
Method Article
Pletismografia simplificada de corpo inteiro para caracterizar a função pulmonar durante a melioidose respiratória
Neste Artigo
Resumo
Este protocolo apresenta a construção e utilização de um aparelho simplificado de pletismografia de corpo inteiro para monitorar a progressão da doença respiratória bacteriana de forma não invasiva.
Resumo
Modelos animais substitutos de doenças estão sujeitos aos 3Rs da Pesquisa Responsável. Há uma revisitação frequente de refinamentos em modelos animais para garantir que tanto o bem-estar animal quanto os insights científicos avancem com a disponibilidade de novas tecnologias. Este artigo demonstra o uso da Pletismografia Simplificada de Corpo Inteiro (sWBP) para estudar de forma não invasiva a insuficiência respiratória em um modelo de melioidose respiratória letal. O sWBP tem a sensibilidade de detectar a respiração em camundongos durante todo o curso da doença, permitindo que os sintomas associados à moribunda (bradipneia e hipopneia) sejam medidos e potencialmente usados para desenvolver critérios de desfecho humanos.
Alguns dos benefícios da WBP no contexto da doença respiratória são que o monitoramento da respiração do hospedeiro é o mais próximo de qualquer medida fisiológica na avaliação da disfunção do tecido primário infectado, ou seja, o pulmão. Além do significado biológico, o uso do sWBP é rápido e não invasivo, minimizando o estresse em animais de pesquisa. Este trabalho demonstra o uso de aparelhos sWBP internos para monitorar a doença ao longo do curso da insuficiência respiratória no modelo murino de melioidose respiratória.
Introdução
Patógenos bacterianos respiratórios estão frequentemente associados a uma resposta inflamatória no pulmão, levando à patologia pulmonar 1,2. No cenário clínico, o diagnóstico de pneumonia geralmente inclui técnicas de cultura de escarro, análise de saturação de oxigênio no sangue e radiografia de tórax. Essas técnicas podem ser traduzidas para modelos de infecção de pequenos animais, mas apenas a análise de saturação de oxigênio representa uma análise rápida e em tempo real em camundongos quanto à gravidade da doença. A saturação de oxigênio no sangue (SpO2) foi previamente investigada como método para rastrear a progressão da doença em estudos de doenças respiratórias; no entanto, camundongos moribundos têm leituras inesperadamente altas de SpO2 tanto em um modelo3 de Pseudomonas aeruginosa, que não são a doença preditiva ou moribunda, provavelmente porque os camundongos podem modular sua atividade fisiológica. Para este fim, os níveis diagnósticos de SpO2 não foram encontrados para doença respiratória bacteriana em camundongos até o momento.
Portanto, este trabalho investigou o uso de outros métodos clinicamente relevantes de detecção dos efeitos da doença pulmonar sobre a função pulmonar como uma medida fisiológica rápida. A Pletismografia Simplificada de Corpo Inteiro (sWBP) oferece a oportunidade de investigar a taxa de respiração e a profundidade como uma análise biométrica rápida e não invasiva. Estudos prévios demonstraram como montar aparelhos de WBP em laboratório4; no entanto, vários dos componentes mostrados em tais estudos não estão atualmente disponíveis comercialmente. Além disso, a WBP tradicional requer coleta e processamento de dados complexos com base na umidade e temperatura 5,6. Assim, optou-se por desenvolver um aparelho de WBP simplificado que seja calibrado diariamente para temperatura/umidade ambiente e avaliar se a contribuição temperatura/umidade do próprio sujeito tem ou não algum efeito sobre o volume respiratório medido. Assim, um aparelho sWBP modificado foi criado que fornece os materiais atualmente disponíveis. Além disso, tem sido investigado se este aparelho de origem laboratorial pode detectar alterações na respiração associadas à progressão da doença durante o modelo de melioidose respiratória letal em camundongos.
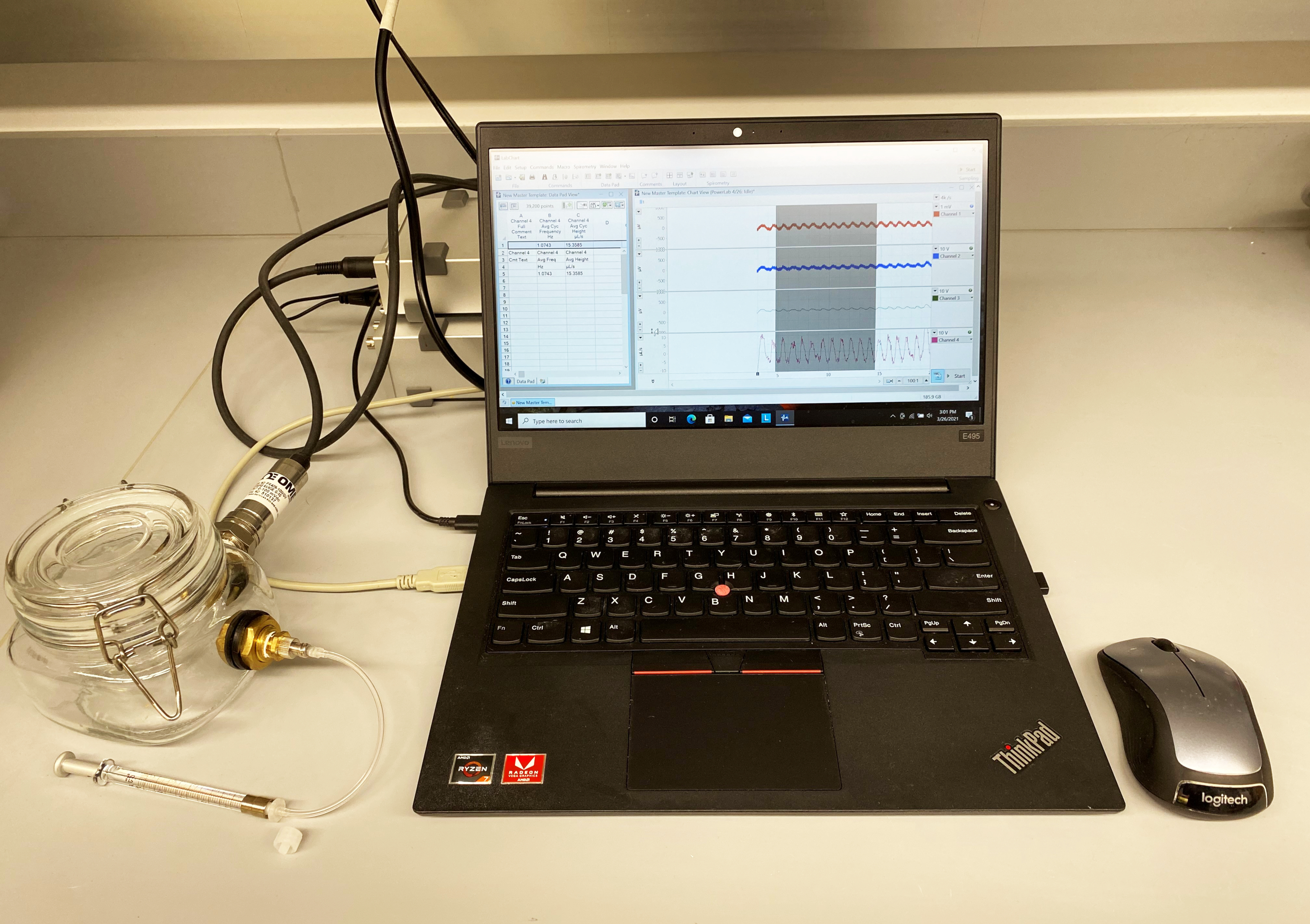
O aparelho sWBP construído para este trabalho usou equipamentos e softwares comercialmente disponíveis para processar dados de sensores de pressão analógicos em uma leitura digital. O sensor de pressão foi instalado em um frasco de vidro hermético com conectores de antepara. O benefício de um frasco de vidro é a rigidez estrutural do material, que resistirá a mudanças na pressão interna do frasco, afetando as medições de mudanças de volume durante o monitoramento da respiração. A câmara de amostragem foi projetada para ter duas portas nas duas superfícies planas do frasco quadrado, uma para acessar a câmara por um conector Luer para calibração e a outra para abrigar o sensor de pressão. O sensor de pressão selecionado tem um transdutor de pressão manométrica altamente sensível com uma faixa para pequenas mudanças de pressão (faixa de 25 mbar).
Este protocolo é demonstrado usando um modelo murino de melioidose respiratória. Burkholderia pseudomallei (Bp) é o agente bacteriano da melioidose - doença associada a regiões tropicais do mundo7. A pb é encontrada no ambiente, especificamente em ambientes úmidos de água parada e solo úmido, a partir do qual normalmente causa infecções subcutâneas de cortes/arranhões de hospedeiros suscetíveis. No entanto, a Bp também é infecciosa quando inalada e é uma ameaça potencial para uso em bioterrorismo por dispersão de aerossóis. Embora a Bp totalmente virulenta exija manuseio em um laboratório BSL-3, uma cepa mutante acapsular foi previamente projetada, que pode ser manuseada com segurança na BSL-2 e excluída dos critérios de agente selecionado8. Além disso, um modelo de infecção intratraqueal mediada por intubação (IMIT) de melioidose respiratória foi desenvolvido para estudar a progressão da doença respiratória da Bp 5,9. Utilizamos este modelo de infecção para caracterizar a mudança na respiração que ocorre durante a progressão da doença através do desfecho moribundo.
Protocolo
Os procedimentos aqui descritos foram revisados e aprovados pelo Comitê de Biossegurança Institucional da Universidade de Louisville (protocolo # 14-038) e pelo Comitê Institucional de Cuidados e Uso de Animais (protocolo # 19567).
1. Montagem da câmara de amostragem
- Crie dois furos usando uma broca diamantada de 3/4" em uma prensa de perfuração nas superfícies planas de um frasco de conserva Mason de boca larga de vidro quadrado de 600 mL com junta de 95 mm e tampas herméticas, com tampas de braçadeira de alça e gatilho (Figura 1).
NOTA: Uma câmara de amostragem não está comercialmente disponível e deve ser construída. - Monte uma antepara de latão (rosca interna NPT de 1/4", rosca externa 3/4-16 UNF) através de ambos os orifícios no frasco Mason usando arruelas de borracha (diâmetro interno de 3/4", diâmetro externo de 1") em ambas as faces de contato entre a antepara e o vidro para garantir uma vedação hermética.
- Use um conjunto de anteparas para um sensor de pressão enquanto conecta a outra antepara por uma seringa conectada por Luer para fins de calibração.
- Para o sensor de pressão, envolva as roscas NPT de 1/4" de um transdutor de pressão manométrica de alto desempenho com fita de Teflon e enfie-as na antepara. Use um ferro de solda para conectar a fiação do sensor de pressão a um conector DIN macho de 8 pinos, usando as instruções de fiação do fabricante para interface com um dispositivo de aquisição de dados de alta qualidade disponível comercialmente (consulte Tabela de materiais).
NOTA: Isso requer o uso de um resistor de filme metálico de 150 K ohm 1/8 watt 1% dentro da fiação do conector DIN. - Para a porta de calibração, use um adaptador NPT macho de 1/4" para NPT fêmea de 1/8" para conectar um NPT macho de 1/8" a um conector niquelado de bloqueio Luer fêmea à antepara de latão envolvendo conexões rosqueadas com fita de Teflon. Use uma tampa Luer macho rosqueada com polipropileno para selar o conector Luer quando não estiver em uso.
NOTA: Não aperte demais os conectores da antepara no frasco de vidro, pois isso desenvolverá rachaduras. Se desejado, o silicone pode ser adicionado às juntas de borracha para garantir uma vedação hermética das anteparas ao frasco de vidro.
- Para o sensor de pressão, envolva as roscas NPT de 1/4" de um transdutor de pressão manométrica de alto desempenho com fita de Teflon e enfie-as na antepara. Use um ferro de solda para conectar a fiação do sensor de pressão a um conector DIN macho de 8 pinos, usando as instruções de fiação do fabricante para interface com um dispositivo de aquisição de dados de alta qualidade disponível comercialmente (consulte Tabela de materiais).
2. Configuração do sistema
- Conecte a câmara de amostragem a um amplificador de ponte usando um conector DIN de 8 pinos e o amplificador de ponte ao dispositivo de aquisição de dados, seguindo as instruções do fabricante.
- Conecte o dispositivo de aquisição de dados a uma fonte de alimentação e a um computador executando um software de análise de dados fisiológicos usando os cabos do fabricante.
NOTA: Certifique-se de que o dispositivo de aquisição de dados esteja ligado e aquecido por pelo menos 5 minutos antes do uso para garantir que o sensor estabilize suas medições. - Inicie o software para fazer a interface com o sistema de aquisição de dados.
- Baixe o Módulo de Espirometria opcional dentro do software e modifique as configurações padrão da unidade de L/s para μL/s na janela Configurações de > de Espirometria.
3. Calibração do sistema
- Dentro do software, crie uma janela de 4 canais com as seguintes janelas de dados: Canal 1: Dados de origem a uma taxa de amostragem de 4 k/s e faixa de 1 mV ; Canal 2: Filtro digital do Canal 1 usando um filtro de ajuste automático de 1 Hz passa-alta; Canal 3: Suavização dos dados do Canal 2 por uma média de 100 amostras; Canal 4: Espirometria Fluxo de dados do Canal 3 (Flowhead Personalizado, calibrado para Fórmula (μL/s) = 120.000 x Tensão).
NOTA: 120.000 é um coeficiente de correlação de espaço reservado que será modificado durante a calibração. - Configure a análise do DataPad do Channel 4 com as seguintes Colunas: Coluna 1: Dados do Channel 4, Comentários > Texto de comentário completo; Coluna 2: Dados do Canal 4, Medições Cíclicas > Frequência Cíclica Média; Coluna 3: Dados do Canal 4, Medições Cíclicas > Altura Cíclica Média.
- Defina a taxa de quadros como 100:1 no canto inferior direito da exibição do gráfico. Salve esta configuração de janela como um modelo para todos os estudos futuros.
- Feche a tampa da câmara de amostra e fixe uma seringa à prova de gás de 25 μL ao conector da antepara Luer. Ajuste a seringa com um adaptador Chaney ajustado para fornecer repetidamente um volume de 20 μL.
NOTA: Uma peça curta opcional de tubo de 1/16" e conectores Luer/barb pode ser usada para conectar a seringa à Câmara de Amostragem. No entanto, a tubulação longa deve ser evitada para evitar alterações significativas no volume total de ar da Câmara de Amostragem. - Desenhe 20 μL de ar para a seringa utilizando a paragem de profundidade do adaptador Chaney.
- Zere o pleth no software (Configuração > Zero Todas as Entradas (Alt-Z)) e inicie uma gravação.
- Durante a gravação, e com uma linha de base estável, deprimir/retirar rapidamente o êmbolo da seringa por aproximadamente 10 repetições para replicar a respiração do sujeito com uma respiração medida de 20 μL. Pare a gravação.
NOTA: A frequência das respirações artificiais deve exceder 2 Hz para maximizar a reprodutibilidade da calibração. - Rotule a identidade da amostra medida clicando com o botão direito do mouse no início da gravação de pleth numerada e clique em Adicionar comentário.
- Redefina a seringa, zere a entrada e repita as medições de gravação de pulsos de 20 μL duas vezes adicionais (três sessões de gravação totais).
- Depois de completar todas as medições, use o mouse do computador para selecionar uma porção de pleth respiratório que represente com precisão as respirações artificiais de 20 μL.
NOTA: Dentro do módulo DataPad, os dados aparecerão no cabeçalho de visualização fornecendo uma leitura temporária da taxa de respiração (Frequência Cíclica Média, Hz) e profundidade de respiração (Altura Cíclica Média, μL). A visualização de dados pode ser gravada no DataPad usando o ícone Adicionar ao DataPad . - Revise os dados da Coluna 3 (Altura Cíclica Média) e calcule o volume médio de respiração medido a partir das três gravações. Realize o seguinte cálculo do volume respiratório médio medido: Coeficiente de calibração = volume entregue / volume medido x 120.000.
NOTA: 120.000 foi o coeficiente de calibração da cabeça de fluxo de espaço reservado usado na etapa 3.1 agora modificado a partir dos dados medidos. O sistema agora é calibrado para a respiração típica do mouse usando a temperatura e a umidade ambientais atuais. O sistema agora pode monitorar a respiração do sujeito, e a calibração pode ser rerealizada diariamente para levar em conta qualquer flutuação na temperatura / umidade.
4. Monitorização dos sujeitos
- Abra um modelo mestre conforme descrito na etapa 3.4 ou conclua as etapas 4.2 a 4.3.
- Dentro do software, crie uma janela de 4 canais com o seguinte processamento de dados: Canal 1: Dados de origem a uma taxa de amostragem de 4 k/s e faixa de 1 mV ; Canal 2: Filtro digital do Canal 1 usando um filtro High Pass 1 Hz Auto Adjust; Canal 3: Suavização dos dados do Canal 2 por Média de 100 Amostras; Canal 4: Espirometria Fluxo de dados do Canal 3 (Flowhead Personalizado, calibrado para Fórmula (μL/s) = 120.000 x Tensão).
NOTA: 120.000 é o coeficiente de correlação calculado para o sensor de pressão de corrente; no entanto, o usuário deve executar a calibração do sistema descrita na etapa 3 e usar esse coeficiente de correlação definido pelo usuário. - Configure a análise do DataPad do Channel 4 com as seguintes Colunas: Coluna 1: Dados do Channel 4, Comentários > Texto de comentário completo; Coluna 2: Dados do Canal 4, Medições Cíclicas > Frequência Cíclica Média; Coluna 3: Dados do Canal 4, Medições Cíclicas > Altura Cíclica Média.
- Coloque o sujeito na câmara de amostragem e feche a tampa. Para este experimento foi utilizado um camundongo albino C57BL/6J fêmea consciente de 4-12 semanas (B6(Cg)-Tyrc-2J/J).
- Equalize a pressão atmosférica na câmara (a partir da vedação da tampa) afrouxando brevemente a tampa da antepara Luer e aperte novamente.
- Observe que o sujeito não está se movendo ativamente dentro da câmara de amostragem antes de zerar todas as entradas (atalho Alt-Z) e iniciar uma gravação.
NOTA: Se o sujeito começar a se mover na câmara de amostragem, a linha de base pode sair da escala, o que pode ser resolvido zerando novamente todas as entradas no meio de uma gravação, o que criará uma nova gravação na escala. Suponha que o sujeito se envolva em exploração ou preparação durante a gravação; observe qual parte do registro da pletismografia reflete com mais precisão a respiração normal. - Rotule a identidade do sujeito clicando com o botão direito do mouse no início da gravação de pleth numerado e clique em Adicionar comentário.
- Devolva o objeto à sua gaiola. Limite o tempo gasto na câmara de amostragem selada a 5 minutos para evitar asfixia e estresse.
NOTA: O risco de asfixia é baixo, dado que o volume de ar de 600 ml da Câmara de Amostra não será rapidamente gasto por um rato saudável a respirar a <15 ml/min. - Use o mouse do computador para selecionar uma parte da totalidade da respiração que represente com precisão a respiração do sujeito.
NOTA: Dentro do módulo DataPad, os dados aparecerão no cabeçalho de visualização fornecendo uma leitura temporária da taxa de respiração (Frequência Cíclica Média, Hz) e do volume de respiração (Altura Cíclica Média, μL). A visualização de dados pode ser gravada no DataPad usando o ícone Adicionar ao DataPad . - Continue medindo os ratos sujeitos, um de cada vez, e registre seções representativas da totalidade respiratória para o DataPad.
- Após a gravação dos dados, exporte os dados do DataPad para o Excel. Calcule o volume minuto da seguinte forma: Volume minuto (mL/min) = Taxa de Respiração (Hz) x Volume de Respiração (μl) x 0,06.
Resultados
Calibração do sistema
O software de análise de dados permite a calibração direta de uma cabeça de fluxo personalizada, como a descrita aqui. Isso é realizado ao definir o Fluxo de Espirometria. Conforme descrito na etapa 3.1, existe uma opção para inserir o volume de ar de calibração conhecido, que calcula o coeficiente de correlação tensão-volume dentro do sistema. Isso, no entanto, gera um coeficiente de correlação baseado em uma única leitura, e observou-se que a variação inerente da calibração de um padrão n = 1 tem pouca utilidade. A abordagem atual pode resolver essa deficiência e permite que um usuário execute uma calibração diária usando várias leituras calculadas em média para calcular um coeficiente de calibração. A calibração com 20 μL de ar injetado foi demonstrada aqui, representando um volume de respiração típico de alta qualidade em um rato típico. O software assume um intercepto de origem (0,0) e, portanto, é calibrado de 0-20 μL usando essa abordagem.
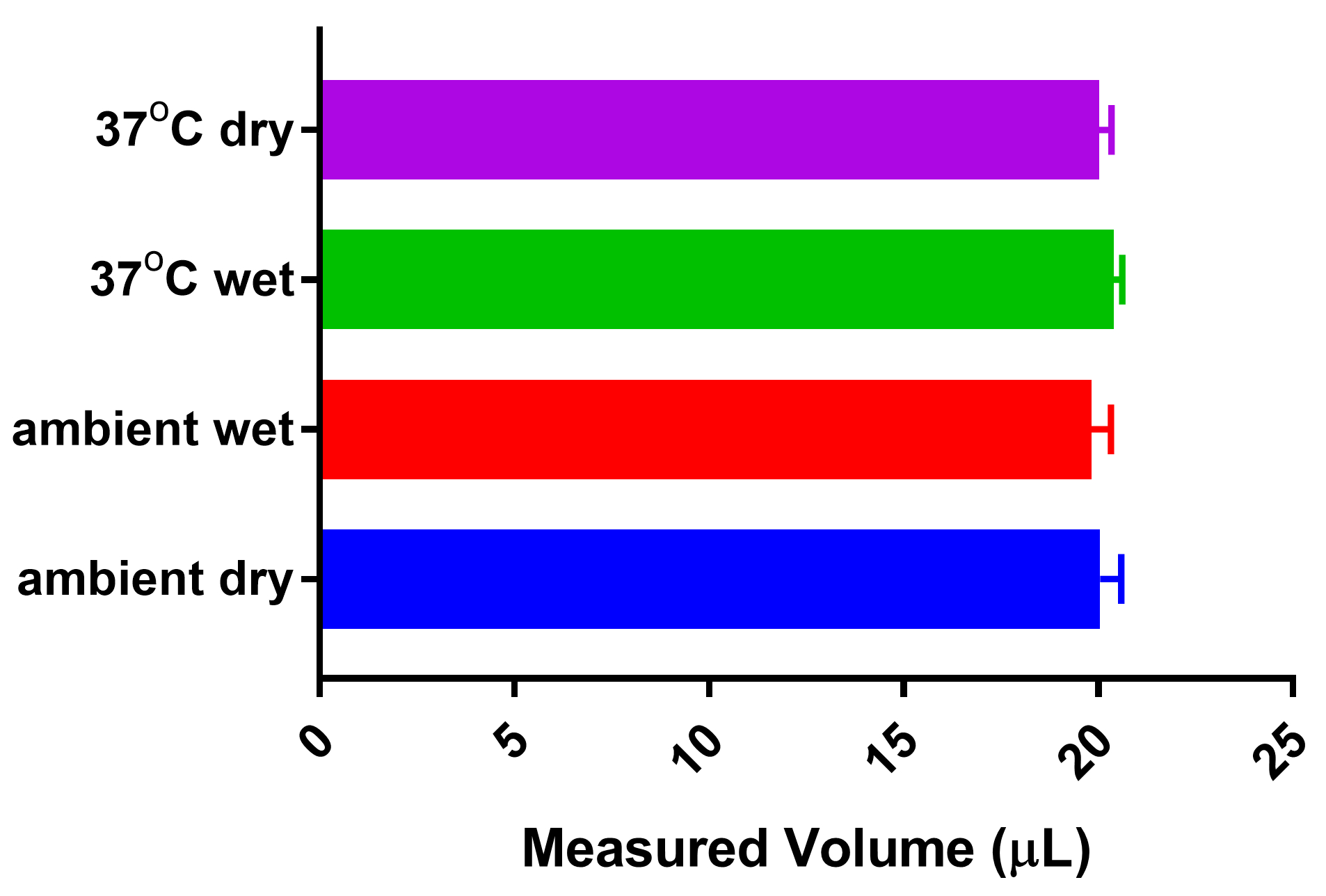
A metodologia aqui proposta para o sWBP calibra diariamente, contabilizando assim quaisquer flutuações na umidade/temperatura ambiental. Os métodos originais utilizados para a WBP específica, remontam à metodologia de Drorbaugh e Fenn de 1955, que desenvolveram a WBP para medir a ventilação em lactentes humanos5. Os cálculos de Drorbaugh e Fenn explicam as variações de temperatura e umidade do ambiente e do sujeito. A abordagem atual corrige as flutuações ambientais calibrando cada sessão sWBP. Ainda assim, decidiu-se abordar se o aquecimento e a umidificação da respiração através da cavidade nasal / pulmão de um rato afetam a medição de um volume conhecido de ar. Assim, um aparelho artificial foi criado para imitar o efeito do sujeito no aquecimento e umidificação de medições de ar calibrado. Os conectores Luer foram fixados a um tubo cônico de 15 mL e colocados em linha cônica selada entre a câmara de amostra e a seringa de calibração à prova de gás. Uma calibração de 20 μL foi realizada usando um tubo cônico vazio mantido à temperatura ambiente (23 °C). O tubo cônico foi então parcialmente preenchido com água destilada logo abaixo dos conectores Luer, permitindo tempo para equilibrar o espaço cefálico do cônico; o volume de calibração foi então remedido para investigar o efeito da umidade. O tubo cônico foi colocado em bloco de aquecimento e equilibrado a 37 °C em ambiente úmido e, finalmente, equilibrado a 37 °C sem água para avaliar o efeito do aquecimento do sujeito e sem contribuição adicional de umidade. A Figura 2 demonstra que todas as condições testadas não impactaram significativamente a medição calibrada de 20 μL fornecida pela seringa à prova de gás. A partir desse achado, concluiu-se que o sWBP oferece uma abordagem acessível para monitorar a respiração em animais de pesquisa sem a necessidade de cálculos complexos baseados na temperatura e umidade do animal sujeito, uma vez que estes não causam impacto significativo no volume respiratório medido.
Monitoramento do assunto
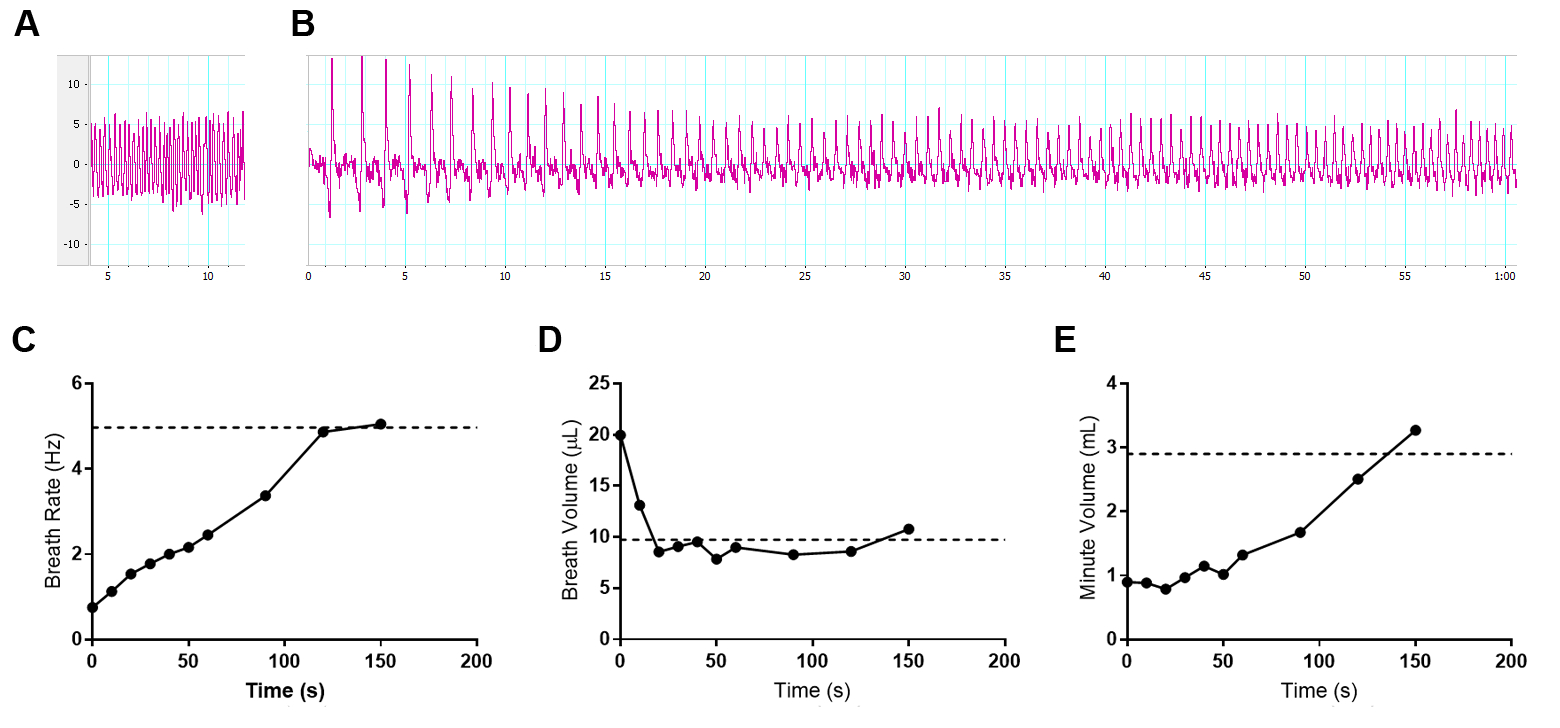
A espa foi utilizada para monitorar a respiração durante a doença de infecções respiratórias letais com o patógeno bacteriano B. pseudomallei. Um desafio de monitorar a respiração em animais conscientes é a curiosidade de animais saudáveis normais que se movem dentro da câmara de amostragem. O movimento do mouse cria uma linha de base em constante movimento que pode ser mitigada em parte pelo pré-condicionamento dos sujeitos à câmara durante um período de vários dias antes da medição. Esse problema afeta principalmente a medição basal em camundongos saudáveis, pois os indivíduos se tornam letárgicos durante a infecção, tornando a sWBP muito mais gerenciável com a atividade reduzida do sujeito. Pode ser tentador tentar usar alguma forma de restrição, seja física ou anestésica. O uso de contenção física pode afetar a respiração natural, causando estresse. Além disso, sabe-se que o uso de anestésicos tem efeitos pronunciados sobre a frequência respiratória e a profundidade10; assim, optou-se por investigar o impacto da anestesia com o aparelho sWBP interno. O isoflurano é comumente usado para realizar imagens diagnósticas in vivo durante os modelos de infecção e, portanto, um camundongo C57BL/6 foi anestesiado e monitorou a progressão até a recuperação da anestesia usando sWBP. Este ensaio foi conduzido com um rato albino C57BL/6J juvenil de 4 semanas de idade para prolongar a janela de recuperação da anestesia. A Figura 3 demonstra que o anestésico preferido faz com que os camundongos exibam uma taxa de respiração lenta com um grande volume corrente de ar. À medida que os ratos começam a se recuperar da sedação, sua taxa de respiração aumenta e o volume de respiração diminui, com o efeito líquido de que o ar total inspirado aumenta lentamente. Neste ensaio, verificou-se que o volume da respiração é restaurado aos níveis pré-anestésicos nos primeiros 30 s de recuperação. A taxa de respiração aumenta constantemente até que a respiração basal seja restaurada para 2-2,5 minutos após a remoção da anestesia. O volume minuto acompanhou de perto os efeitos da frequência respiratória, atingindo o volume minuto basal em 2,5 min após a remoção da anestesia. Esse achado sustenta que a anestesia não deve ser empregada na abordagem da espácea. Isso afeta drasticamente a respiração basal, não surpreendentemente, pois a anestesia retardará o metabolismo do hospedeiro, criando uma demanda reduzida por oxigênio inspirado. O saneamento da câmara de amostra também deve ser considerado entre os sujeitos para abordar o controle de infecção específico do estudo, bem como o impacto dos feromônios da urina ou fezes, o que poderia afetar o estresse entre os indivíduos.
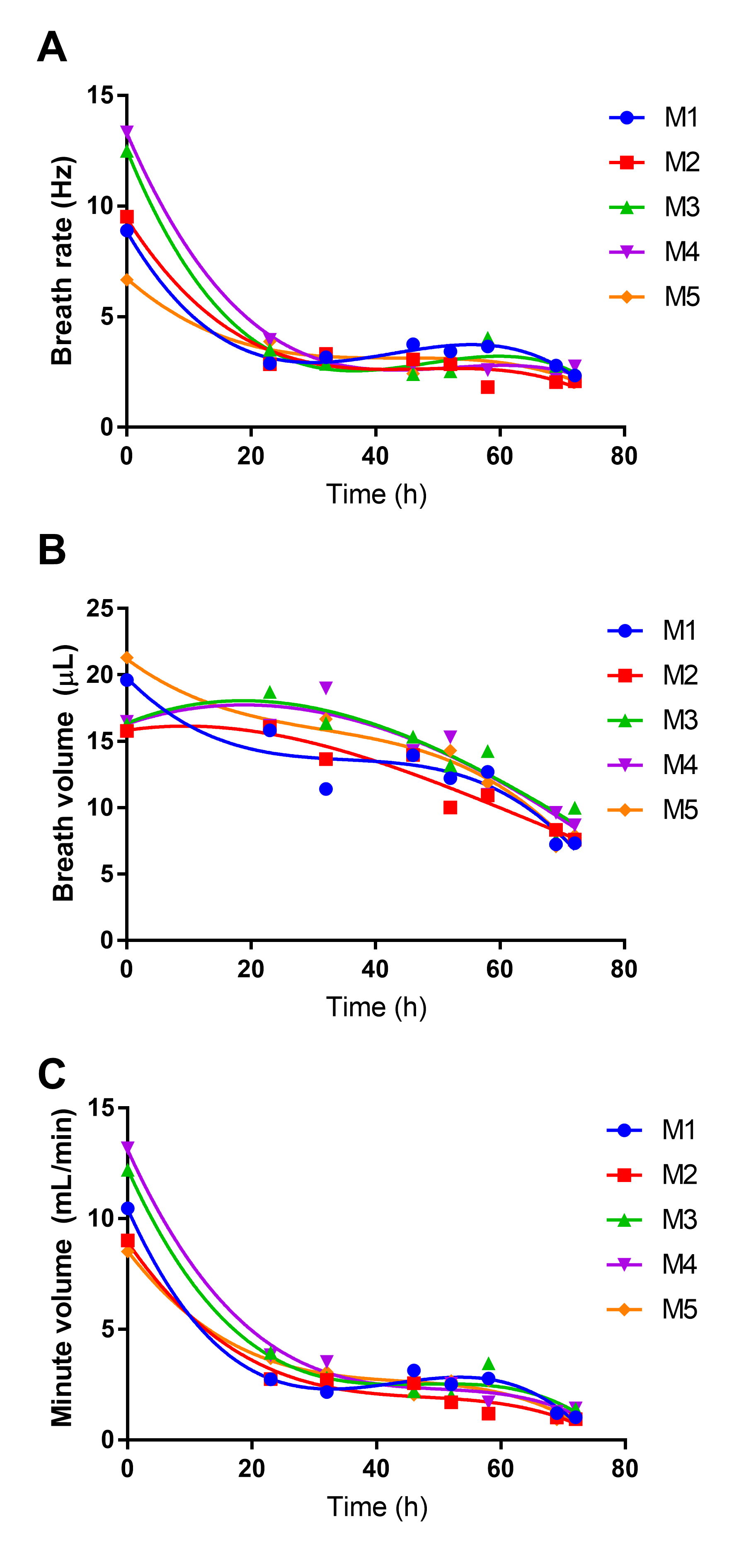
A WBP é uma estratégia atraente para monitorar a função pulmonar em modelos de doenças respiratórias de forma não invasiva. A WBP foi utilizada para estudar como a respiração muda durante infecções letais de melioidose respiratória (Figura 4), com pontos de tempo espelhando o monitoramento da bioluminescência no pulmão. Observou-se que esse modelo está associado a um início precoce da letargia, que persiste de forma lentamente progressiva até o desenvolvimento da doença moribunda em aproximadamente 3 dias pós-infecção. Observou-se também que a frequência respiratória e o ar inspirado total (volume minuto) dos camundongos diminuem rapidamente durante o primeiro dia de infecção e permanecem baixos pelo restante do curso da infecção (Figura 4A,C). Este padrão é consistente com a letargia de início precoce, que persiste pelos próximos 2 dias da infecção. Em contraste, o volume da respiração não cai acentuadamente durante as primeiras 24 horas e, em vez disso, tem uma ligeira e constante diminuição, o que se aproxima de um declínio linear ao longo do curso de 3 dias da doença (Figura 4B).

Figura 1: Aparelho sWBP. Uma Câmara de Amostra personalizada foi construída a partir de um frasco de vidro quadrado selado com conectores de anteparo em duas faces planas. Uma antepara foi usada para montar um sensor de pressão manométrica conectado a um amplificador de ponte e digitalizador de dispositivo de aquisição de dados através de uma conexão DIN de 8 pinos. A segunda antepara foi equipada com um conector Luer para calibração por uma seringa à prova de gás. O dispositivo foi conectado a um PC que executa o software. Por favor, clique aqui para ver uma versão maior desta figura.
{kind=link}

Figura 2: Efeito da temperatura e umidade do sujeito sobre o volume de respiração. Um tubo cônico de 15 mL com conectores Luer foi instalado em linha entre a seringa de calibração de 20 μL e a Câmara de Amostragem. O sistema foi calibrado para 20 μL sem contribuição adicional de temperatura/umidade do tubo cônico. Outras medidas foram coletadas pós-equilíbrio com umidade saturada da água destilada e/ou aquecimento do tubo cônico da temperatura ambiente (23 °C) para a temperatura corporal (37 °C). Nenhuma diferença significativa foi detectada a partir de n = 5 medidas de cada condição por ANOVA One-way com o pós-teste de Comparação Múltipla de Tukey. Por favor, clique aqui para ver uma versão maior desta figura.
{kind=link}

Figura 3: Efeito da anestesia gasosa na respiração em camundongos. Dados representativos de uma rata albina C57BL/6J fêmea de 4 semanas de idade (8,6 g) foram sedados por 5 min com isoflurano a 3% em oxigênio e transferidos para uma Câmara de Amostra de WBP. Os dados de pleth foram coletados por 150 s após a remoção da anestesia. O sujeito iniciou a deambulação inicial por volta de 100 s após a remoção da anestesia. (A) Respiração basal antes da anestesia, medindo uma frequência respiratória de 4,97 Hz, volume respiratório de 9,74 μL e volume minuto de 2,91 mL. (B) Os primeiros 60 s de mudanças na respiração durante a recuperação da anestesia. (A-B) Eixo vertical medindo μL por respiração e eixo horizontal em segundos. (C-E) Os dados de ventilação foram coletados durante os 150 s de recuperação da anestesia, em média de ≥3 ciclos de respiração por ponto de tempo para (C) Taxa de Respiração, (D) Volume de Respiração e (E) Volume de Minutos calculado. Os valores basais pré-anestésicos são indicados com uma linha pontilhada horizontal em cada gráfico respectivo. Por favor, clique aqui para ver uma versão maior desta figura.
{kind=link}

Figura 4: Efeito da melioidose respiratória na respiração do hospedeiro. Cinco camundongos fêmeas C57BL/6 de 8 semanas foram infectados com 4,9 log CFU da cepa bioluminescente de B. pseudomallei JW270. A WBP foi realizada ao longo dos 3 dias de infecção, medindo-se a Taxa de Respiração (A) e o Volume de Respiração (B). O ar total inspirado foi calculado como Volume Minuto (C). Os dados para cada um dos cinco sujeitos são plotados independentemente com regressão polinomial de terceira ordem. Por favor, clique aqui para ver uma versão maior desta figura.
{kind=link}
Discussão
A WBP é uma abordagem atraente para melhorar a compreensão da infecção respiratória em modelos de pequenos animais. É importante ressaltar que é uma abordagem não invasiva e, como tal, não representa um risco significativo de causar estresse indevido aos animais de pesquisa durante um desafio de infecção. De fato, o procedimento de monitoramento da respiração do sujeito é um teste rápido que requer vários minutos e manuseio mínimo do sujeito. O benefício científico é a compreensão de alta resolução de como os patógenos microbianos influenciam a função pulmonar durante a doença. Essa abordagem proporcionará benefícios à pesquisa básica, facilitando a compreensão de como um patógeno causa a doença, além de fornecer uma utilidade translacional para entender como uma nova terapêutica restaura uma pesquisa sujeita a um estado de saúde respiratória.
Neste manuscrito, resultados representativos são fornecidos para o patógeno B. pseudomallei, que causa uma resposta letárgica precoce. Nem todas as infecções pulmonares bacterianas estão presentes da mesma maneira em modelos de infecção de camundongos. A experiência prévia com outros modelos de infecção demonstrou que o patógeno bacteriano Klebsiella pneumoniae se apresenta como uma infecção assintomática até o ponto em que camundongos sucumbem à infecção, também aproximadamente no 3º dia pós-infecção11. Hipotetiza-se que a demanda do hospedeiro por ar inspirado (ou seja, volume minuto) pode estar intimamente relacionada ao grau de letargia com que uma determinada doença se apresenta. Estudos futuros serão necessários para examinar como diferentes patógenos bacterianos afetam a função pulmonar durante a doença respiratória. Entende-se que diferentes patógenos têm abordagens únicas para evitar a defesa do hospedeiro, incluindo diferenças em, (1) propensão a serem patógenos intracelulares ou extracelulares, (2) a capacidade de causar resposta hipotérmica precoce/tardia e (3) uso de diferentes repertórios de determinantes de virulência 3,12,13. Portanto, é provável que diferentes estratégias de doença resultem em efeitos únicos na função pulmonar e na respiração durante a infecção.
As configurações recomendadas descritas neste protocolo podem ser modificadas para acomodar desafios exclusivos presentes durante o sWBP. Um dos problemas comuns experimentados durante uma sessão de gravação do sWBP é o movimento do sujeito dentro da Câmara de Amostras. Como mencionado, esse movimento modifica a linha de base e pode afetar a precisão das medidas respiratórias. Um filtro digital foi usado para normalizar a linha de base de deslocamento, permitindo medições viáveis da respiração, apesar de pequenos movimentos. O movimento excessivo pode empurrar uma medida de linha de base para fora do intervalo de uma entrada zerada. As gravações são recomendadas na faixa de 1 mV (configuração do Canal 1), o que proporciona um compromisso de ainda observar os picos da pletismografia, evitando a perda de dados fora do intervalo. Para indivíduos excepcionalmente ativos, pode ser necessário estender a faixa de gravação >1 mV para evitar sinais persistentes fora do alcance.
O procedimento recomendado exige calibração diária (ou em cada sessão) para acomodar as flutuações de umidade/temperatura do ambiente. A WBP tradicional utiliza cálculos complexos que levam em conta a temperatura/umidade do ambiente e do sujeito 5,6. Demonstrou-se que, no presente aparelho de oscilação do hospedeiro, os efeitos da temperatura/humidade do hospedeiro não alteram significativamente o volume respiratório medido de uma fonte de calibração. Portanto, essa abordagem no sWBP difere fundamentalmente da abordagem de >50 anos de idade de Drorbaugh e Fenn. Aqui, a sWBP relaciona diretamente as mudanças de pressão a um volume de respiração medido sem correção adicional do hospedeiro.
É essencial contrastar o WBP animal de pesquisa com o WBP clínico. Os tipos de dados biométricos que foram tentados coletar por WBP são o volume e a frequência da respiração. Tais medições são coletadas clinicamente usando um equipamento de espirometria simples no qual um paciente prende um monitor de respiração à boca e respira normalmente em um dispositivo de monitoramento do fluxo de ar. Espirometria semelhante em animais de pesquisa requer contenção, contribuindo assim para o estresse e uma interrupção inerente na respiração. Portanto, a espirometria simples é funcional clinicamente, mas não para animais de pesquisa. A WBP serve a um propósito essencial na clínica para coletar dados avançados, incluindo medições como o volume pulmonar residual. Tais dados só podem ser contidos no contexto de um sujeito ser capaz de seguir instruções sobre como eles respiram, incluindo a expiração forçada (esvaziamento de seu pulmão por uma expiração profunda). Não se pode confiar que os animais de pesquisa sigam as instruções de respiração de um pesquisador. Muitas das medidas avançadas coletadas clinicamente durante a WBP não podem ser reproduzidas em animais de pesquisa. O WBP em animais de pesquisa é fundamentalmente diferente do WBP clínico. A WBP animal procura coletar dados de ventilação simples (taxa de respiração e volume) de forma não contida para evitar o estresse animal e a perturbação respiratória. Até o momento, o uso de WBP em animais de pesquisa parece replicar as técnicas usadas na WBP clínica, incluindo cálculos complexos com base na temperatura e umidade ambiental e do sujeito, mas sem a capacidade de coletar os dados avançados de um sujeito que possa seguir instruções sobre como realizar uma expiração forçada. Com isso em mente, buscou-se demonstrar se uma versão simplificada da WBP seria suficiente para coletar a frequência e o volume respiratórios pertinentes relevantes para os estudos de doenças respiratórias. Foi empregada uma sessão de calibração, que compensou qualquer variação na temperatura e umidade do ambiente. Além disso, foi demonstrado com um rato artificial que a temperatura e a umidade de um volume respiratório medido não têm efeito significativo na medição precisa do volume da respiração. Concluiu-se que o sWBP tem excelente aplicação para pesquisas em estudos com animais, sem a exigência do usuário de empregar um tratamento matemático complicado dos dados.
Divulgações
Os autores não têm conflitos de interesse.
Agradecimentos
Estes estudos foram apoiados pelo National Institutes of Health COBRE grant P20GM125504-01 Sub-Project 8246.
Materiais
| Name | Company | Catalog Number | Comments |
| 1/8" NPT Luer adaptor | Amazon | B07DH9MY8W | Calibration port |
| 1/8" NPT to 1/4" NPT adaptor | Amazon | B07T6CR6FS | Bulkhead to luer adaptor |
| 150 kohm resistor | Amazon | B07GPRYL81 | Pressure transducer excitation voltage selection |
| 3/4" diamond drill bit | Drilax | DRILAX100425 | To drill bulkhead mounts in glass jar |
| Bridge Amp | AD Instruments | FE221 | One channel option |
| Bulkhead fitting | Legines | 3000L-B | 1/4" NPT, 3/4-16 UNF brass bulkhead coupling |
| Chaney adaptor | Hamilton | 14725 | Gas tight syringe adaptor for set volume |
| DIN connector | AD Instruments | SP0104 | To connect pressure sensor to Bridge Amp |
| Gastight syringe, 25 uL | Hamilton | 80201 | Calibration syringe |
| LabChart | AD Instruments | Life Science Data Acquisition Software | |
| Luer plug | Cole Parmer | 45513-56 | Calibration port closure |
| PowerLab 4/26 | AD Instruments | PL2604 | Digital interface to computer |
| Pressure transducer | Omega Engineering | PX409-10WGV | High accuracy oil filed gage pressure sensor |
| Rubber gasket | Amazon | B07LH4C8LS | To mount bulkheads (4 required per chamber) |
| Square glass jar | Amazon | B07VNSPR8P | 600 ml with 95 mm silicone gasket |
Referências
- Warawa, J. M., Long, D., Rosenke, R., Gardner, D., Gherardini, F. C. Role for the Burkholderia pseudomallei capsular polysaccharide encoded by the wcb operon in acute disseminated melioidosis. Infection and Immunity. 77 (12), 5252-5261 (2009).
- West, T. E., Myers, N. D., Liggitt, H. D., Skerrett, S. J. Murine pulmonary infection and inflammation induced by inhalation of Burkholderia pseudomallei. International Journal of Experimental Pathology. 93 (6), 421-428 (2012).
- Lawrenz, M. B., et al. Development and evaluation of murine lung-specific disease models for Pseudomonas aeruginosa applicable to therapeutic testing. Pathogens and Disease. 73 (5), (2015).
- Lim, R., et al. Measuring respiratory function in mice using unrestrained whole-body plethysmography. Journal of Visualized Experiments: JoVE. (90), e51755(2014).
- Drorbaugh, J. E., Fenn, W. O. A barometric method for measuring ventilation in newborn infants. Pediatrics. 16 (1), 81-87 (1955).
- Simon, G., Pride, N. B., Jones, N. L., Raimondi, A. C. Relation between abnormalities in the chest radiograph and changes in pulmonary function in chronic bronchitis and emphysema. Thorax. 28 (1), 15-23 (1973).
- Gassiep, I., Armstrong, M., Norton, R. Human melioidosis. Clinical Microbiology Reviews. 33 (2), 06-19 (2020).
- Gutierrez, M. G., Warawa, J. M. Attenuation of a select agent-excluded Burkholderia pseudomallei capsule mutant in hamsters. Acta Tropica. 157, 68-72 (2016).
- Gutierrez, M. G., Pfeffer, T. L., Warawa, J. M. Type 3 secretion system cluster 3 is a critical virulence determinant for lung-specific melioidosis. PLoS Neglected Tropical Diseases. 9 (1), 3441(2015).
- Rocco, P. R. M., Zin, W. A. Anaesthesia, Pain, Intensive Care and Emergency Medicine. Gullo, A. , Springer. (2002).
- Fodah, R. A., et al. Correlation of Klebsiella pneumoniae comparative genetic analyses with virulence profiles in a murine respiratory disease model. PLoS One. 9 (9), 107394(2014).
- Gotts, J. E., et al. Clinically relevant model of pneumococcal pneumonia, ARDS, and nonpulmonary organ dysfunction in mice. American Journal of Physiology-Lung Cellular and Molecular Physiology. 317 (5), 717-736 (2019).
- Galan, J. E. Common themes in the design and function of bacterial effectors. Cell Host & Microbe. 5 (6), 571-579 (2009).
Reimpressões e Permissões
Solicitar permissão para reutilizar o texto ou figuras deste artigo JoVE
Solicitar PermissãoExplore Mais Artigos
This article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. Todos os direitos reservados