
Auscultation
Overview
Source: Jaideep S. Talwalkar, MD, Internal Medicine and Pediatrics, Yale School of Medicine, New Haven, CT
Through auscultation, the clinician is able "to eavesdrop on the workings of the body" to gain important diagnostic information.1 Historically, the term "auscultation" was synonymous with "immediate auscultation," in which the examiner's ear was placed directly against the patient's skin. Although this was standard practice for centuries, the method proved inadequate in nineteenth-century France, due to social norms and suboptimal diagnostic yield. This led René Laënnec to invent the first stethoscope in 1816 (Figure 1), a tool that has since become inseparable from auscultation in modern clinical practice, and patients hold it as a symbol of honor and trustworthiness among those who carry them.2
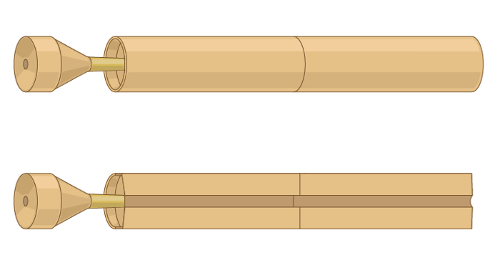
Figure 1. A representative illustration of the first stethoscope invented by René Laënnec.
The stethoscope has undergone many technologic advances since Laënnec's initial hollow wooden tube. Practically speaking, the provider must understand the difference between the two sides of the modern stethoscope's chest piece: the diaphragm and the bell (Figure 2).
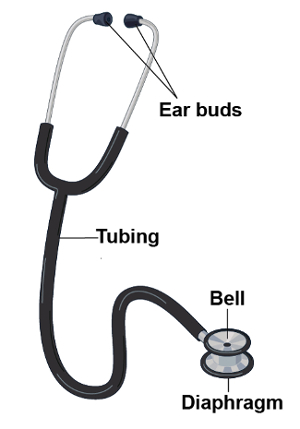
Figure 2. Parts of a modern stethoscope.
When applied firmly against the patient's skin, the diaphragm transmits high frequency sounds. Sounds from within the patient vibrate the membrane of the diaphragm. These vibrations result in the propagation of sound through the column of air inside the stethoscope and into the examiner's ears. Conversely, when applied lightly, the bell transmits low frequency sounds. The bell acts as a cup that directly transmits sounds from within the patient through the tubing of the stethoscope. Pressing more firmly with the bell can stretch the underlying skin, essentially turning it into a diaphragm. Auscultation is used in a wide variety of clinical settings. It most commonly plays a role in the examination of the chest, heart, abdomen, and vasculature.
Procedure
- Throughout the entirety of the patient encounter, use your un-aided sense of hearing to identify findings that may be diagnostically useful (e.g., hoarse voice or grunting with expiration).
- Before patient contact, decontaminate the stethoscope by wiping it with a 70% alcohol pledget, a standardly available antiseptic rinse used for hand hygiene, or a hospital surface disinfectant.3
- Positioning of the stethoscope
- Place the stethoscope ear buds in your ears with the tips pointing forwa
Application and Summary
This video covered the general considerations related to auscultation during the physical examination. Auscultation is typically done with the aid of a stethoscope, though certain findings, especially on the respiratory examination, may be evident to the un-aided ear. While specific stethoscope techniques vary based on each individual portion of the exam, in all circumstances, the clinician must hold the stethoscope properly and recognize the difference between the bell and the diaphragm in order to optimize the diagnost
References
- Markel, H. The Stethoscope and the Art of Listening. New England Journal of Medicine. 354: 551-553 (2006)
- Jiwa, M., Millett, S., Meng, X., and Hewitt, V.M. Impact of the Presence of Medical Equipment in Images on Viewers' Perceptions of the Trustworthiness of an Individual On-Screen. Journal of medical Internet research. 14 (4), e100 (2012).
- Makim, D.G. Stethoscopes and Health Care-Associated Infection. Mayo Clinic Proceedings. 89: 277-280 (2014).
Skip to...
Videos from this collection:

Now Playing
Auscultation
Physical Examinations I
60.3K Views

General Approach to the Physical Exam
Physical Examinations I
115.7K Views

Observation and Inspection
Physical Examinations I
93.2K Views

Palpation
Physical Examinations I
82.7K Views

Percussion
Physical Examinations I
99.7K Views

Proper Adjustment of Patient Attire during the Physical Exam
Physical Examinations I
83.2K Views

Blood Pressure Measurement
Physical Examinations I
107.4K Views

Measuring Vital Signs
Physical Examinations I
113.9K Views

Respiratory Exam I: Inspection and Palpation
Physical Examinations I
156.7K Views

Respiratory Exam II: Percussion and Auscultation
Physical Examinations I
212.2K Views

Cardiac Exam I: Inspection and Palpation
Physical Examinations I
175.8K Views

Cardiac Exam II: Auscultation
Physical Examinations I
139.4K Views

Cardiac Exam III: Abnormal Heart Sounds
Physical Examinations I
91.4K Views

Peripheral Vascular Exam
Physical Examinations I
68.0K Views

Peripheral Vascular Exam Using a Continuous Wave Doppler
Physical Examinations I
38.5K Views
Copyright © 2025 MyJoVE Corporation. All rights reserved