
Aby wyświetlić tę treść, wymagana jest subskrypcja JoVE. Zaloguj się lub rozpocznij bezpłatny okres próbny.
Method Article
Muscle Function Obtained with Motion Mode Ultrasound and Surface Electromyography during Core Endurance Exercise
W tym Artykule
Podsumowanie
This protocol uses motion mode ultrasound and surface electromyography simultaneously to measure muscle function of the core. Muscle thickness and activation of the local stabilizers (e.g., transverse abdominis, internal oblique) and global movers (e.g., external oblique) is achievable during specific time points of the side plank and dead bug exercises.
Streszczenie
Motion mode (M-mode) ultrasound allows researchers and clinicians to measure the change of muscle thickness across time. Muscle thickness can be measured between fascial borders at a given time point during an exercise. This selected time point produces a one-dimensional image resulting in real-time, live observation of anatomy. Ultrasound used during functional movement can be referred to as dynamic ultrasound; this is feasible and reliable with the use of a linear transducer, elastic belt, and foam block to secure consistent transducer placement. The lateral abdominal wall is commonly investigated using ultrasound due to the overlapping nature of the muscles. Surface electromyography (sEMG) can complement M-mode ultrasound imaging because it measures the electrical representation of muscle activation. There is minimal evidence using M-mode ultrasound and sEMG simultaneously during core exercise. Exercises that challenge the core musculature involve both isometric holds (e.g., side plank), as well as oscillatory extremity movements (e.g., dead bug). In this study, both instruments will be used simultaneously to measure core muscle function during exercise. Ultrasound measurements will be obtained using a linear transducer and ultrasound unit, and sEMG measurements will be acquired from a wireless sEMG system. To make comparisons between participants and exercises, normalization methods using static, exercise starting positions for both instruments will be used. An activation ratio will be used for ultrasound and calculated by dividing the contracted thickness (thickness during a time point of exercise) by the rested (starting position) thickness. Muscle thickness will be measured in centimeters from the superior inferior fascial border to inferior superior fascial border. These methods aim to offer an innovative and practical measurement of muscle function with M-mode ultrasound and sEMG during core endurance exercises.
Wprowadzenie
The lateral abdominal wall is made up of the transverse abdominis, internal oblique, and external oblique1. The lateral abdominal wall contracts concentrically, eccentrically, and isometrically to withstand the forces placed on the body1. The co-contraction of this muscle group provides stabilization of the center of the human body2,3. These muscles are important during the prevention and rehabilitation of lower extremity injuries because poor trunk function is associated with increased hip adduction and knee valgus, which are risk factors for lower extremity injuries4,5. Focusing on strengthening and increasing muscular endurance of the core musculature not only decreases risk factors for the lower extremity but can also decrease low back pain6. Recently, it has been recommended that individuals who are suffering from acute and chronic low back pain should include trunk strengthening, endurance, and specific trunk muscle activation in their rehabilitation6. An example of specific trunk muscle activation is targeting isolated or grouped trunk muscles using co-contraction to restore control or increase coordination of the lumbopelvic-hip region6.
Two ways to objectively measure muscle function are the use of motion mode (M-mode) ultrasound and surface electromyography (sEMG). M-mode ultrasound provides a real-time visualization of muscle and fascia movement during a recorded time which can display onset and extent of the motion7. The distance between the superior inferior fascial border and inferior superior fascial border are measured at a selected time to obtain muscle thickness. Muscle thickness during a specific time point of an exercise can be divided by resting thickness to achieve an activation ratio8. sEMG provides insight into muscle activation and fatigue, as the output can be compared to the muscle's maximum contraction9. These two instruments and methods have been used previously to measure the onset of hip muscle activation during a variety of exercises in healthy and injured individuals10. Exercises that target the trunk, and specifically the lateral abdominal wall, are the side plank and dead bug11,12,13. The side plank is performed in a side lying position with the elbow directly underneath the shoulder and forearm on the ground, the hips are raised off the ground until the spine is in a neutral position. The knees are extended, and the feet are placed on top of one another9 (Supplemental Figure 1). The dead bug is performed in a supine position with both arms straight above and the hips and knees flexed in a 90° angle. The exercise begins when one arm is flexed above the head and the contralateral leg extends. The opposite arm and leg remain in a neutral position and then flex and extend once the original moving arm and leg return to the neutral position13 (Supplemental Figure 2 and Supplemental Figure 3).
The activation of the external oblique has been seen to range from 37% to 62% of maximum voluntary isometric contraction (MVIC) during the side plank11,12,14. During the dead bug, the activation of the external oblique has been recorded between 20% to 30% of MVIC for only five repetitions of the exercise15. The internal oblique and transverse abdominis, the deeper abdominal muscles of the lateral abdominal wall, activate between 22% to 28% of MVIC during the side plank12,14. Due to the overlapping nature of the internal oblique and transverse abdominis, the two muscles have been combined during sEMG collection14. A limitation of sEMG is the crosstalk from adjacent muscles, where the sEMG sensor may be producing an output of a different muscle, resulting in a false understanding of activation16. Muscle thickness measurements obtained with ultrasound can be used to mitigate this limitation, and this measurement is feasible during trunk exercises, such as the isometric holds previously mentioned17.
Muscle thickness of the lateral abdominal wall has been recorded during the side plank as an absolute magnitude of difference between contracted thickness and rested thickness. At the 30 s time point of a side plank, the muscle thickness of the internal oblique and external oblique increased by 0.526 mm and 0.205 mm, respectively17. These measurements were recorded in brightness mode ultrasound at one time point during the side plank. B-mode ultrasound is commonly performed to assess before and after images; however, this method only allows for measurement at two time points18. M-mode ultrasound provides increased advantages compared to B-mode ultrasound, as it can detect onset of muscle activation as well as muscle thickness during the entirety of the exercise with any time point able to be selected for measurement18. Therefore, the overall goal of the current protocol is to provide an innovative and practical measurement of muscle function with M-mode ultrasound and sEMG during core endurance exercises. This is beneficial to researchers and clinicians to understand how muscles function throughout the duration of an exercise, especially of an endurance nature, as opposed to a measurement isolated to a single time point.
Protokół
All human participants provided informed consent. The protocol was part of a study approved by the Institutional Review Board of the University of Central Florida. Inclusion criteria included ages 18 -45 and physically active according to ACSM guidelines (30 min of moderate to vigorous activity 5 days per week)19. Exclusion criteria included low back pain within the past year, current hip, upper, or lower extremity pain or injury, a year history of low back surgery or lower extremity surgery, self-reported balance disorder, muscular abnormalities, currently pregnant, or having an open wound in the abdominal area (Table 1).
1. Data collection instrument preparation
- Check the integrity of the ultrasound machine and sEMG machine (see Table of Materials).
- Turn on the ultrasound machine, press Patient, and add a new patient. Click New Patient and enter the patient identification number. Select MSK exam type > Abdominal preset and press Register. Press Exit.
- Turn on the tablet (see Table of Materials) and click the EMG recording application. Click the Menu button in the top left screen and scan for sensors. Take the sensor out of the base and hover over the activation button. Once the sensor is connected with the application, create a new folder with the participant's identification number.
NOTE: Ultrasound settings in Abdominal Preset, B-mode: B color = Tint Map D, Write Zoom Height = 4, Write Zoom Width = 4, Thermal Index = Tls, ATO Level = Low, Focus Number = 2, Focus Number CrossXBeam = 2, Focus Depth = 50, Depth (cm) = 3, Compression = 1, Focus Width = 1, Focus Width CrossXBeam = 1, Line Density = 3, Line Density CrossXBeam = 3, Suppression = 0, Frame Average = 4, From Average CrossXBeam = 2, CrossXBeam = 2, CrossXBeam # = Low, CrossXBeam Type = Mean, Edge Enhance = 3, B Steer = 0, Gray Scale Map = Gray Map C, Gain = 34, Dynamic Range = 69, Rejection = 0, Frequency (MHz) = 12. Ultrasound settings in Abdominal Preset, M-mode: sweep speed = 0, M color = Tint Map C, Dop Display Format = Vert ½ B, Rejection = 0, Compression = 1, Gray Scale Map = Gray Map D, M Gain (delta from B) = 0.
2. Surface electromyography preparation (see Table of Materials)
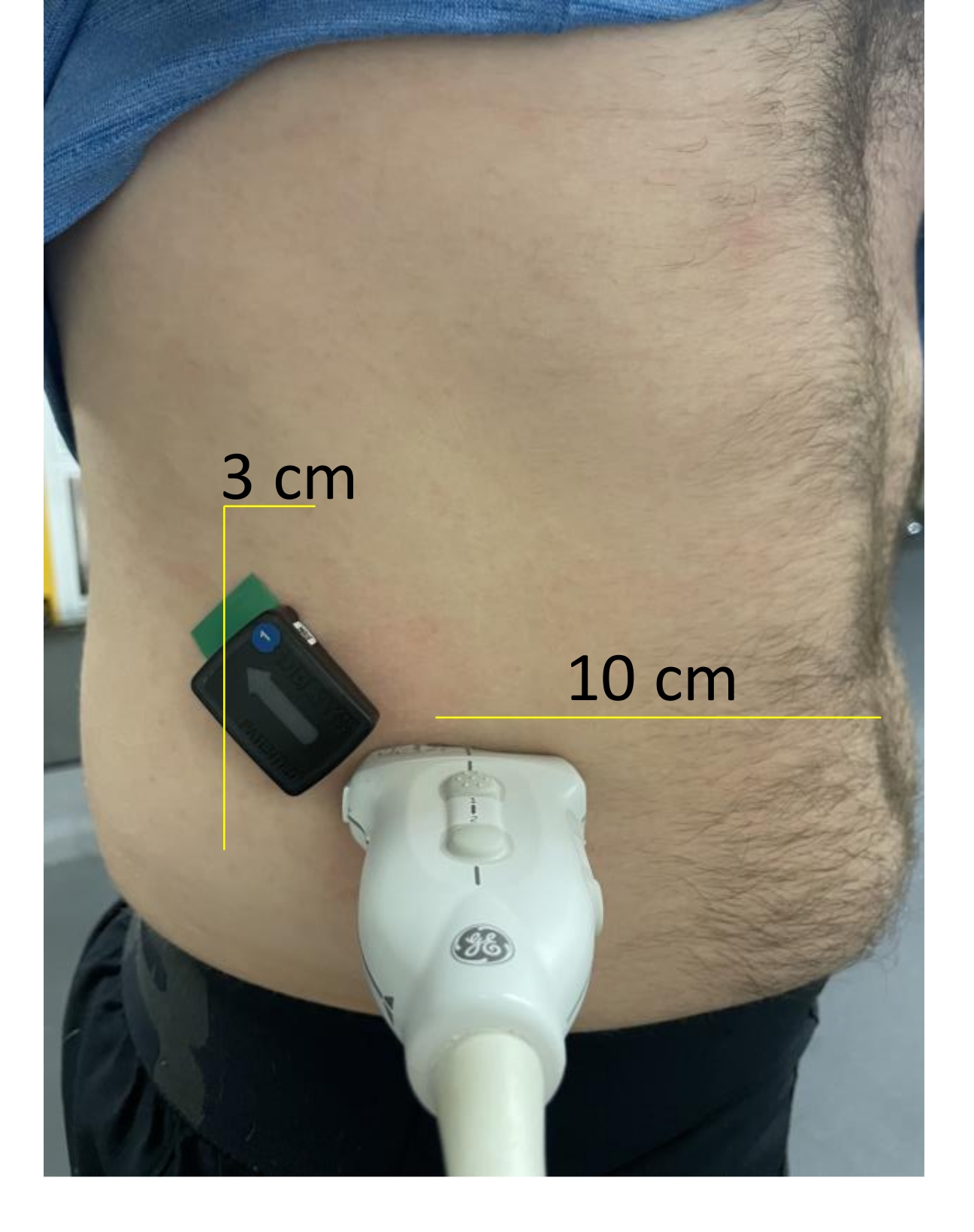
- Determine the external oblique sensor location by palpating the right iliac crest and right inferior rib while the participant is supine hook-lying (Figure 1). Place the sensor 3 cm anterior from the midway point between the lower rib and the iliac crest, parallel to the muscle fibers20.
- Shave, clean, and debride the area of the skin where the sensor (see Table of Materials) will be placed. Add adhesive (see Table of Materials) to the sensor and secure onto skin.

Figure 1: Examination location of the lateral abdominal wall. The sEMG sensor is placed 3 cm anterior from the midway point between the lower rib and the iliac crest, parallel to the muscle fibers20. The transducer is located 10 cm lateral to the umbilicus until the lateral abdominal wall is visible on the screen. Please click here to view a larger version of this figure.
{kind=link}
3. Ultrasound preparation (see Table of Materials)
- In a standing position, place the transducer through the elastic belt and foam block (Figure 2).
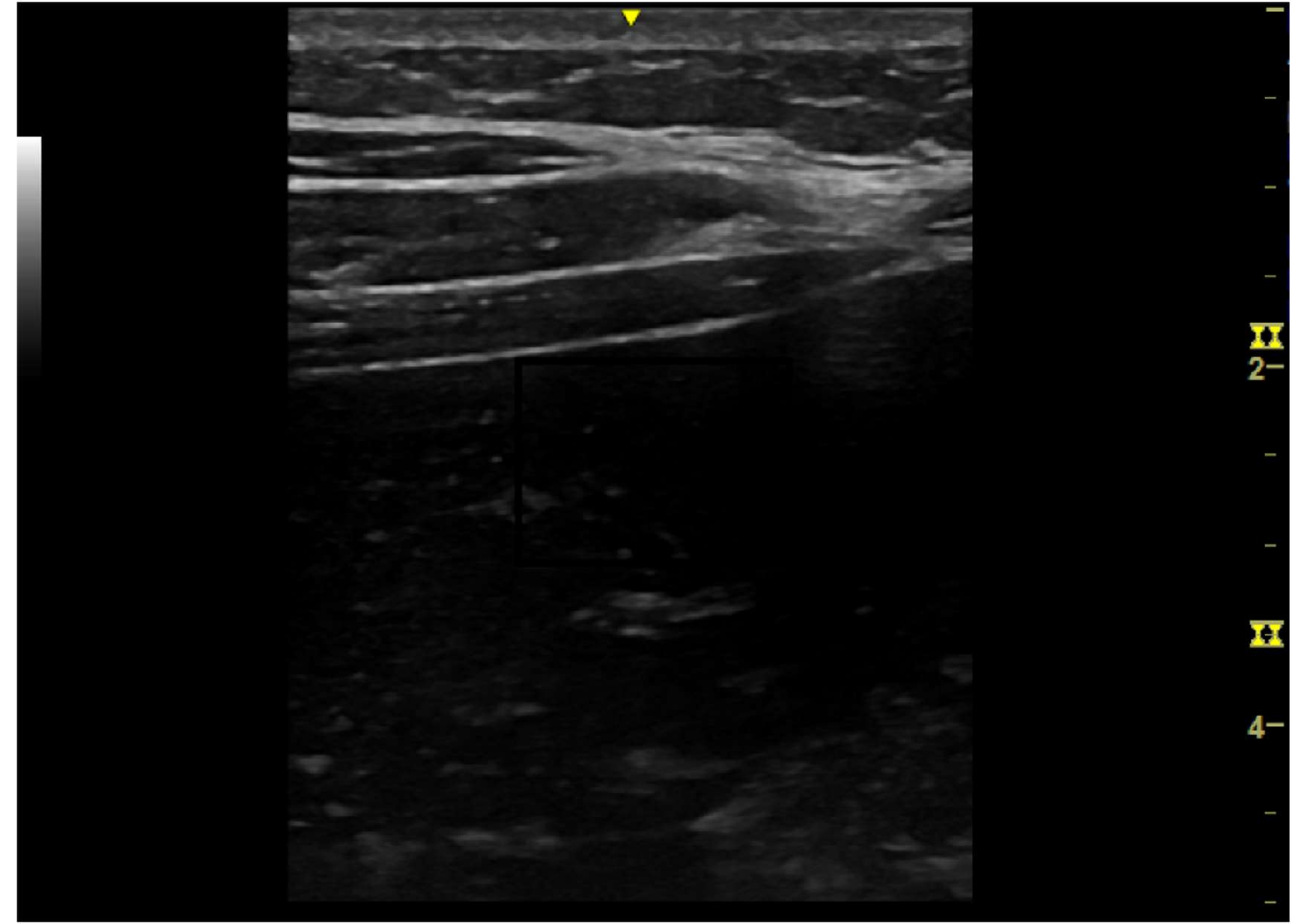
- Add gel to the transducer and place the transducer 10 cm lateral to the umbilicus. Adjust until the lateral abdominal wall is visible on the screen21 (Figure 3).
- Ensure that the transducer is tightly secured to the lateral abdominal wall.
- Secure the belt with the velcro straps. Adjust the depth to obtain optimal image quality in B-Mode (Figure 4).

Figure 2: Transducer placed through the elastic belt and foam block. Please click here to view a larger version of this figure.
{kind=link}

Figure 3: Example of resting image to verify the lateral abdominal wall. Please click here to view a larger version of this figure.
{kind=link}

Figure 4: Transducer secured on the lateral abdominal wall by the elastic belt and foam block. Please click here to view a larger version of this figure.
{kind=link}
4. Ultrasound static side plank
- On a yoga mat (see Table of Materials), instruct the participant to lay on their right side with their elbow in 90 degrees of flexion, so their trunk and upper extremity are raised off the ground. The participant's feet should be stacked on each other with the knees fully extended. The legs should be parallel touching the yoga mat.
- Press Freeze then Store for each image to capture three static ultrasound images of the lateral abdominal wall.
NOTE: Saved images will be located below the active image screen.
5. sEMG static side plank
NOTE: Simultaneously, the researcher will also obtain the sEMG output during the static positioning described in step 4.1.
- In the sEMG menu in the top left screen of the EMG recording application, select Settings, which is a gear icon.
- Once in the sensor settings page, select the bicep icon. This will open the page for normalization measurements.
- Press Click Play to Begin; there will be a 5 s countdown. During this period, instruct the patient to assume the testing position. The recording will take an additional 5 s.
- Record the "MVC = .XXXXmV", as this will be used for normalization calculation.
NOTE: The EMG mobile suite automatically band pass filters between 20 -450 Hz. EMG (RMS) 333.3, 1125 ms window width.
6. Side plank
- Next, instruct the participant to complete the side plank for 60 s maintaining the correct form22. Press the M on the ultrasound machine to turn on M-mode.
- Press Plot, press the red button and press the Save button again in the EMG application. The participant will be given a 3 s countdown. Once that countdown commences, press Store on the ultrasound to begin the ultrasound recording.
NOTE: The participant will hold the correct form until 60 s, or when the researcher determines that the correct form has been disrupted. - To save the recorded M-mode video, press Store once the exercise has stopped and the Stop button on the sEMG application.
- Click Save file as and type in a filename to save the output, which will appear on the screen when the recording is stopped.
7. Ultrasound static dead bug
- On the yoga mat, instruct the participant to lay supine with their legs in a hook-lying position.
- Press B to enter brightness mode. Press Freeze and then Store for each image to capture three static images of the lateral abdominal wall via ultrasound. Saved images will be located below the active image screen.
8. sEMG static dead bug
- In the menu of the EMG application (top left), select Settings, which is a gear icon.
- Once in the sensor settings page, select the bicep icon. This will open the page for normalization measurements.
- Press Click Play to Begin. During the 5 s countdown, instruct the patient to assume the testing position. The recording will take an additional 5 s.
- Record the "MVC = .XXXXmV", as this will be used for normalization calculation.
9. Dead bug
- Next, instruct the participant to complete the dead bug for 60 s, maintaining the correct form. Press the M on the ultrasound machine to turn on M-mode.
- Instruct the participant to maximally extend their right shoulder while maximally extending their left hip and knee, while also maintaining the starting position of the contralateral extremities.
- Instruct the participant to then flex their shoulder, hip, and knee to return to the starting position. The contralateral extremities will then perform the same motion.
- Ask the participant to perform the exercise to a metronome set to 45 beats per min. This results in 22 repetitions of the dead bug in 60 s.
NOTE: The participant should hold the correct form until 60 s, or until the researcher determines that the correct form has been disrupted or the metronome rhythm has been interrupted. - Press Plot, press the red button and then press Play. Press the Save button again in the EMG application. The participant will be given a 3 s countdown. Once that countdown commences, press Store on the ultrasound to begin the ultrasound recording.
10. Ultrasound static measurement
- Click Enter when the first static image you want to measure is selected.
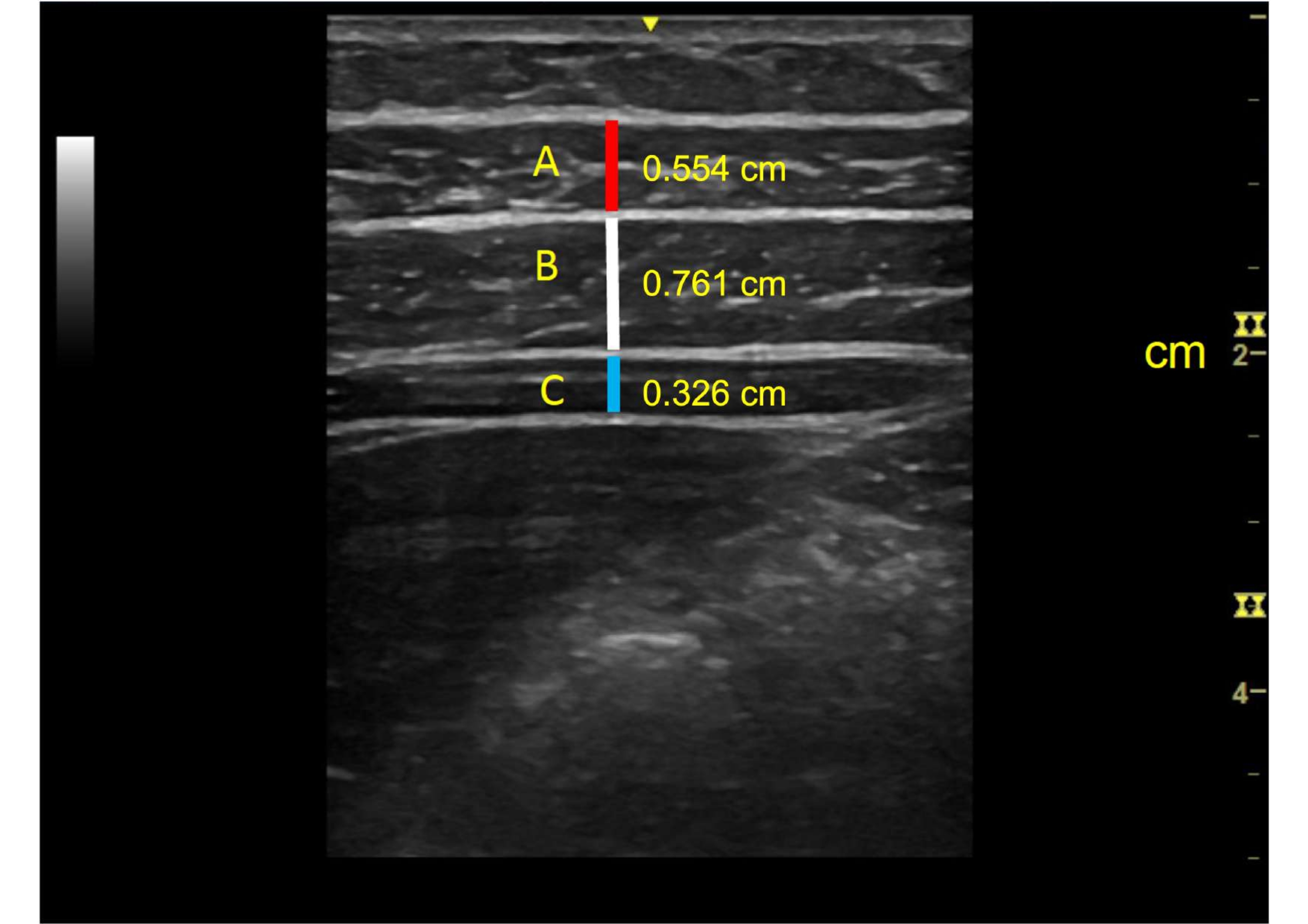
- Press Measure to open the measurement tool. Measure the maximal muscle thickness during the static positions in centimeters from the superior inferior fascial border to the inferior superior fascial border (Figure 5 [side plank] and Figure 6 [dead bug]).
- Click Enter at the superior inferior border and Enter again at the inferior superior border.
- Repeat steps 10.1-10.3 for side plank and dead bug static measurements. Average the measurements of the three static images.

Figure 5: Example of lateral abdominal wall during the side plank static, exercise starting position and measurements of muscles. A = external oblique (0.554 cm), B = internal oblique (0.761 cm), and C = transverse abdominis (0.326 cm). Please click here to view a larger version of this figure.
{kind=link}

Figure 6: Example of lateral abdominal wall in the dead bug static, exercise starting position and measurements of muscles. A = external oblique (0.618 cm), B = internal oblique (0.820 cm), and C = transverse abdominis (0.438 cm). Please click here to view a larger version of this figure.
{kind=link}
11. Ultrasound dynamic measurements
- Measure the maximal thickness of the external oblique, internal oblique, and transverse abdominis thickness during the first 5 s and last 5 s of the exercise. Additionally, record the maximal thickness over the entire 60 s.
NOTE: The side plank is commonly performed for durations of 5 s. Taking sets and repetition guidelines from previous authors, a longer duration of 60 s was chosen for comparison in this protocol. The first 5 s and last 5 s of the task were compared to evaluate both the strength and endurance aspects of the muscle group23,24. - Using the Scroll button, find the first 5 s and last 5 s of each exercise. Additionally, visually inspect for the greatest thickness of each muscle throughout the 60 s exercise.
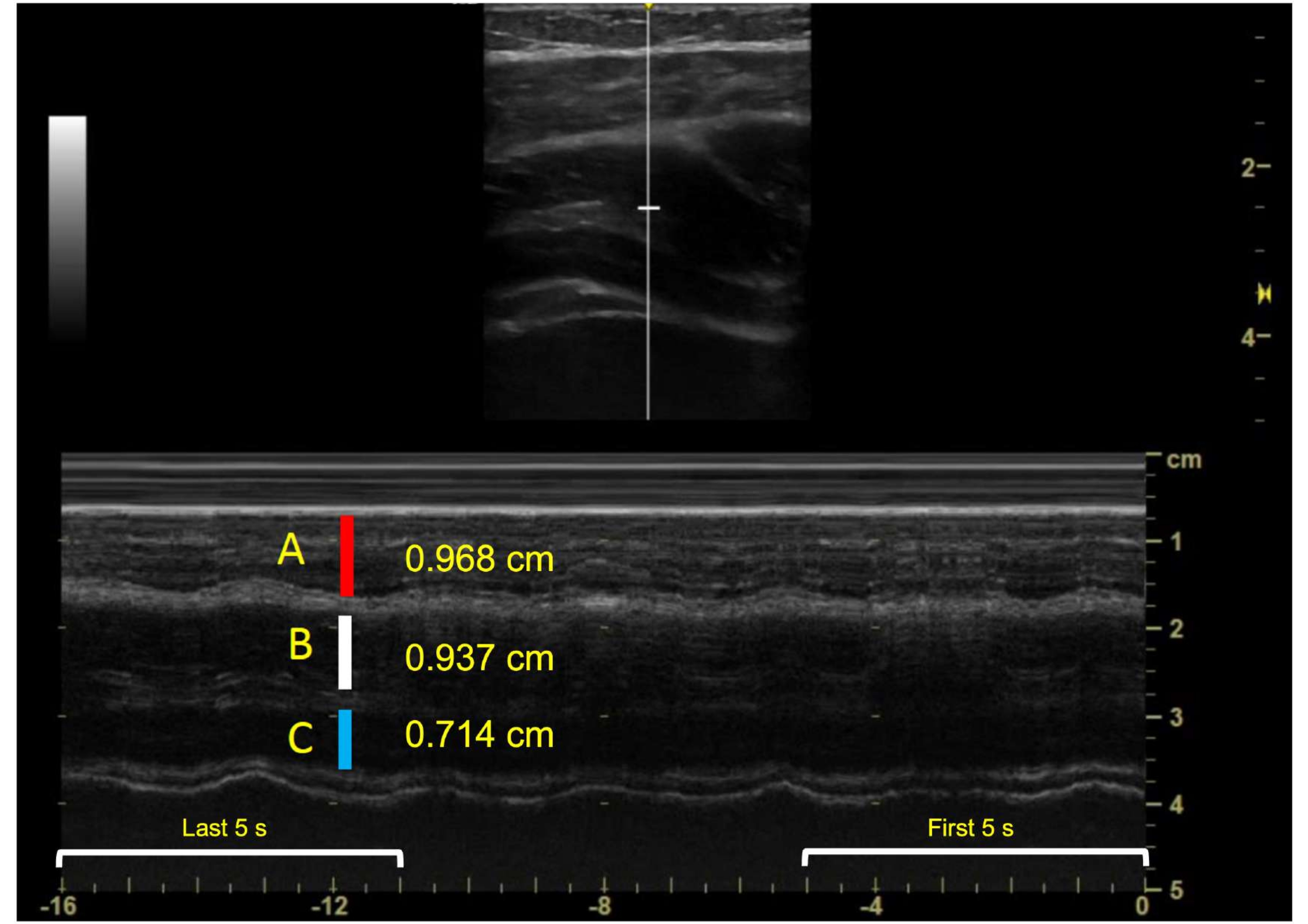
- Press Measure to open the measurement tool. Measure the maximal muscle thickness during the static positions in centimeters from the superior inferior fascial border to the inferior superior fascial border (Figure 7 [side plank] and Figure 8 [dead bug]).
- Divide each of the three thickness measurements obtained during the exercises by the averaged static position to obtain an activation ratio 25.

Figure 7: Example of lateral abdominal wall during the side plank exercise and measurements of muscles in M-mode. A = external oblique (0.968 cm), B = internal oblique (0.937 cm), and C = transverse abdominis (0.714 cm). Please click here to view a larger version of this figure.
{kind=link}

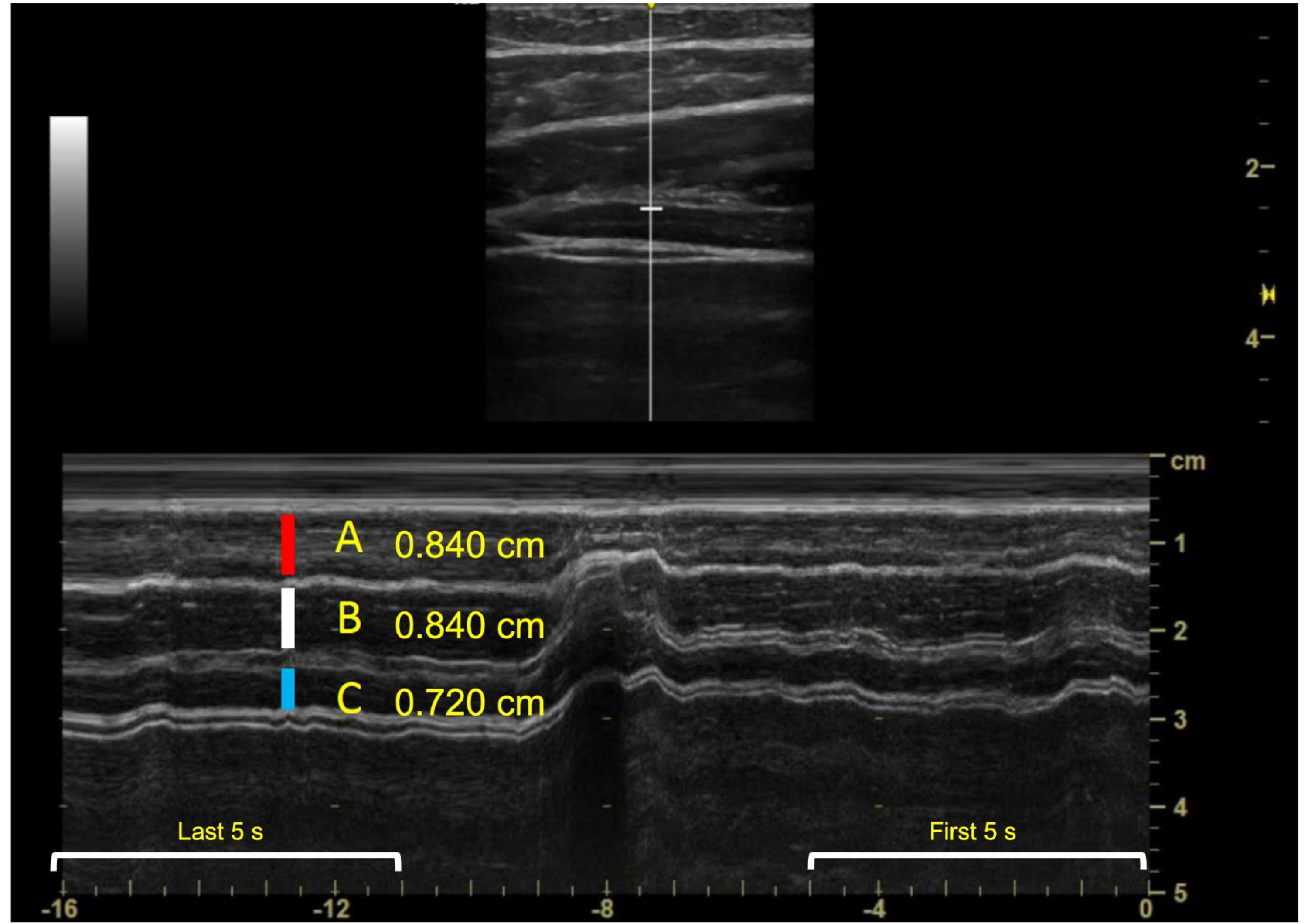
Figure 8: Example of lateral abdominal wall during the dead bug exercise and measurements of muscles in M-mode. A = external oblique (0.840 cm), B = internal oblique (0.840 cm), and C = transverse abdominis (0.720 cm). Please click here to view a larger version of this figure.
{kind=link}
12. sEMG Measurement
- Press the Home icon on the EMG data recording page. Select the folder icon in the top right corner of the screen. The saved output from the static and exercise trials will be saved here. Convert each file to an .xlsx file. Export the .xlsx file.
- In a spreadsheet, obtain the maximum values during the first and last 5 s, and the overall maximum value.
- Divide the static sEMG output obtained in steps 5 (static side plank sEMG) and 8 (dead bug sEMG) by the output during the exercises, respectively.
Wyniki
The measurements of both ultrasound and sEMG during the static, exercise starting position are represented in Table 2. These numbers will be used as the denominator when calculating the activation ratio. The thickness values of external oblique, internal oblique, and transverse abdominis during the first 5 s, last 5 s, and total duration (60 s) are in Table 3. These numbers are divided by the numbers in Table 2. The sEMG values normalized to static, exercise starting pos...
Dyskusje
M-mode ultrasound provides onset of muscle tissue movement and muscle thickness change during real time observation of anatomy over a selected time21. M-mode ultrasound combined with sEMG provides an overall understanding of muscle function, including electrical representation and visual observation. These instruments can be used in tandem during exercise to provide researchers with a global understanding of muscle function.
Specific training of ultrasound and sEMG tech...
Ujawnienia
The authors declare no conflicts of interest related to this manuscript.
Podziękowania
None.
Materiały
| Name | Company | Catalog Number | Comments |
| Alcohol prep pads | Henry Schein | HS1007 | |
| Amazon Basics 1/2- Inch Extra Thick Exercise Yoga Mat | Amazon | YM2001BK | |
| Delsys Trigno Sensor Adhesive Interface, 4-Slot | Delsys | SC:F03 | |
| Delsys Trigno Wireless System | Delsys | T03-A16014 | |
| Galaxy Tablet S5e | Samsung | SM-TS20N | |
| GE NextGen Logig e Ultrasound Unit | GE Healthcare | HR48382AR | |
| Linear Array Probe | GE Healthcare | H48062AB | |
| Trigno Avanti sensors | Delsys | T03-A16014 |
Odniesienia
- Kendall, F., McCreary, E., Provance, P., Rodgers, M., Romani, W. . Muscles: Testing and Function with Posture and Pain. , (2005).
- Bergmark, A. Stability of the lumbar spine. A study in mechanical engineering. Acta Orthopaedica Scandinavica. Supplementum. 230, 1-54 (1989).
- Borghuis, J., Hof, A. L., Lemmink, K. A. P. M. The importance of sensory-motor control in providing core stability. Sports Medicine. 38 (11), 893-916 (2008).
- Ireland, M. L., Willson, J. D., Ballantyne, B. T., Davis, I. M. Hip strength in females with and without patellofemoral pain. Journal of Orthopaedic & Sports Physical Therapy. 33 (11), 671-676 (2003).
- Zazulak, B. T., Hewett, T. E., Reeves, N. P., Goldberg, B., Cholewicki, J. Deficits in neuromuscular control of the trunk predict knee injury risk: prospective biomechanical-epidemiologic study. The American Journal of Sports Medicine. 35 (7), 1123-1130 (2007).
- George, S. Z., et al. Interventions for the management of acute and chronic low back pain: revision 2021. Journal of Orthopaedic & Sports Physical Therapy. 51 (11), (2021).
- Dieterich, A. V., et al. M-mode ultrasound used to detect the onset of deep muscle activity. Journal of Electromyography and Kinesiology. 25 (2), 224-231 (2015).
- Teyhen, D. S., et al. Abdominal and lumbar multifidus muscle size and symmetry at rest and during contracted states normative reference ranges. Journal of Ultrasound in Medicine. 31 (7), 1099-1110 (2012).
- Oliva-Lozano, J. M., Muyor, J. M. Core muscle activity during physical fitness exercises: A systematic review. International Journal of Environmental Research and Public Health. 17 (12), 4306 (2020).
- Dieterich, A., Petzke, F., Pickard, C., Davey, P., Falla, D. Differentiation of gluteus medius and minimus activity in weight bearing and non-weight bearing exercises by M-mode ultrasound imaging. Manual therapy. 20 (5), 715-722 (2015).
- Biscarini, A., Contemori, S., Grolla, G. Activation of scapular and lumbopelvic muscles during core exercises executed on a whole-body wobble board. Journal of Sport Rehabilitation. 28 (6), 623-634 (2019).
- Calatayud, J., et al. Progression of core stability exercises based on the extent of muscle activity. American Journal of Physical Medicine & Rehabilitation. 96 (10), 694-699 (2017).
- McGill, S. M., Karpowicz, A. Exercises for spine stabilization: motion/motor patterns, stability progressions, and clinical technique. Archives of Physical Medicine and Rehabilitation. 90 (1), 118-126 (2009).
- Czaprowski, D., et al. Abdominal muscle EMG-activity during bridge exercises on stable and unstable surfaces. Physical Therapy in Sport. 15 (3), 162-168 (2014).
- Souza, G. M., Baker, L. L., Powers, C. M. Electromyographic activity of selected trunk muscles during dynamic spine stabilization exercises. Archives of Physical Medicine and Rehabilitation. 82 (11), 1551-1557 (2001).
- Criswell, E. . Cram's Introduction to Surface Electromyography. , (2010).
- Mirmohammad, R., Minoonejhad, H., Sheikhhoseini, R. Ultrasonographic comparison of deep lumbopelvic muscles activity in plank movements on stable and unstable surface. Physical Treatments: Specific Physical Therapy Journal. 9 (3), 147-152 (2019).
- Bunce, S. M., Hough, A. D., Moore, A. P. Measurement of abdominal muscle thickness using M-mode ultrasound imaging during functional activities. Manual Therapy. 9 (1), 41-44 (2004).
- Garber, C. E., et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Medicine & Science in Sports & Exercise. 43 (7), 1334-1359 (2011).
- Vera-Garcia, F. J., Moreside, J. M., McGill, S. M. MVC techniques to normalize trunk muscle EMG in healthy women. Journal of Electromyography and Kinesiology. 20 (1), 10-16 (2010).
- Partner, S. L., et al. Changes in muscle thickness after exercise and biofeedback in people with low back pain. Journal of Sport Rehabilitation. 23 (4), 307-318 (2014).
- Devorski, L., Bazett-Jones, D., Mangum, L. C., Glaviano, N. R. Muscle activation in the shoulder girdle and lumbopelvic-hip complex during common therapeutic exercises. Journal of Sport Rehabilitation. 31 (1), 31-37 (2021).
- Youdas, J. W., et al. Magnitudes of muscle activation of spine stabilizers in healthy adults during prone on elbow planking exercises with and without a fitness ball. Physiotherapy Theory and Practice. 34 (3), 212-222 (2018).
- Ekstrom, R. A., Donatelli, R. A., Carp, K. C. Electromyographic analysis of core trunk, hip, and thigh muscles during 9 rehabilitation exercises. The Journal of Orthopaedic and Sports Physical Therapy. 37 (12), 754-762 (2007).
- Mangum, L. C., Sutherlin, M. A., Saliba, S. A., Hart, J. M. Reliability of ultrasound imaging measures of transverse abdominis and lumbar multifidus in various positions. PM&R. 8 (4), 340-347 (2016).
- Mangum, L. C., Henderson, K., Murray, K. P., Saliba, S. A. Ultrasound assessment of the transverse abdominis during functional movement. Journal of Ultrasound in Medicine. 37 (5), 1225-1231 (2018).
- Carovac, A., Smajlovic, F., Junuzovic, D. Application of ultrasound in medicine. Acta Informatica Medica. 19 (3), 168-171 (2011).
- Chowdhury, R. H., et al. Surface electromyography signal processing and classification techniques. Sensors. 13 (9), 12431-12466 (2013).
- Tweedell, A. J., Tenan, M. S., Haynes, C. A. Differences in muscle contraction onset as determined by ultrasound and electromyography. Muscle & Nerve. 59 (4), 494-500 (2019).
Przedruki i uprawnienia
Zapytaj o uprawnienia na użycie tekstu lub obrazów z tego artykułu JoVE
Zapytaj o uprawnieniaThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. Wszelkie prawa zastrzeżone