
Method Article
An Electrophysiological Technique to Accurately Diagnose and Treat Erectile Dysfunction
In This Article
Summary
Here we describe an appropriate electrophysiological technique to diagnose and treat patients with erectile dysfunction.
Abstract
Erectile dysfunction (ED) is a common disease in males. In the past, the first-line treatment of ED was mainly noninvasive-psychotherapy and oral phosphodiesterase 5 (PDE5) inhibitors. Oral PDE5 inhibitors often need to be used before sexual intercourse and do not repair the pathological damage; hence, the therapeutic effect for secondary ED caused by neurological or endocrine disorders is poor. Second-line treatments mainly include penile corpus cavernosum injection of alprostadil, transurethral administration, vacuum negative pressure devices, and other methods, with obvious side effects such as local pain.
The third-line treatment mainly refers to penile prosthesis implantation. Indications of this treatment are strict, complications such as mechanical failure and infection may occur after operation, and it is expensive. Other treatments such as stem cell therapy and gene therapy are still in the experimental research stage and have not been used in clinics. A new treatment based on an electrophysiological technique combines a medical infrared thermal imager with low-frequency (20-50 Hz) neuromuscular electrical stimulation, which has achieved good results in the prevention and treatment of female pelvic floor dysfunction.
Male generative organs are located in the pelvic floor area, and their normal function not only depends on the integrity of the structure and function of the male generative organs, but is also closely related to the blood vessels, nerves, muscles, and other pelvic floor organs. Therefore, this electrophysiological technique was applied to male ED, focusing on the observation of the penis, groin, and hypogastrium for accurate diagnosis and treatment. This demonstrated effective improvement in the conscious erectile status and erectile function scores of patients suffering from ED.
Introduction
Erectile dysfunction (ED) refers to the male inability to achieve and/or maintain a satisfactory erection during sexual behavior1. The common etiologies of ED are psychological, neurotic, anatomical, vascular, and drug-induced. Worldwide, the prevalence of ED in men is high and increases with age2. ED can affect a patient's self-confidence, quality of life, and the stability of family relations. In addition, research shows that ED increases the risk of cardiovascular disease in patients in the future3. Therefore, once ED is diagnosed, it should be treated as soon as possible. At present, the main therapies for ED are oral PDE5 inhibitors and surgeries. Studies show that PDE5 inhibitors are ineffective in up to 35% of patients suffering from ED4, resulting in a discontinuation rate between 35% and 45%5. The reasons for the discontinuation of PDE5 inhibitors include concerns about possible side effects and high drug costs6. Additionally, surgical treatment could cause complications such as infection and pain. However, electrophysiological technology can be used to analyze the temperature of patients in different positions under different movements by using medical infrared thermal imaging visual thermography to identify the abnormal parts of the human body, and then patients can be treated with low-frequency (20-50 Hz) neuromuscular electrical stimulation.
The low-frequency nerve and muscle electrical stimulator is a continuous activation instrument with simple and effective operation and a wide range of indications, which has been widely used in obstetrics and gynecology7, cardiovascular diseases8, and perioperative rapid rehabilitation9. In particular, it has achieved good results in the prevention and treatment of female pelvic floor dysfunction diseases and female pelvic floor discipline construction10. It is noteworthy that this electrophysiological technology has not yet been applied in andrology. The medical infrared thermal imager can produce infrared wave images emitted by humans. As a part of the temperature regulation process, the intensity can be changed according to the health status of the patients11, and the physiological and pathological reactions of diseases can be studied from the cell metabolism and human functional changes to provide a specific auxiliary diagnostic method for clinical research. There are temperature differences between individuals due to the differences in human anatomy, tissue metabolism, blood circulation, nerve function, and blood states.
Moreover, different images can be formed by medical infrared thermal image scanning. Comparisons of the similarities and differences between the images of the normal state of the body and abnormal states can help diagnose the nature and degree of the disease in combination with clinical diagnosis. These comparisons can also help accomplish accurate diagnoses of related diseases under the infrared visible state by combining these data with the low-frequency (20-50 Hz) neuromuscular therapy instrument. Accurate electrophysiological diagnosis and treatment parameters, including treatment sites, blood vessels, muscles, and nerves, are determined using computer software supporting the low-frequency neuromuscular therapy instrument, and individualized treatment plans are formulated to achieve immediate and precise treatment. Moreover, related parameters can be seen simultaneously, and it is convenient for the observation and evaluation of the curative effect.
Male pelvic floor muscles can promote erection and ejaculation12. By monitoring intracavernous pressure, spontaneous contraction and electrical stimulation increase muscle strength in the sciatic cavernous body13. Although patients suffering from ED have potential pelvic floor muscle dysfunction, the treatment of ED is still based on drug treatment and lifestyle improvement. In this study, electrophysiological technology, including medical infrared thermal imaging and low-frequency neuromuscular electrical stimulation, provides a new method for the treatment of ED patients through the diagnosis and treatment of nerves, muscles, and blood vessels in abnormal parts of patients suffering from ED.
Protocol
All the procedures in the following protocol were reviewed and approved by the Institutional Review Board of The Northern Jiangsu People's Hospital for application on November 11, 2020. In this study, the process is explained to the patients in detail and the patients' consent is obtained before using electrophysiological technology for diagnosis and treatment.
1. Patient selection
- Set the following inclusion criteria:
- Select patients who score <22 points on the International Erectile Function Questionnaire-5 (IIEF-5).
- Ensure that the selected patients are generally in good health, married or have a fixed sexual partner, and can maintain normal sexual intercourse at least once a week from the beginning to the end of the study.
- Ensure that patients do not and have not taken any drugs to improve erectile function in the first 4 weeks.
- Select patients whose reproductive hormone examination results are normal.
- Select patients who voluntarily agree to participate in this study and give their signed, informed consent.
- Set the following exclusion criteria:
- Exclude patients suffering from ED caused by hormones, nerves, or psychological factors.
- Exclude patients with organic abnormalities in the penis (abnormal development of genitalia or abnormal palpation of the bilateral testis, epididymis, or spermatic cord).
- Exclude patients with severe cardiovascular and cerebrovascular diseases who cannot have normal sex lives.
- Exclude patients with a pacemaker implantation.
- Exclude patients with poor blood pressure control (systolic blood pressure ≥160 mmHg and diastolic blood pressure ≥100 mmHg after treatment) and patients with poor glycemic control whose fasting plasma glucose is >7.0 mmol or 126 mg/dL after treatment.
- Exclude patients with drug, alcohol, or other substance abuse history in the past 6 months.
- Exclude patients with radical prostatectomy or pelvic surgery and those who have participated in any other medical device or drug clinical research studies in the past 3 months.
2. Diagnosis and treatment process
- Preparation before inspection
- Maintain the ambient temperature of the infrared thermal imaging inspection chamber at 24 ± 2 °C and ambient humidity at 40% to 60%.
- Prohibit the examinee from drinking alcohol, taking vasodilator and vasoconstrictor drugs, and eating food at temperatures over 40 °C (or any spicy food), 24 h before examination.
- Fully expose the test area during the examination, removing bandages 2 h before the examination.
- Prohibit the examinee from being exposed to high temperature, a strong cold environment, or being directly in the airflow from an air conditioner or fan 1 h before inspection. Loosen the pants belt, and remove watches, necklaces, and other items 15 min in advance.
- Let the examinee stand or sit quietly in the waiting area for 10 min.
- Locate the outliers.
- Let the patient enter the medical infrared camera inspection chamber, take off all their clothes, and face the scanning head.
- Click the motion capture bar button after posing, click freeze, and save each action (Figure 1).
- Analyze the temperatures of different positions of patients under different movements, especially the penis, groin, and lower abdomen.
- Consider the penis position to be abnormal if the penis temperature is lower than 33.5 °C or higher than 34.5 °C (see Figure 2).
- Consider the groin position to be abnormal if the groin temperature is lower than 33.5 °C or higher than 34.5 °C (see Figure 2).
- Consider the lower abdomen position to be abnormal if the lower abdomen temperature is lower than 33 °C or higher than 34 °C (see Figure 2).
- Analyze and determine the diagnosis and treatment plan.
- Analyze the treatment plan of the abnormal points on the computer equipment of the low-frequency neuromuscular therapy instrument and download it to the diagnosis equipment of the low-frequency neuromuscular therapy instrument after detecting the abnormal point.
- Determine the abnormal points where the temperature anomaly was detected before, affix the electrodes one by one to the corresponding sites on the patient, and connect them to the computer equipment of the low-frequency (20-50 Hz) neuromuscular therapy instrument, as shown in Figure 3, Figure 4, and Figure 5.
- Observe the real-time temperature change of each program acting on the abnormal point under infrared thermal imaging.
- Select the fastest program that can be seen on the infrared imager for the temperature of the abnormal part to return to normal and determine the corresponding frequency and pulse width on the equipment of the low-frequency neuromuscular therapy instrument.
- Precision electrophysiological therapy
- Find the corresponding plan on the Bluetooth equipment of the low-frequency neuromuscular therapy instrument.
- Use the Bluetooth equipment of the low-frequency neuromuscular therapy instrument to connect the patient's own mobile phone for treatment. Select a value at which the patient feels comfortable within the allowable frequency (20-50 Hz) and pulse width (0.02-0.3 ms) range once a day, for 12 stimulations as a course, and evaluate the effect after a course of treatment.
Results
The electrophysiological technique was performed on 48 patients from August to December 2021. Among them, 46 cases had penile temperature disorder with a temperature of 30.2 ± 1.2 °C, 35 cases had groin temperature disorder with a temperature of 30.6 ± 1.3 °C, and 18 cases had abdominal temperature disorder with a temperature of 30.1 ± 1.2 °C. After one course of treatment, the temperature of the treatment site increased in all patients. The temperature of the penis was 31.0 ± 1.0 °C, the temperature of the groin was 31.5 ± 1.1 °C, and the temperature of the lower abdomen was 31.2 ± 1.1 °C. The IIEF-5 score before treatment was 13.8 ± 3.6, and the IIEF-5 score after one course of treatment was 16.6 ± 4.2. The temperature and IIEF-5 score of the patient's treatment site were both increased after treatment (p < 0.05); the Erectile Hardness Scale (EHS) score, which showed a skewed distribution, was 2.43 (2, 3) versus 2.96 (2, 3.75). These differences were significant (p < 0.05) (Table 1).
The effect of this electrophysiological technique was analyzed via Audiovisual Sexual Stimulation (AVSS) examinations before and after therapy, as shown in Table 2. Before and after therapy, the erection time of the patients significantly increased from 6.14 (0.44, 11.5) min to 8.67 (4.13, 14.25) min (p < 0.01). The average hardness of the tip of the penis significantly increased from 18.92% (1.50%, 30.00%) to 24.33% (15.00%, 34.00%) (p < 0.01), as did the average hardness of the root of the penis, from 26.33% (5.75%, 39.50%) to 30.10% (26.00%, 41.50%) (p < 0.01). The circumference of the tip of the penis significantly increased from 1.30 (0, 2.15) cm to 1.67 (1.20, 2.20) cm (p < 0.05), whereas the circumference of the penis root increased from 1.70 (0.23, 2.58) cm to 1.79 (1.40, 2.6) cm (p > 0.05).
In an example, a 32-year-old male came to the hospital for medical treatment after experiencing weak erection and unsatisfactory sexual experience for 1 month. The patient met the inclusion criteria and volunteered to participate in this trial. Before the treatment, the IIEF-5 score of the patient was 17, and the erectile hardness monitor indicated poor hardness. The patient entered the medical infrared camera inspection chamber, followed the instructions as shown in Figure 1, and the infrared thermal imager analyzed the temperature of the patient's penis, groin, and lower abdomen with different movements. The infrared thermal imager indicated that the penis temperature was 32.7 °C, the groin temperature was 33.7 °C, and the lower abdomen temperature was 32.5 °C.
According to the examination, the patient's penis and lower abdomen were identified as the anomalous sites. Therefore, we affixed the electrodes to the corresponding sites on the patient and connected them to the computer equipment of the low-frequency neuromuscular therapy instrument as shown in Figure 3 and Figure 5. We observed the temperature change of each program acting on the abnormal points under infrared thermal imaging for 60 s, selected the fastest program for the temperature of the abnormal site to return to normal, and determined the corresponding frequency and pulse width on the low-frequency neuromuscular therapy instrument. The treatment plan for the patient was "30 Hz, 500 US" to stimulate the patient's penis and lower abdomen for 30 min in turn once a day, for a total of 12 stimulations as a course. After a course of treatment, the patient had satisfactory intercourse, with an IIEF-5 score of 21 and erectile hardness monitor indicating suitable hardness. The infrared thermal imager showed a penis temperature of 34.3 °C and a lower abdomen temperature of 33.1 °C.

Figure 1: Actions to be followed by the patients. (A) Put the hands up against the ears and put the palms forward with fingers open. (B) Place the hands on the back of the head and lean back to reveal the neck. (C) Put the hands on the back of the head and turn 45° to the left. (D) Place the hands on the back of the head and turn 45° to the right. (E) Spread the legs slightly with drooping hands and put the palms forward with fingers open, facing the scanning head. (F) Keeping the hands down, put the palms forward with fingers open and face away from the scanning head. Please click here to view a larger version of this figure.
{kind=link}

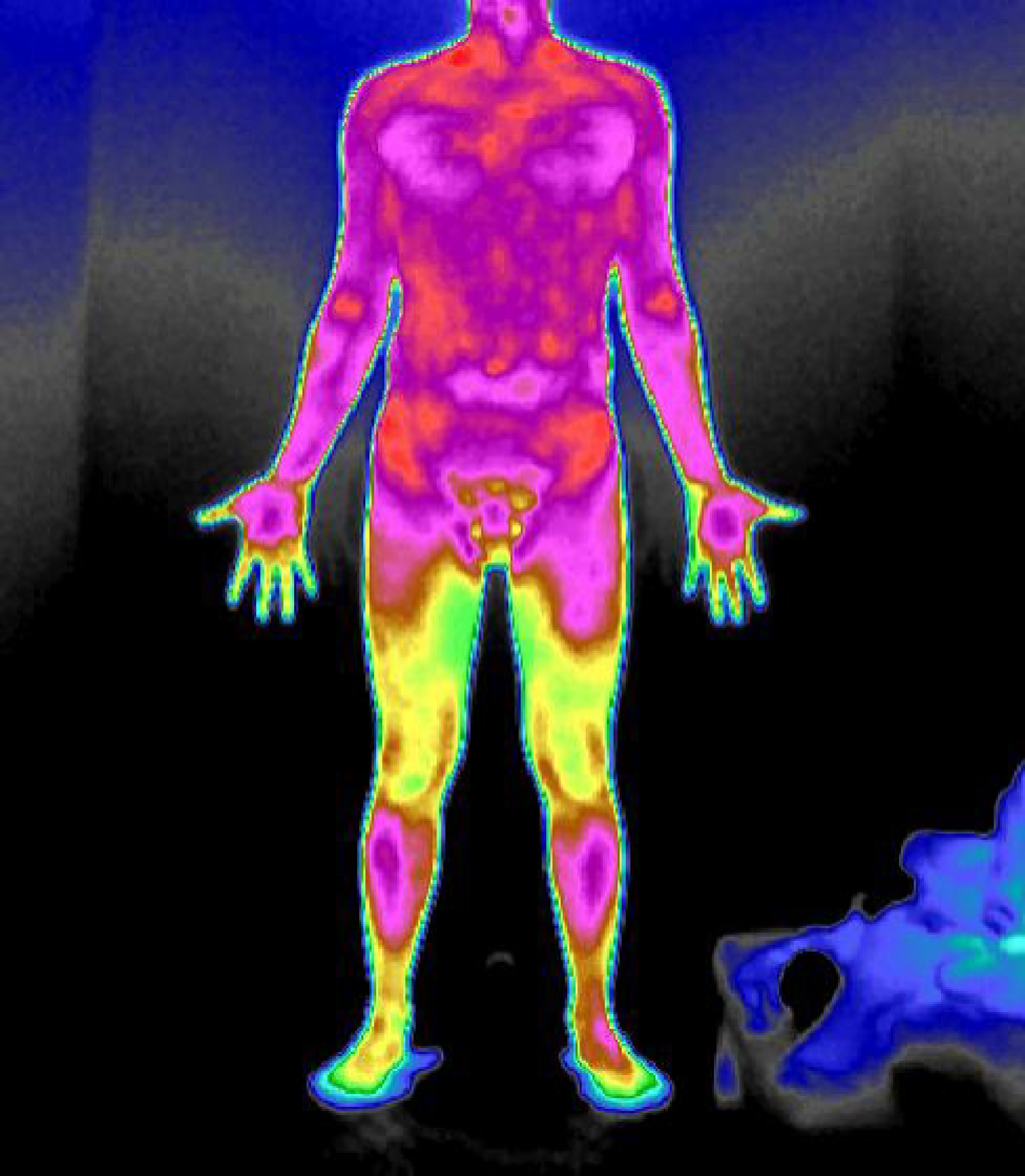
Figure 2: Normal infrared thermal imaging. Please click here to view a larger version of this figure.
{kind=link}

Figure 3: Placement of electrode pads for abnormal penile temperature. Please click here to view a larger version of this figure.
{kind=link}

Figure 4: Placement of electrode pads for abnormal groin temperature. Please click here to view a larger version of this figure.
{kind=link}

Figure 5: Placement of electrode pads for abnormal abdominal temperature. Please click here to view a larger version of this figure.
{kind=link}
| before therapy | after treatment | N | P | |
| temperature of penis (°C) | 30.2 ± 1.2 | 31.0 ± 1.0 | 46 | <0.05 |
| temperature of groin (°C) | 30.6 ± 1.3 | 31.5 ± 1.1 | 35 | <0.05 |
| temperature of lower abdomen (°C) | 30.1 ± 1.2 | 31.2 ± 1.1 | 18 | <0.05 |
| IIEF-5 | 13.8 ± 3.6 | 16.6 ± 4.2 | 48 | <0.05 |
| EHS | 2.43 (2, 3) | 2.96 (2, 3.75) | 48 | 0.02 |
Table 1: The effect of the electrophysiological technique on the temperature, IIEF-5, and EHS of the treatment site. Abbreviations: IIEF-5 = International Erectile Function Questionnaire-5; EHS = Erectile Hardness Scale.
| before therapy | after treatment | N | P | |
| erection time (min) | 6.14 (0.44, 11.5) | 8.67 (4.13, 14.25) | 48 | <0.05 |
| the average hardness of the tip (%) | 18.92 (1.50, 30.00) | 24.33 (15.00, 34.00) | 48 | 0.001 |
| the average hardness of the root (%) | 26.33 (5.75, 39.50) | 30.10 (26.00, 41.50) | 48 | <0.05 |
| the circumference of tip (cm) | 1.30 (0, 2.15) | 1.67 (1.20, 2.20) | 48 | 0.018 |
| the circumference of root (cm) | 1.70 (0.23, 2.58) | 1.79 (1.40, 2.6) | 48 | 0.272 |
Table 2: The effect of the electrophysiological technique on the results of the AVSS examination in ED patients. Abbreviations: AVSS = AudioVisual Sexual Stimulation; ED = erectile dysfunction.
Discussion
During sex, penile erection is largely dependent upon sufficient blood flow into the corpus cavernosum, which requires the coordination of arterial endothelium-dependent vasodilation and sinus endothelium-dependent cavernous smooth muscle relaxation14. Nitric oxide (NO) is the primary neurotransmitter of the peripheral erectile-promoting nerves, released by parasympathetic autonomic nerves and sinus endothelium to produce cyclic guanosine monophosphate (cGMP). This cGMP relaxes the cavernous smooth muscle, resulting in increased pressure in the cavernous body to achieve erection15. By monitoring the formation of NO and cGMP, it was confirmed that electrical stimulation could lead to the formation of NO and cGMP in the penile cavernous smooth muscle16.
From the perspective of anatomical structure, male reproductive organs are located in the pelvic floor-related areas, and their normal function depends not only on their structural and functional integrity but also on the blood vessels, nerves, muscles, and other organs associated with the pelvic floor. Studies have shown that contraction of the superficial pelvic floor musculature can increase intracavernous pressure by restricting venous return to the base of the penis to produce an erection17. In addition, neural, endocrine, immune regulatory networks, and psychophysiological factors also play important roles. Problems in any one or more of the above areas will promote the occurrence and development of male diseases. Previous studies have shown that male pelvic floor muscle training, including electrical stimulation, can improve stress urinary incontinence, overactive bladder, ED, premature ejaculation, lower urinary tract syndrome, and muscle-related pelvic pain12. Further, physical exercise therapy and electrical stimulation can effectively treat premature ejaculation with an effective rate of 64%18.
Although functional electrical stimulation therapy is widely used in sexual dysfunction19, there are few studies on the treatment of ED. There are many advantages of the described electrophysiological technique; it is suitable for a variety of diseases caused by nerve and muscle damage, including pelvic floor dysfunction diseases, motor system injury diseases, nervous system diseases, digestive system diseases, and endocrine diseases. Additionally, it has no side effects, is easy for patients to accept, and has been used in clinical practice for many years because of its stable, safe, and reliable features.
This study draws lessons from this electrophysiological technique that has achieved good results in the prevention and treatment of female pelvic floor dysfunction. Medical thermal imaging is used to detect, before low-frequency neuromuscular electrical stimulation is used to accurately treat, abnormal sites through blood vessels, muscles, and nerves.
We use a medical thermal imager to find the abnormal parts and then treat them with low-frequency neuromuscular current stimulated by blood vessels, muscles, and nerves, which provides a new method for the diagnosis and treatment of patients suffering from ED. However, due to the short duration of this study and the small number of samples, we will continue to increase the number of cases to observe the recovery of patients suffering from ED treated with this electrophysiological technique. In addition, compared with the current ED treatment methods, this method has the disadvantages of a slow effect and long therapeutic time.
Disclosures
The authors have no conflicts of interest to disclose.
Acknowledgements
This research was supported by a grant from the National Health Commission Science and Technology Plan Project, funded by the Medical and Health Science and Technology Development Research Center of the National Health Commission (grant number: HDSL202001051).
Materials
| Name | Company | Catalog Number | Comments |
| Low-frequency nerve and muscle electrical stimulator | Foshan Shanshan Datang Medical Technology Company | 20182260716 | |
| RigiScan Plus Monitor | GOTOP Medical | 20162211942 |
References
- NIH consensus conference. NIH consensus development panel on impotence. JAMA. 270 (1), 83-90 (1993).
- Eardley, I. The incidence, prevalence, and natural history of erectile dysfunction. Sexual Medicine Reviews. 1 (1), 3-16 (2013).
- Gandaglia, G., et al. A systematic review of the association between erectile dysfunction and cardiovascular disease. European Urology. 65 (5), 968-978 (2014).
- McMahon, C. N., Smith, C. J., Shabsigh, R. Treating erectile dysfunction when PDE5 inhibitors fail. BMJ. 332 (7541), 589-592 (2006).
- Al-Shaiji, T. F., Brock, G. B. Phosphodiesterase type 5 inhibitors for the management of erectile dysfunction: preference and adherence to treatment. Current Pharmaceutical Design. 15 (30), 3486-3495 (2009).
- Son, H., Park, K., Kim, S. W., Paick, J. S. Reasons for discontinuation of sildenafil citrate after successful restoration of erectile function. Asian Journal of Andrology. 6 (2), 117-120 (2004).
- Brown, O., et al. Vaginal electrical stimulation for postpartum neuromuscular recovery: a randomized clinical trial. Female Pelvic Medicine & Reconstructive Surgery. 27 (11), 659-666 (2021).
- Williams, K. J., Moore, H. M., Davies, A. H. Haemodynamic changes with the use of neuromuscular electrical stimulation compared to intermittent pneumatic compression. Phlebology. 30 (5), 365-372 (2015).
- Li, H., et al. Curative efficacy of low frequency electrical stimulation in preventing urinary retention after cervical cancer operation. World Journal of Surgical Oncology. 17 (1), 141 (2019).
- Reis, B. M., da Silva, J. B., Rocha, A. P. R., Liebano, R. E., Driusso, P. Intravaginal electrical stimulation associated with pelvic floor muscle training for women with stress urinary incontinence: study protocol for a randomized controlled trial with economic evaluation. Trials. 22 (1), 823 (2021).
- Diakides, N. A. Advances in medical infrared imaging. IEEE Engineering in Medicine and Biology Magazine. 21 (6), 32-33 (2002).
- Rosenbaum, T. Y. Pelvic floor involvement in male and female sexual dysfunction and the role of pelvic floor rehabilitation in treatment: a literature review. The Journal of Sexual Medicine. 4 (1), 4-13 (2007).
- Lavoisier, P., et al. Pelvic-floor muscle rehabilitation in erectile dysfunction and premature ejaculation. Physical Therapy. 94 (12), 1731-1743 (2014).
- Dean, R. C., Lue, T. F. Physiology of penile erection and pathophysiology of erectile dysfunction. The Urologic Clinics of North America. 32 (4), 379-395 (2005).
- Hurt, K. J., et al. Akt-dependent phosphorylation of endothelial nitric-oxide synthase mediates penile erection. Proceedings of the National Academy of Sciences. 99 (6), 4061-4066 (2002).
- Ignarro, L. J., et al. Nitric oxide and cyclic GMP formation upon electrical field stimulation cause relaxation of corpus cavernosum smooth muscle. Biochemical and Biophysical Research Communications. 170 (2), 843-850 (1990).
- Dorey, G. Conservative treatment of erectile dysfunction. 3: Literature review. British Journal of Nursing. 9 (13), 859-863 (2000).
- Pastore, A. L., et al. Pelvic muscle floor rehabilitation as a therapeutic option in lifelong premature ejaculation: long-term outcomes. Asian Journal of Andrology. 20 (6), 572-575 (2018).
- Balog, B. M., Deng, K., Labhasetwar, V., Jones, K. J., Damaser, M. S. Electrical stimulation for neuroregeneration in urology: a new therapeutic paradigm. Current Opinion in Urology. 29 (4), 458-465 (2019).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved