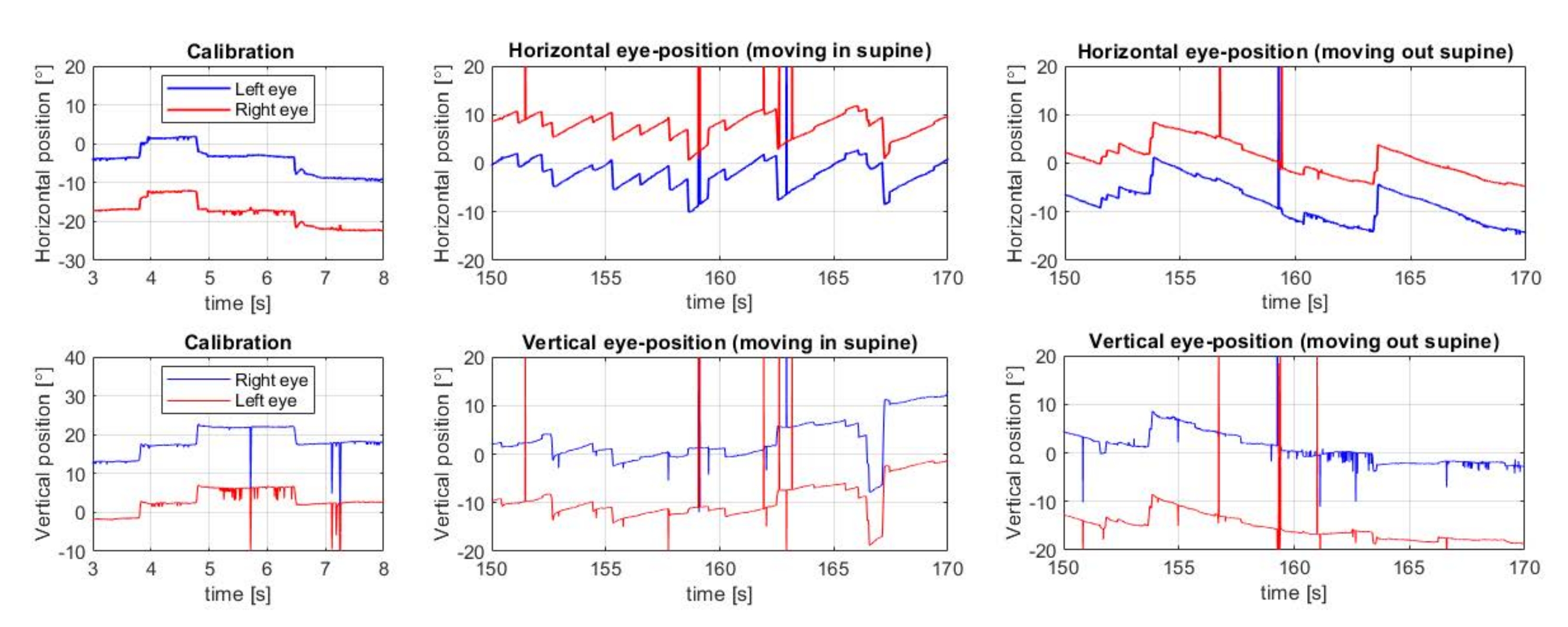
The eye-tracking data show the captured horizontal and vertical eye movements (see Figure 4). Tracking torsional eye movements (not shown) requires specific software9,25 and/or sophisticated postprocessing. Calibration recordings are used to transform units from pixels to degrees. The data are of good quality if a steady tracking (with approx. 100 Hz) is reached, and the extracted data show only minor tracking artifacts (see Figure 4 for an example of minor artifacts, mostly due to blinking). Spontaneous nystagmus outside the MRI scanner should be assessed before the experiment to exclude nystagmus due to other reasons than the magnetic field.

Figure 4: Eye-tracking data. Horizontal and vertical eye positions during calibration and moving into and out of the MRI scanner in the supine head position. Data show the horizontal nystagmus, which reverses between moving into and out of the bore. Please click here to view a larger version of this figure.
{kind=link}
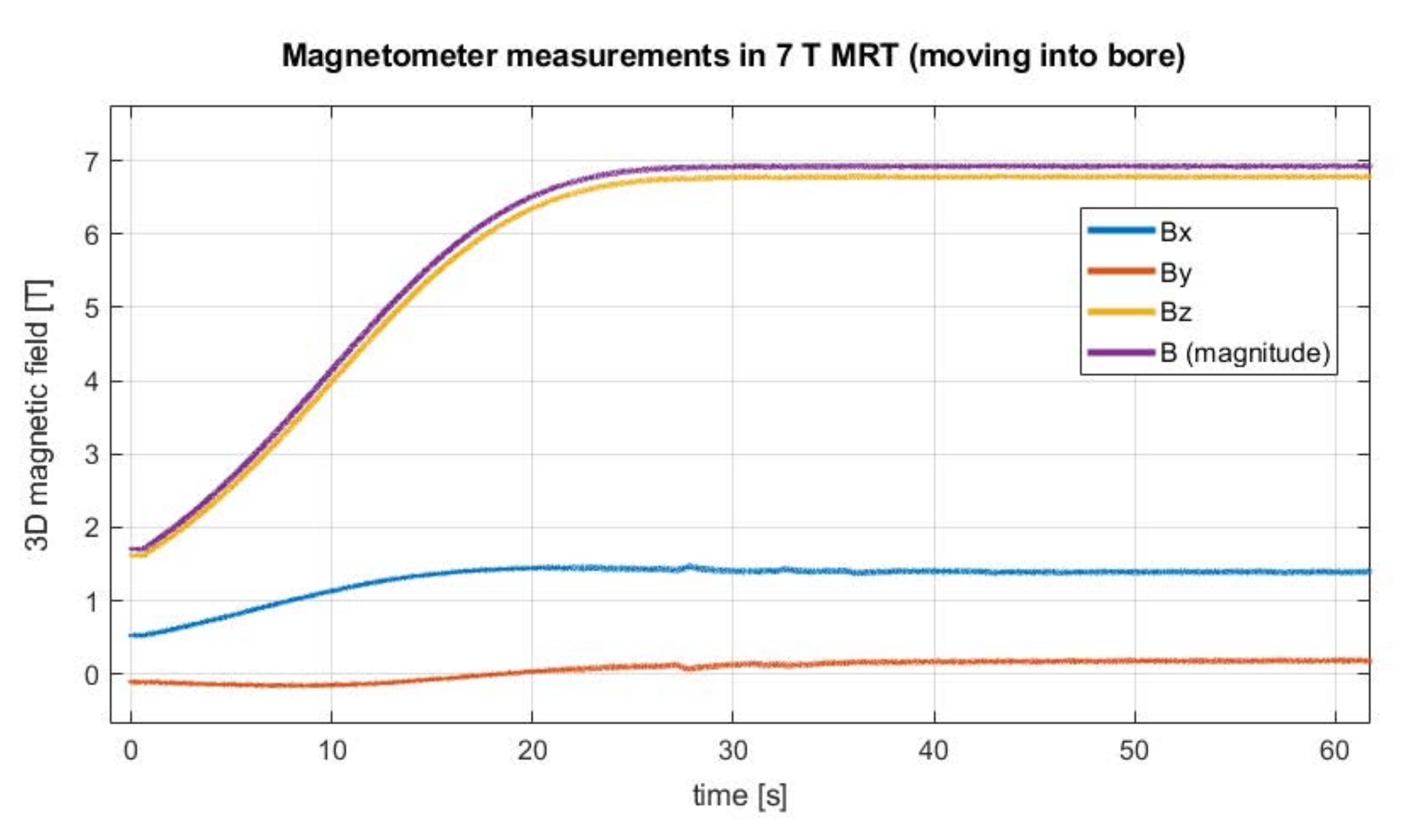
The magnetometer data show the position of the magnetometer probe in relation to the Z-axis of the magnetic field inside the bore (Figure 5). Ideally, the tracked data look smooth and show no alterations in field strengths in each rotation axis after reaching the inside of the bore. Thus, significant head movements of the participants can be detected easily.

Figure 5: Magnetometer data. Data from the 3D magnetometer moving into the bore show a maximum field strength of almost 7 T after approximately 27 s. No movement artifacts are visible, indicating that the participant did not make head movements while entering the bore. Please click here to view a larger version of this figure.
{kind=link}
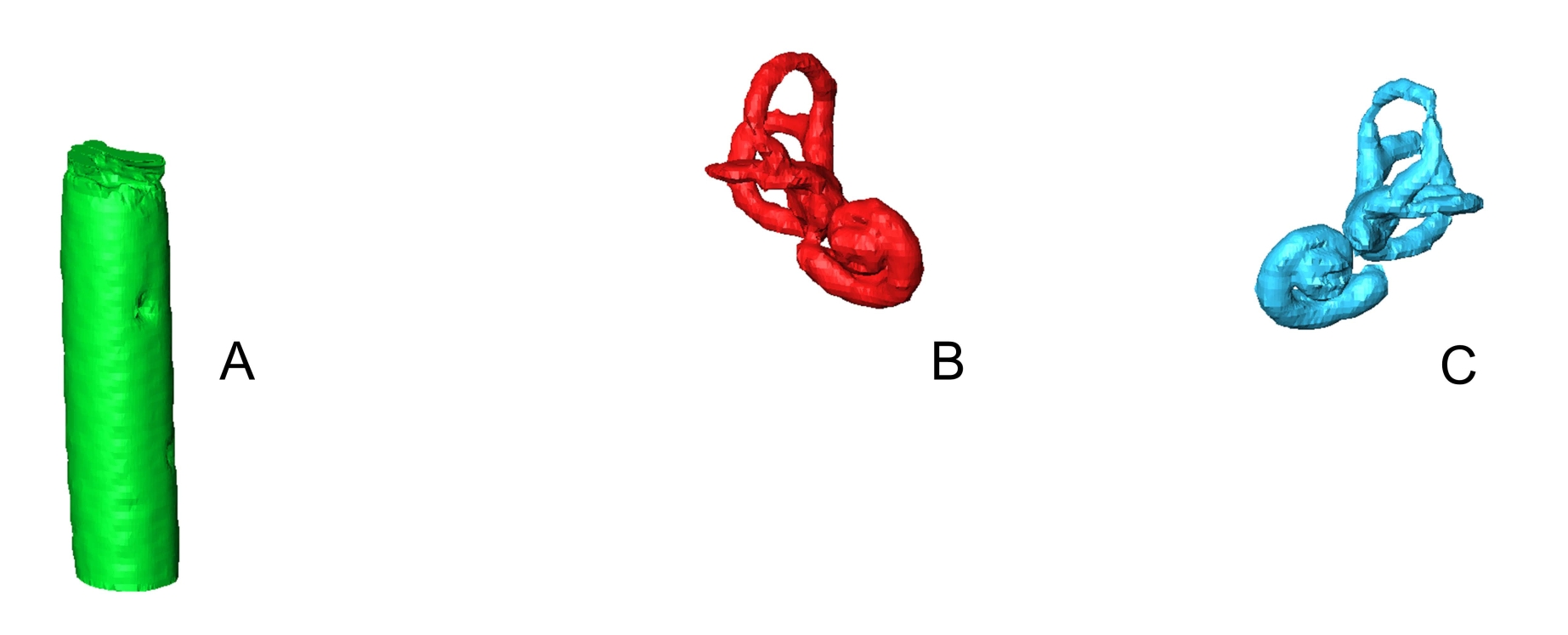
The 3D-CISS sequence was acquired with a 7 T MRI scanner. From the 3D-CISS images, the 3D surface models of the left and right inner ears and the magnetometer orientation were extracted (see Figure 6). The surface models were generated using medical image processing and visualization software. This allows for extracting the orientation of the semi-circular canals with respect to the magnetometer orientation and the Z-axis of the magnetic field during the experiment (see Figure 7).

Figure 6: 3D surface models extracted from the 3D CISS image. (A) Water pipette at previous magnetometer position; (B) right (red) and (C) left (blue) inner ear structure (original positions and proportions). Please click here to view a larger version of this figure.
{kind=link}

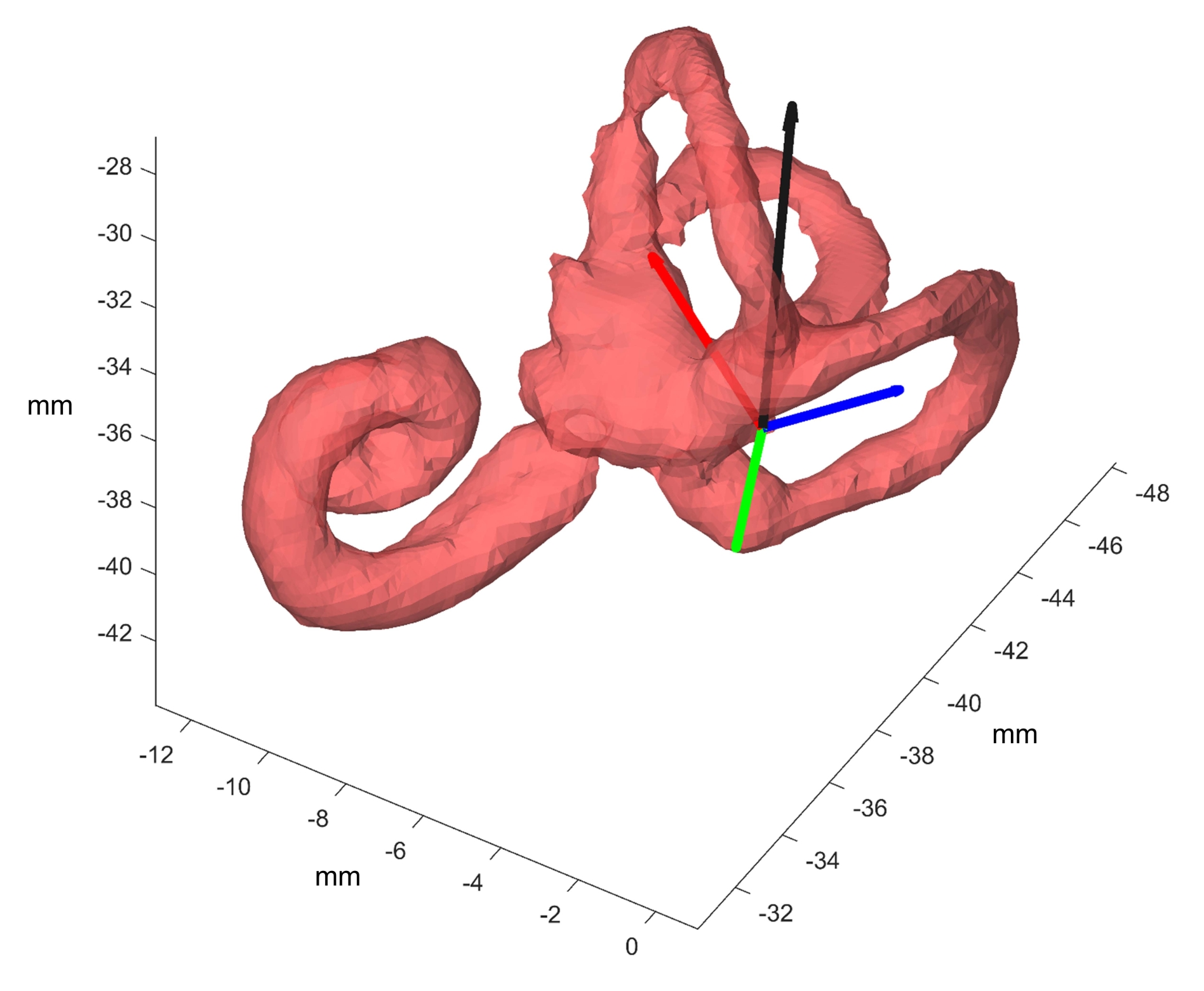
Figure 7: Orientation of the semi-circular canals as extracted from the 3D-CISS image. For every semi-circular canal, three landmarks are chosen, and a surface normal vector is calculated (horizontal canal: green, posterior canal: red, superior canal: blue). This vector is brought into relation with the orientation of the water pipette (black) as a proxy for the magnetometer probe orientation and with the Z-axis of the magnetic field (not depicted here). Units in millimeters (mm) (absolute coordinates of the MR image). Please click here to view a larger version of this figure.
{kind=link}
The orientation of the canals and the magnetometer with respect to the Z-axis of the MRI scanner from the 3D-CISS images can be combined with the orientation of the magnetometer during the two runs without imaging. This allows the reconstruction of the canal orientation during MVS exposure under different head positions. Alternatively, a picture of every participant and the attached magnetometer could be taken outside the magnetic field. Then, the external facial structures could be reconstructed to map the magnetometer orientation measures with inner ear structures and the direction of the magnetic field. Data of self-motion percepts and cognitive tasks (not described here) can be analyzed together with the above data. Thus, canal position, eye-tracking data (horizontal, vertical, and torsional nystagmus), as well as reported self-motion percepts and behavioral results, can be linked to answer the specific research question of the experiment.
Discussion
The reported setup is suited to investigate various aspects of MVS effects on nystagmus, self-motion perception, and performance in cognitive tasks. Combining the measures of the elicited MVS response could give insights such as how the brain processes conflicting vestibular information and show how vestibular information influences perceptual and cognitive processes on the inter-and intra-individual level. In contrast to other vestibular stimulation methods, such as rotational chairs, MVS elicits a constant acceleration stimulus, making it suitable for longer-lasting behavioral studies and use as a noninvasive model for unilateral failure8,28. Therefore, this approach could provide insights into the interplay between vestibular information and cognitive processes in terms of spatial cognition and the emergence of self-motion percepts under conflicting sensory information. In the future, the use of MVS can be exploited in clinical research, for example, to investigate acute stage early compensation to vestibular imbalance during exposure to MVS. These findings could then be connected to compensation mechanisms after vestibular lesions. The comparison of participants with normal and dysfunctional vestibular organs could foster knowledge about adaptation processes in vestibular patients to the altered incoming vestibular information.
The described procedure includes critical steps for safe and accurate data acquisition in a 7 T MRI scanner. First, the MRI environment poses several difficulties. The experimental setup must be MRI safe, which may require changes in the eye-tracking goggles or cable connections in comparison to a non-MRI setup. This can lead to compromises in data quality. Also, the participants must meet the MRI inclusion criteria and should tolerate the inconvenience of the process (e.g., tilting the head while lying in the MRI scanner for several minutes). Second, eye-tracking in the scanner, especially the acquisition of torsional nystagmus, is difficult and requires specialized software25. For torsion, the pattern of the iris is used for tracking, which requires high-quality images and is also influenced by differences in individual iris patterns. Another approach could be using artificial pigment markers on the sclera3, which can be unpleasant for the participant. Third, self-motion percepts due to MVS are non-veridical and, thus, imply intra-vestibular as well as multisensory conflicts28. Therefore, the verbalization of these head and/or body rotation and translation experiences are often difficult to describe for participants. Clear instructions adapted to the research question are of crucial importance. We recommend using well-known rotation and translation terms to which participants can relate, thus enabling them to better describe their perceptual experience. For assessing specific motion parameters, more fine-grained methods can be used, such as ratings of rotation velocity over time7.
The presented setup is limited by the technical constraints of our equipment and could be improved if these could be overcome. For example, to assess not only static but also dynamic head position inside the bore, the magnetometer data could also be synchronized with eye-tracking and behavioral data. The calibration of the goggles would be better if repeated before every run. Also, the length of the eye-tracking cable is of importance, as this defines if spontaneous nystagmus can be measured outside the scanner room. The best solution would be a detachable MRI bed, which can be moved outside the magnetic field. However, the eye-tracking computer screen must be seen from inside the scanner room to enable the calibration and fine-tuning of the eye-tracking parameters while having access to the goggles. In our case, we solved that via a second screen rotated toward the scanner room window.
MVS could affect performance and brain responses in fMRI studies. In studies comparing vestibular patients with healthy controls, MVS could lead to group differences because of a difference in stimulation strength instead of other patient characteristics. For the purpose of controlling confounding MVS effects, the current setup is a time-consuming process both timewise and financially (equipment). Alternatively, tilting the head upward for small angles7, 23 (to the extent allowed by the head coil) or assessing covariates, such as the orientation of the vestibular organs with MRI as described above23,30 and/or nystagmus (e.g., recent fMRI-based eye-tracking approaches32), could be of use.
Disclosures
No conflicts of interest.
Acknowledgements
We thank the participants and the MR team, as well as the reviewers whose valuable comments improved the quality of the manuscript. We thank D. S. Zee for his valuable advice. We are grateful that DIATEC AG provided an eye-tracking laptop for the experiment. The project is supported by a SITEM-Insel support grant from the University of Bern awarded to FWM and GM.
Materials
| Name | Company | Catalog Number | Comments |
| 3D Magnetometer | Metrolab Technology, Switzerland | THM1176-HF | Calibrated for 7 Tesla, with fibre optic cable, CE-labelled |
| AMIRA 6.3 (Software) | Thermo Fisher Scientific, USA | Medical image processing and visualization software | |
| Celeritas Fiber Optic Response Box Unit | Psychology Software Tools | Response box | |
| Celeritas Fiber Optic Response Unit | Psychology Software Tools | PST-100761 | Response buttons, 5 buttons for each hand |
| Ear plugs | |||
| EEG cap | Any MRI safe EEG cap is suitable | ||
| Elastic band | Used to fixate the Magnetometer behind the ear | ||
| Ethernet cable (crossover) | Daetwyler | Uninet 5502 flex 4P FRNC/LSOH 522830.01 | |
| Ethernet cable adapter | TP-Link | UE305 | |
| Experimental laptop | Computer with enough performance, with Response Buttons software (e.g. Celeritas), software for running paradigm (e.g. MATLAB, PsychToolBox), Ethernet cable link to eye-tracking computer | ||
| Eye-tracking Goggles (Visual Eyes) | Interacoustics | 515b | Micromedical goggles with infrared camera: Point Grey Firefly, CE-labelled, modified for 7 Tesla, shielded firewire cable |
| Eye-tracking laptop | Computer with enough performance, with eye-tracking software (e.g. OpenIris), Ethernet cable link to experimental computer | ||
| Headband | MRI safe headband | ||
| Magnetom Terra 7T MRI Scanner | Siemens Healthcare, Erlangen Germany | Located at Translational Imaging Center (TIC) in the Swiss Institute of Translational and Entrepreneurial Medicine (sitem-insel AG) in Bern, Switzerland | |
| Magnetometer laptop | Computer with enough performance, with magnetometer software (e.g. EZMag3D) | ||
| MATLAB R2017b (Software) | MathWorks | Experimental paradigm can be run e.g. with PsychToolBox (Brainard, D. H., & Vision, S. (1997). The psychophysics toolbox. Spatial vision, 10(4), 433-436.) | |
| Metrolab EZMag3D v1.1.2 (Software) | Metrolab Technology, Switzerland | 3D magnetometer software: https://www.metrolab.com/resources/downloads/ | |
| MRI-Mirror | Siemens Healthcare, Erlangen Germany | ||
| OpenIris (Software) | Software to record and analyse the eye movements within the MRI-scanner. Reference: Otero-Millan, J., Roberts, D.C., Lasker, A., Zee, D.S., Kheradmand, A. Knowing what the brain is seeing in three dimensions: A novel, noninvasive, sensitive, accurate, and low-noise technique for measuring ocular torsion. Journal of Vision. 15 (14), 11, doi: 10.1167/15.14.11 (2015). | ||
| Pregnancy test | e.g. early pregnancy test stripes (10 mIU/mL) | ||
| Projector system | Hyperion Psychology Tools | ||
| Triangle Cushion | Siemens Healthcare, Erlangen Germany |
References
- Roberts, D. C., et al. MRI magnetic field stimulates rotational sensors of the brain. Current Biology. 21 (19), 1635-1640 (2011).
- Ward, B. K., Roberts, D. C., Della Santina, C. C., Carey, J. P., Zee, D. S. Vestibular stimulation by magnetic fields. Annals of the New York Academy of Sciences. 1343 (1), 69-79 (2015).
- Boegle, R., Stephan, T., Ertl, M., Glasauer, S., Dieterich, M. Magnetic vestibular stimulation modulates default mode network fluctuations. NeuroImage. 127, 409-421 (2016).
- Goldberg, J. M., et al. The Vestibular System: A Sixth Sense. , Oxford University Press. Oxford, UK. (2012).
- Antunes, A., Glover, P. M., Li, Y., Mian, O. S., Day, B. L. Magnetic field effects on the vestibular system: Calculation of the pressure on the cupula due to ionic current-induced Lorentz force. Physics in Medicine and Biology. 57 (14), 4477-4487 (2012).
- Glover, P. M., Li, Y., Antunes, A., Mian, O. S., Day, B. L. A dynamic model of the eye nystagmus response to high magnetic fields. Physics in Medicine and Biology. 59 (3), 631-645 (2014).
- Mian, O. S., Li, Y., Antunes, A., Glover, P. M., Day, B. L. On the vertigo due to static magnetic fields. PloS One. 8 (10), 78748(2013).
- Jareonsettasin, P., et al. Multiple time courses of vestibular set-point adaptation revealed by sustained magnetic field stimulation of the labyrinth. Current Biology. 26 (10), 1359-1366 (2016).
- Otero-Millan, J., Zee, D. S., Schubert, M. C., Roberts, D. C., Ward, B. K. Three-dimensional eye movement recordings during magnetic vestibular stimulation. Journal of Neurology. 264, Suppl 1 7-12 (2017).
- Ward, B. K., Roberts, D. C., Della Santina, C. C., Carey, J. P., Zee, D. S. Magnetic vestibular stimulation in subjects with unilateral labyrinthine disorders. Frontiers in Neurology. 5, 28(2014).
- Grabherr, L., et al. Mental own-body and body-part transformations in microgravity. Journal of Vestibular Research: Equilibrium and Orientation. 17 (5-6), 279-287 (2007).
- van Elk, M., Blanke, O. Imagined own-body transformations during passive self-motion. Psychological Research. 78 (1), 18-27 (2014).
- Klaus, M. P., et al. Vestibular stimulation modulates neural correlates of own-body mental imagery. Journal of Cognitive Neuroscience. 32 (3), 484-496 (2020).
- Heinrich, A., et al. Cognition and sensation in very high static magnetic fields: A randomized case-crossover study with different field strengths. Radiology. 266 (1), 236-245 (2013).
- Van Nierop, L. E., Van Slottje, Z., Kromhout, V. Effects of MRI related magnetic fields on cognitive performance. Occupational and Environmental Medicine. 70, 83(2013).
- Martínez-Gallardo, S., Miguel-Puga, J. A., Cooper-Bribiesca, D., Bronstein, A. M., Jáuregui-Renaud, K. Derealization and motion-perception related to repeated exposure to 3T magnetic resonance image scanner in healthy adults. Journal of Vestibular Research. 31 (2), 69-80 (2021).
- Chakeres, D. W., Bornstein, R., Kangarlu, A. Randomized comparison of cognitive function in humans at 0 and 8 Tesla. Journal of Magnetic Resonance Imaging. 18 (3), 342-345 (2003).
- De Vocht, F., et al. Cognitive effects of head-movements in stray fields generated by a 7 Tesla whole-body MRI magnet. Bioelectromagnetics. 28 (4), 247-255 (2007).
- Heinrich, A., et al. Effects of static magnetic fields on cognition, vital signs, and sensory perception: A meta-analysis. Journal of Magnetic Resonance Imaging. 34 (4), 758-763 (2011).
- Van Nierop, L. E., Slottje, P., Van Zandvoort, M. J. E., De Vocht, F., Kromhout, H. Effects of magnetic stray fields from a 7 Tesla MRI scanner on neurocognition: A double-blind randomised crossover study. Occupational and Environmental Medicine. 69 (10), 759-766 (2012).
- Lindner, A., Wiesen, D., Karnath, H. -O. Lying in a 3T MRI scanner induces neglect-like spatial attention bias. eLife. 10, 71076(2021).
- Boegle, R., Ertl, M., Stephan, T., Dieterich, M. Magnetic vestibular stimulation influences resting-state fluctuations and induces visual-vestibular biases. Journal of Neurology. 264 (5), 999-1001 (2017).
- Boegle, R., Kirsch, V., Gerb, J., Dieterich, M. Modulatory effects of magnetic vestibular stimulation on resting-state networks can be explained by subject-specific orientation of inner-ear anatomy in the MR static magnetic field. Journal of Neurology. 267, 91-103 (2020).
- Mian, O. S., Li, Y., Antunes, A., Glover, P. M., Day, B. L. Effect of head pitch and roll orientations on magnetically induced vertigo. Journal of Physiology. 594 (4), 1051-1067 (2016).
- Otero-Millan, J., Roberts, D. C., Lasker, A., Zee, D. S., Kheradmand, A. Knowing what the brain is seeing in three dimensions: A novel, noninvasive, sensitive, accurate, and low-noise technique for measuring ocular torsion. Journal of Vision. 15 (14), 11(2015).
- Wyssen, G. Measuring the influence of magnetic vestibular stimulation on reflexive eye-movements, self-motion perception, and cognitive performance in a 7T MRT. OSF. , (2022).
- Ward, B. K., et al. Magnetic vestibular stimulation (MVS) as a technique for understanding the normal and diseased labyrinth. Frontiers in Neurology. 8, 122(2017).
- Ertl, M., Boegle, R. Investigating the vestibular system using modern imaging techniques-A review on the available stimulation and imaging methods. Journal of Neuroscience Methods. 326, 108363(2019).
- Jacobson, G. P., Newman, C. W. The development of the dizziness handicap inventory. Archives of Otolaryngology - Head and Neck Surgery. 116 (4), 424-427 (1990).
- Go, C. C., et al. Persistent horizontal and vertical, MR-induced nystagmus in resting state Human Connectome Project data. NeuroImage. 255, 119170(2022).
- Dmitry, L., et al. Raw data repository for the article "Spatially resolved fluorescence of caesium lead halide perovskite supercrystals reveals quasi-atomic behavior of nanocrystals" [Data set]. Zenodo. , (2022).
- Son, J., et al. Evaluating fMRI-based estimation of eye gaze during naturalistic viewing. Cerebral Cortex. 30 (3), 1171-1184 (2020).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionExplore More Articles
This article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved