
Examen des ganglions lymphatiques
Vue d'ensemble
Source : Richard Glickman-Simon, MD, professeur adjoint, département de santé publique et médecine sociale, Tufts University School of Medicine, MA
Le système lymphatique a deux fonctions principales : de retour arrière de fluide extracellulaire à la circulation veineuse et d’exposer des substances antigéniques au système immunitaire. Comme le liquide recueilli traverse les voies lymphatiques sur son chemin du retour vers la circulation systémique, il rencontre plusieurs nœuds consistant en grappes hautement concentrés des lymphocytes. La plupart des chaînes de ganglions et nœuds résident profondément dans le corps et, par conséquent, ne sont pas accessibles à l’examen physique (Figure 1). Seuls les nœuds près de la surface peuvent être inspectés ou palpés. Les ganglions lymphatiques sont normalement invisibles, et petits noeuds sont également non palpable. Cependant, plus gros nœuds (> 1 cm) dans le cou, aisselles et les régions inguinales sont souvent comme des masses en forme de haricot, douces, lisses, mobiliers, non-appel d’offres ancrées dans le tissu sous-cutané.
Adénopathie indique généralement une infection ou, plus rarement, un cancer dans la région de drainage lymphatique. Lymphatiques peuvent devenir élargie, fixe, ferme ou tendre selon la pathologie présente. Par exemple, un ganglion doux et tendre palpable près de l’angle de la mandibule peut indiquer une amygdale infectée, alors qu’un ganglion non-tendre, ferme et élargi palpable dans l’aisselle d’une patiente peut être un signe de cancer du sein.
Régionales ganglions lymphatiques drainant la région d’une infection localisée en général restent invisibles, mais peut devenir élargies et tendre à la palpation. Une plaie infectée ou cellulite peut aussi entraîner une lymphangite ou lymphadénite, une condition où l’infection se propage le long de la chaîne des chaînes de ganglions et nœuds. Cela peut être accompagné de l’apparition de stries rouges et symptômes systémiques comme la fièvre, des frissons et malaise. Dans de rares cas, l’intensité de la réaction inflammatoire peut causer les nœuds d’adhérer aux tissus mous environnants, leur fixation en place.
Beaucoup de cancers métastatiques se propage aux ganglions lymphatiques régionaux tout d’abord. Contrairement aux infections, cellules malignes envahir les ganglions lymphatiques peuvent les amener à se sentir irrégulière et entreprise (même roche dure) mais restent non-appel d’offres. Si le cancer envahit les capsules externes, nœuds peuvent devenir attachés à des tissus mous environnants ou collés ensemble. Lymphome, un cancer primitif intrinsèque au système lymphatique, peut-être exister n’importe où dans le corps comme un ou plusieurs ganglions lymphatiques, qui peut devenir assez grand pour voir sur l’inspection et sont généralement dur et non tendre à la palpation. En plus de lymphome, adénopathie diffuse peut être une indication de généralisée troubles infectieux ou inflammatoires telles que le VIH, la mononucléose ou la sarcoïdose.
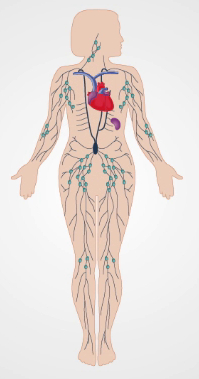
La figure 1. Le système lymphatique.
Procédure
Parce que les ganglions lymphatiques sont distribués dans tout le corps, leur évaluation a généralement lieu dans le cadre des enquêtes régionales sur la tête et cou, poitrine et aisselles, membres supérieurs, des organes génitaux externes et/ou des membres inférieurs. Il est préférable d’utiliser les touches de l’index et le médius de noter la taille, forme, nombre, souplesse, texture, mobilité et tendresse de nœuds sur le plan bilatéral.
1. les ganglions lymphatiques de la tête et du cou

La figure 2. Ganglions lymphatiques de la tête et du cou.
- Légèrement vers l’avant en position de flexion du cou du patient, une inspection à l’élargissement de nœud nettement visible.
- Pour chacune des étapes suivantes, plan de palper les lymphatiques de la tête et du cou (Figure 2) avec les deux mains, une de chaque côté. Dans de nombreux cas, les nœuds ne sont pas palpables.
- Palper les nœuds auriculaires et mastoïde pré-auriculaire, postérieurs devant l’oreille, derrière l’oreille et superficiel à l’apophyse mastoïde, respectivement.
- Palper les nœuds occipitales postérieurement à la base du crâne.
- Palper les lymphatiques sous-maxillaires situés à l’angle de la mandibule, la lymphatiques sous-maxillaires à mi-chemin entre l’angle et la pointe et les nœuds sous-mentale quelques centimètres de l’extrémité. Notez que lymphatiques sous-maxillaires doivent être distinguée de la glande sous-maxillaire sous-jacente, qui est plus grand et sphériques.
- Palper les ganglions cervicaux superficielles et antérieures en avant et en recouvrant le muscle sternomastoïdien, respectivement. Lymphatiques cervicaux profonds, sous le muscle sternomastoïdien, sont rarement palpables.
- Palper les ganglions cervicaux postérieures entre le bord antérieur du trapèze et le bord postérieur de le sternomastoïdien.
- Palper les nœuds sus-claviculaires profondément dans l’angle formé par le muscle sternomastoïdien et la clavicule. Certains poumon et abdominale métastaser dans ces nœuds, donc ils ont peuvent être découvert lors de l’examen.
- Palper les nœuds infraclaviculaire sur le dessous de la clavicule.
2. axillae et membre supérieur

La figure 3. Ganglions axillaires.
Trois groupes de lymphatiques axillaires - brachiales, sous-scapulaire et pectoraux - déversent leurs ganglions dans les centrales lymphatiques axillaires qui pondent profondes au sein de la région axillaire contre la paroi thoracique, environ à mi-chemin entre les plis axillaires antérieurs et postérieurs (Figure 3). Ces nœuds, soutirer à son tour, dans l’infraclaviculaire (apical) et les lymphatiques sus-claviculaires. Des quatre groupes axillaires, seuls les nœuds centraux sont généralement palpables. Étant donné que la plupart des cancers du sein drain ici, les vaisseaux lymphatiques axillaires doivent être examinés soigneusement, surtout chez les femmes. Majeure partie des membres supérieurs de vidange plus ou moins directement dans les ganglions axillaires. Une seule exception est le drainage des aspects ulnaire de la main et l’avant-bras, qui rencontre d’abord les nœuds epitrochlear au-dessus du coude.
- Pour examiner les axillaires gauche, debout à l’avant et à gauche du patient assis, soutenir le bras du patient détendu gauche au poignet ou au coude.
- Informer le patient que l’examen peut se sentir un peu mal à l’aise.
- Rejoindre votre main droite en haut dans l’aisselle gauche, juste derrière le muscle pectoral, avec doigts pointant vers la milieu clavicule. Appuyez vos doigts contre la paroi thoracique et glissez-les vers le bas pour sentir les nœuds centraux.
- Si ne pas encore fait, palper l’infraclaviculaire (apical) et les lymphatiques sus-claviculaires.
- Alors que le bras gauche soutenant toujours du patient, palper les nœuds epitrochlear, qui sont trouvent en dedans environ 3 cm au-dessus du coude.
- Répétez les étapes 2.1-2.5 pour la région axillaire droite du patient et des membres supérieurs à l’aide de votre main gauche.
3. des membres inférieurs

La figure 4. Ganglions lymphatiques inguinaux superficiels.
Ganglions inguinaux superficiels (Figure 4) sont situés en haut de la cuisse antérieure et égoutter les diverses régions des jambes, abdomen et périnée. Ces nœuds sont souvent assez grands pour palper, même si c’est normal.
- Demander au patient de poser en décubitus dorsal avec hanches étirée ou légèrement fléchis.
- Palper un groupe horizontal de nœuds le long et juste inférieur à l’arcade crurale. Ces nœuds égoutter la fesse superficielle et le bas de l’abdomen, les organes génitaux externes (à l’exclusion des testicules), abaisser, vagin, canal anal et région périanale.
- Palper un groupe vertical de nœuds vers le groupe horizontal juste inférieur à la pulsation de l’artère fémorale. Ces nœuds se trouvent le long de la veine saphène supérieure et égoutter les mêmes régions des membres inférieurs.
Applications et Résumé
La plupart des ganglions lymphatiques se trouvent trop profondes pour être accessible par l’intermédiaire de l’examen physique. Les lymphatiques superficiels sont évaluées plus efficacement lors des examens régionaux de la tête et cou, seins et aisselles, membres supérieurs, membres inférieurs ou des organes génitaux externes. Parce que les ganglions lymphatiques sont en constante interaction avec vidange fluide extracellulaire des tissus voisins, leur examen peut fournir des informations sur la présence et l’état des infections ou des tumeurs malignes dans la région. Lymphatiques drainant le site d’une infection des tissus mous sont aptes à devenir élargie et tendre mais restent généralement doux, lisse et mobile. Nœuds durs, non-appel d’offres, emmêlés ou fixes sont plus typiques d’une malignité épandage. Adénopathie diffuse peut-être indiquer des maladies systémiques telles que les lymphomes, le VIH, la mononucléose ou sarcoïdose. Trouver un seul nœud anormal devrait inciter à un examen de tous les nœuds.
Passer à...
Vidéos de cette collection:

Now Playing
Examen des ganglions lymphatiques
Physical Examinations II
385.0K Vues

Examen des yeux
Physical Examinations II
76.6K Vues

Examen ophtalmologique
Physical Examinations II
67.3K Vues

Examen des oreilles
Physical Examinations II
54.5K Vues

Examen du nez, des sinus, de la cavité orale et du pharynx
Physical Examinations II
65.2K Vues

Examen de la thyroïde
Physical Examinations II
104.3K Vues

Examen abdominal I: Inspection et auscultation
Physical Examinations II
202.0K Vues

Examen abdominal II: Percussion
Physical Examinations II
247.4K Vues

Examen abdominal III: Palpation
Physical Examinations II
138.2K Vues

Examen abdominal IV: Évaluation de la douleur abdominale aiguë
Physical Examinations II
67.0K Vues

Toucher rectal chez l'homme
Physical Examinations II
113.7K Vues

Examen général des seins
Physical Examinations II
86.7K Vues

Examen pelvien I: Évaluation des organes génitaux externes
Physical Examinations II
304.1K Vues

Examen pelvien: Examen au spéculum
Physical Examinations II
149.5K Vues

Examen pelvien III: Examen bi-manuel et toucher rectal
Physical Examinations II
146.9K Vues
À PROPOS DE JoVE
Copyright © 2025 MyJoVE Corporation. Tous droits réservés.