
A subscription to JoVE is required to view this content. Sign in or start your free trial.
Method Article
Providing Visual Biofeedback Using Brightness Mode Ultrasound During a Golf Swing
In This Article
Summary
Brightness mode ultrasound can be used to provide visual biofeedback of the muscles of the lateral abdominal wall during a golf swing. Post-swing visual and verbal instruction can increase the muscle activation and timing of the external and internal obliques.
Abstract
Using ultrasound biofeedback in conjunction with verbal cueing can increase muscle thickness more than verbal cueing alone and may augment traditional rehabilitation techniques in an athletic, physically active population. Brightness mode (B-mode) ultrasound can be applied using frame-by-frame analysis synchronized with video to understand muscle thickness changes during these dynamic tasks. Visual biofeedback with ultrasound has been established in static positions for the muscles of the lateral abdominal wall. However, by securing the transducer to the abdomen using an elastic belt and foam block, biofeedback can be applied during more specific tasks prevalent in lifetime sports, such as golf. To analyze muscle activity during a golf swing, muscle thickness changes can be compared. The thickness must increase throughout the task, indicating that the muscle is more active. This methodology allows clinicians to immediately replay ultrasound videos for patients as a visual tool to instruct proper activity of the muscles of interest. For example, ultrasound can be used to target the external and internal obliques, which play an important role in swinging a golf club or any other rotational sport or activity. This methodology aims to increase oblique muscle thickness during the golf swing. Additionally, the timing of muscle contraction can be targeted by instructing the patient to contract the abdominal muscles at specific time points, such as the beginning of the downswing, with the goal of improving muscle firing patterns during tasks.
Introduction
The muscles of the lateral abdominal wall include the external oblique, internal oblique, and transverse abdominis. The external obliques perform lateral flexion and contralateral trunk rotation, while the internal obliques perform ipsilateral trunk rotation. The transverse abdominis is the deepest layer of the abdominal musculature, and it functions to increase intra-abdominal pressure and increase the segmental stability of the spine1. The proper function of these muscles is important to reduce low back pain risk and improve athletic performance as core stability allows for increased strength and power through the extremities2.
During sports with an emphasis on trunk rotation, such as golf, tennis, baseball, or softball, there is a high demand for the core muscles. For example, during a golf swing, the obliques on the trail side of the body peak at 64% of the maximal voluntary isometric contraction (MVIC) when measured using surface electromyography, while the lead obliques peak at 54% MVIC3. Trunk rotation is a key contributor to the distance and accuracy of golf shots4. The stresses of the golf swing and the high demand for core muscle activity may contribute to low back pain, which is the most common injury in golf5. Additionally, in elite golfers with low back pain, the timing of external oblique activity is delayed during the golf swing compared to healthy individuals6. Another study using electromyography found golfers with low back pain have an earlier onset of the erector spinae than golfers without low back pain7, suggesting a focus on anterolateral muscles may be beneficial. Therefore, measuring the extent and timing of abdominal muscle activity during a golf swing is important to improve performance and reduce the risk of low back pain.
Rehabilitative ultrasound is commonly used to assess lateral abdominal wall muscles due to the layered nature of this musculature8,9,10. There is no difference in transverse abdominis activation in college golfers with and without low back pain in the supine position or in a more functional golf swing setup position11. However, transverse abdominis activity is only one component of a golf swing, and rotation may be more important for this population. Previous literature has used an elastic belt and foam block to secure the ultrasound transducer to the abdomen, allowing for ultrasound assessment of the core musculature during dynamic movement such as a single leg squat or gait8. Applying ultrasound during dynamic movements has been shown to have acceptable to excellent reliability12. This technique can be applied to measure thickness changes in the lateral abdominal wall during a golf swing or other sport-specific task. While surface electromyography is commonly used to measure the electrical activity of muscles, this is less feasible in the abdominal region. The layered anatomy leads to cross-talk between the muscles and does not allow for a visual representation of the individual muscle layers of the core13. Ultrasound provides an advantage over alternatives like surface electromyography for the core musculature because it allows for a representation of each individual muscle while also giving an image for feedback14.
Since ultrasound provides an image of the muscles of interest in real time, it can also be used as a tool for visual biofeedback. Ultrasound biofeedback has improved the ability to increase the muscle thickness of the transverse abdominis and lumbar multifidus compared to verbal cueing alone15,16. Additionally, in golfers with and without low back pain, real-time ultrasound biofeedback increases transverse abdominis thickness in supine and in the golf-setup position11. Biofeedback training in supine also translates to upright loaded tasks17. More research is needed to determine the required frequency and duration of biofeedback training, as most studies are single-session or short-term training protocols15. Since ultrasound has been applied during functional tasks and there is evidence that golfers can increase deep muscle pre-activation in the setup position, research should next investigate the use of ultrasound biofeedback to increase oblique muscle thickness during the golf swing.
Therefore, this methodology aims to use ultrasound as a feedback mechanism to improve the activation and timing of the abdominal obliques during the golf swing.
Protocol
The present protocol was part of a study approved by the Institutional Review Board at the University of Central Florida. Informed consent was received from all human participants for the present study. To be included in the study, participants had to be between 18 years and 75 years of age, play golf at least once per month for the past year or once per week for the past 2 months, have played golf for at least 2 years, and have had at least two episodes of low back pain in the past 12 months. The exclusion criteria were balance disorders, current pregnancy, surgery to the low back or lower extremities in the past year, or an open wound in the abdominal area where the transducer must be placed.
1. Ultrasound setup and data collection
- Open and turn on the ultrasound device (see Table of Materials) using the On/Off button.
- Press the Patient button on the keyboard to add a new patient and select New Patient on the left side of the screen.
- Enter the desired patient ID number, ensure MSK is selected as the exam type, and click on Register. Exit to begin the exam and enter B-mode.
NOTE: Ultrasound settings in MSK Abdominal Preset, B-mode: B color = Tint Map D, Write Zoom Height = 4, Write Zoom Width = 4, Thermal Index = Tls, ATO Level = Low, Focus Number = 2, Focus Number CrossXBeam = 2, Focus Depth = 50, Depth (cm) = 3, Compression = 1, Focus Width = 1, Focus Width CrossXBeam = 1, Line Density = 3, Line Density CrossXBeam = 3, Suppression = 0, Frame Average = 4, From Average CrossXBeam = 2, CrossXBeam 2, CrossXBeam # = Low, CrossXBeam Type = Mean, Edge Enhance = 3, B Steer = 0, Gray Scale Map = Gray Map C, Gain = 34, Dynamic Range = 69, Rejection = 0, Frequency (MHz) = 12.
- Enter the desired patient ID number, ensure MSK is selected as the exam type, and click on Register. Exit to begin the exam and enter B-mode.
- Position the linear array transducer in the elastic belt by placing the head of the linear transducer through a horizontal slit in the middle of the belt (see Table of Materials). Next, apply one to two foam blocks to secure the transducer in its place.
- Apply ultrasound gel (see Table of Materials) to the linear transducer. Position the transducer on the lateral abdominal wall, approximately 10 cm lateral to the umbilicus8.
- Secure the belt to the participant using the hook and loop fasteners. Ensure the belt is tight enough so that the transducer is secured perpendicular to the lateral abdominal wall8.
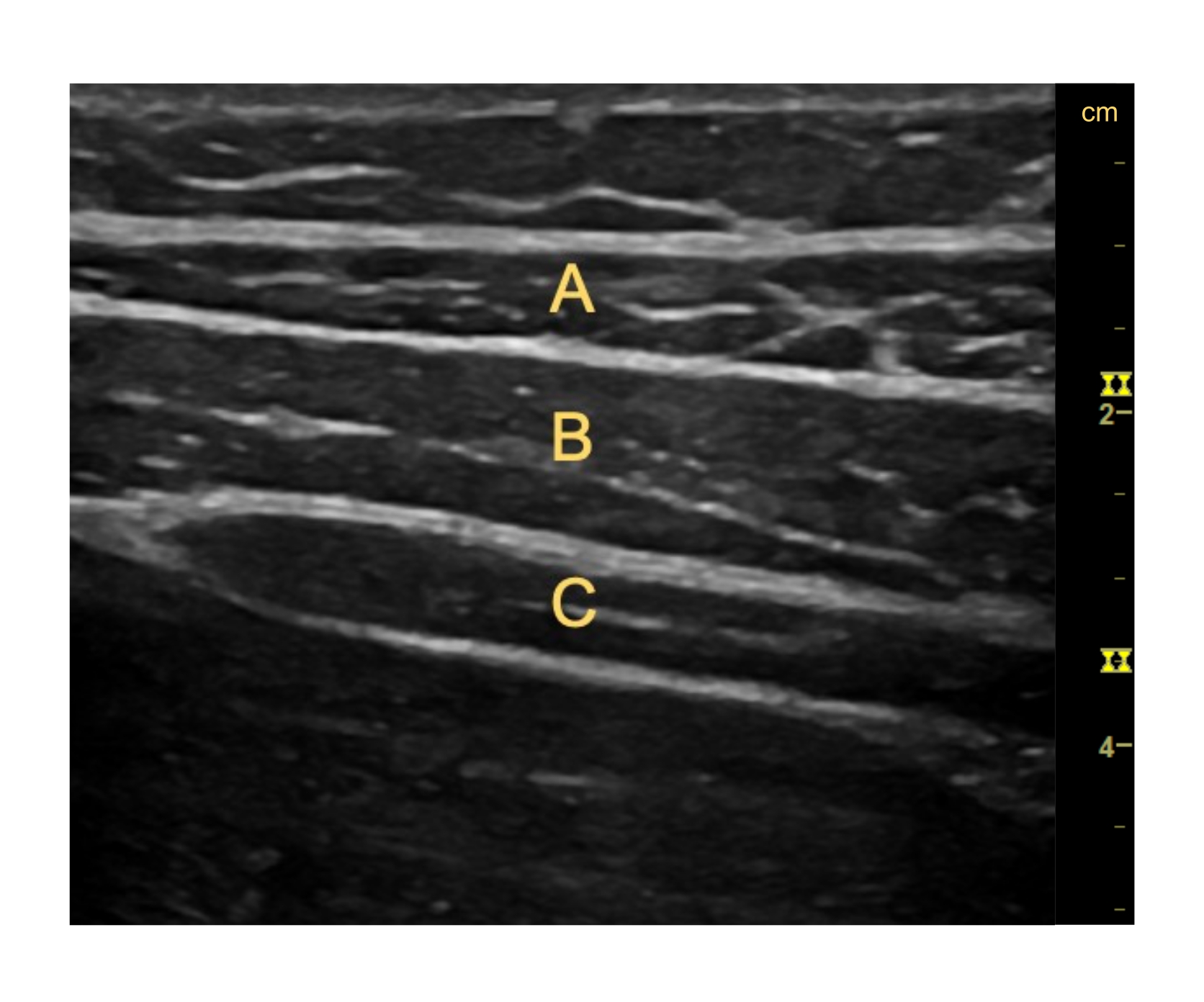
- Adjust the depth and gain (brightness) of the ultrasound if necessary to obtain a clear image of the fascial borders and muscle thickness of the external oblique, internal oblique, and transverse abdominis. Ensure that the fascial border of the transverse abdominis is visible on the edge of the screen in this longitudinal view (Figure 1)8.
NOTE: The depth will depend on the size of the individual being measured, but ensure that the deep fascial border of the transverse abdominis is visible and the image is clear. - Once the image is clear, position the patient in a manner that mirrors the task they will complete. For example, if they perform a golf swing, have them stand in their setup position. Press Freeze, then Store to capture a static image, save it to the patient's exam, and measure in real time or access it later to measure the resting muscle thickness.
NOTE: See Figure 1 for an example of a clear image of the lateral abdominal wall using B-mode ultrasound.
- Select Freeze again to return to live imaging. Press Store to begin recording in B-mode video. On the bottom-right corner of the screen, check that a timer begins and is highlighted in bright green, indicating that a video is being captured. Instruct the participant to take a full golf swing once the recording has begun.
- Press Store again to end the video and save it to their exam.
NOTE: Saved images and videos will appear below the active image, with up to five visible per row. Select the cursor to scroll through or select previous images.
- Press Store again to end the video and save it to their exam.
- Repeat step 1.4 as many times as necessary for the study. Adjust the positioning of the ultrasound probe within the foam block as needed if the image becomes blurry.
NOTE: Typical protocols comparing biofeedback and non-biofeedback conditions use between 3 and 10 repetitions per condition11,17.- After each trial, review the video for image clarity. If the image becomes anechoic (entirely black) at any point, it indicates that the ultrasound probe moved during the swing. In such a case, exclude the trial and re-measure.
- Following each swing, have the patient positioned where they can view the ultrasound screen. Open the most recent trial.
- Provide a brief overview and description of the muscles of interest (for a rotational task, this will include the external and internal obliques). Describe how the muscles should get thicker during the movement and show them their trial, providing education based on each attempt.
- For example, if the obliques stay relatively the same size throughout the task, instruct them to focus during the next attempt to contract their core muscles forcefully throughout the movement instead of passively rotating the trunk.
NOTE: Emphasis on trunk rotation as a power source during a golf swing is a common trait of higher-skilled golfers18. During rotational movements, it is generally not feasible to provide biofeedback during the task. Therefore, providing feedback following each trial is thought to be acceptable19.
- Repeat the biofeedback trials for as many attempts as desired. Provide the ultrasound images as well as verbal cueing or instruction following each attempt, adjusting the cueing as needed.

Figure 1: Image of the right lateral abdominal wall during quiet standing. (A) External oblique. (B) Internal oblique. (C) Transverse abdominis. Please click here to view a larger version of this figure.
{kind=link}
2. Resting image processing
- Open the first resting image to measure. Using the cursor, hover over the desired image from the library below the active image and click on Enter.
- Click on Measure once to open the measurement tool. Click on Enter when the cursor is over the superior fascial border of the muscle of interest.
NOTE: For the present study, the external and internal obliques were measured as they are the muscles of interest, but one can also measure the transverse abdominis in this view. - Click on Enter again once the cursor is over the inferior fascial border.
NOTE: The length of the measured segment will appear on the bottom-left portion of the screen, measured in centimeters. Record this length in a spreadsheet organized to include the participant or patient name/number and resting muscle thickness.
- Click on Measure once to open the measurement tool. Click on Enter when the cursor is over the superior fascial border of the muscle of interest.
- Repeat steps 2.1.1-2.1.2 for all the images needed to measure for both the external and internal obliques.
3. B-Mode video processing
- Once the desired number of videos have been captured, open the first video to be processed. Using the cursor, hover over the desired image from the library below the active image and click on the Enter button.
- Adjust the viewing frame within the B-mode video until the first frame is reached. Determine the desired sampling rate.
NOTE: Previous literature has used 10% intervals of the total frames from 0%-100% for analysis, but one may wish to use more or less depending on the aims20. - Once there is the desired frame open, use the Measure tool. Click the button once to open the tool, place the cursor on the superior fascial border of the muscle of interest, and click on Enter to place the first end of the measurement.
- Drag the measurement line to the inferior fascial border of the muscle of interest and click on Enter again to complete the measurement.
NOTE: The distance measured will appear on the bottom-left portion of the screen. - Press Store to save the measured image.
- Record the measurement in a spreadsheet organized to include participant or patient name/number, frame number, and thickness measurements. Return to the original B-mode video frame (step 3.2).
- Scroll to the next frame to be analyzed. For example, if one is sampling 11 time points (10% intervals from 0%-100%) of a swing that captured 100 frames, one will now use frame 10 (i.e., 10/100 corresponds to frame 10 out of 100 total frames).
- Repeat steps 3.3-3.4 to measure the next frame.
- Repeat step 3.7 until all the desired frames are measured.
- Move to the next video and repeat steps 3.1-3.8 until all the videos are measured.
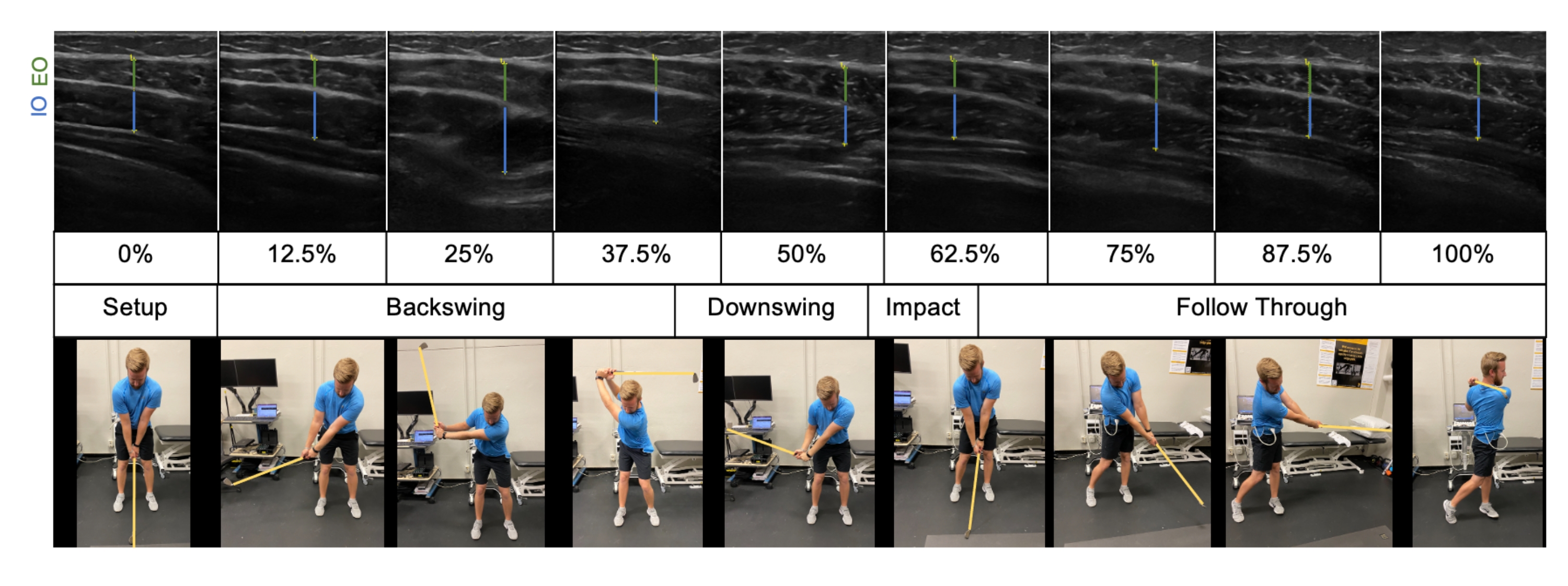
NOTE: See Figure 2 for a compilation of the processed frames throughout phases of a golf swing.
4. Activation ratio calculation
NOTE: An activation ratio is commonly used to determine the degree of muscle thickness change8,9,11. The formula for the activation ratio is contracted thickness (cm)/resting thickness (cm).
- To determine the activation ratio at a specific time point, measure the thickness by following step 3. Divide this value by the resting image thickness obtained from step 2.

Figure 2: Frame-by-frame analysis of a B-mode video on the trail side (right) lateral abdominal wall of a right-handed golfer. EO = external oblique; IO = internal oblique. Please click here to view a larger version of this figure.
{kind=link}
Results
| Non-feedback | Biofeedback | |||||
| Swing Duration | External Oblique Thickness (cm) | Internal Oblique Thickness (cm) | Combined Oblique Thickness (cm) | External Oblique Thickness (cm) |
Discussion
Providing ultrasound biofeedback following a rotation-based sports movement such as a golf swing can be used to increase the muscle thickness of the lateral abdominal wall. As shown in the representative results, a single trial of ultrasound biofeedback can lead to short-term increases in oblique muscle activity throughout a golf swing.
Previous research has also used B-mode ultrasound secured with an elastic belt during dynamic tasks20. This was measured while individu...
Disclosures
The authors have no relevant disclosures to report.
Acknowledgements
None.
Materials
| Name | Company | Catalog Number | Comments |
| Aquasonic 100 | Parker | BT-025-0037L | Ultrasound gel |
| GE NextGen Logig e Ultrasound Unit | GE Healthcare | HR48382AR | |
| Linear Array Probe | GE Healthcare | H48062AB | |
| Velcro straps | VELCRO | Fasteners for the elastic belt used to secure the ultrasound transducer |
References
- Betts, J. G., et al. . Anatomy and Physiology. , (2017).
- Saeterbakken, A. H., vanden Tillaar, R., Seiler, S. Effect of core stability training on throwing velocity in female handball players. Journal of Strength and Conditioning Research. 25 (3), 712-718 (2011).
- Pink, M., Perry, J., Jobe, F. W. Electromyographic analysis of the trunk in golfers. The American Journal of Sports Medicine. 21 (3), 385-388 (1993).
- Cole, M. H., Grimshaw, P. N. The biomechanics of the modern golf swing: Implications for lower back injuries. Sports Medicine. 46 (3), 339-351 (2016).
- McHardy, A. J., Pollard, H. P., Luo, K. Golf-related lower back injuries: An epidemiological survey. Journal of Chiropractic Medicine. 6 (1), 20-26 (2007).
- Horton, J. F., Lindsay, D. M., Macintosh, B. R. Abdominal muscle activation of elite male golfers with chronic low back pain. Medicine and Science in Sports and Exercise. 33 (10), 1647-1654 (2001).
- Cole, M. H., Grimshaw, P. N. Trunk muscle onset and cessation in golfers with and without low back pain. Journal of Biomechanics. 41 (13), 2829-2833 (2008).
- Mangum, L. C., Henderson, K., Murray, K. P., Saliba, S. A. Ultrasound assessment of the transverse abdominis during functional movement. Journal of Ultrasound in Medicine. 37 (5), 1225-1231 (2018).
- Sutherlin, M. A., et al. Changes in muscle thickness across positions on ultrasound imaging in participants with or without a history of low back pain. Journal of Athletic Training. 53 (6), 553-559 (2018).
- Teyhen, D. S., et al. The use of ultrasound imaging of the abdominal drawing-in maneuver in subjects with low back pain. Journal of Orthopaedic & Sports Physical Therapy. 35 (6), 346-355 (2005).
- Skibski, A., Burkholder, E., Goetschius, J. Transverse abdominis activity and ultrasound biofeedback in college golfers with and without low back pain. Physical Therapy in Sport. 46, 249-253 (2020).
- Mangum, L. C., Sutherlin, M. A., Saliba, S. A., Hart, J. M. Reliability of ultrasound imaging measures of transverse abdominis and lumbar multifidus in various positions. PM&R. 8 (4), 340-347 (2016).
- Stokes, I. A. F., Henry, S. M., Single, R. M. Surface EMG electrodes do not accurately record from lumbar multifidus muscles. Clinical Biomechanics. 18 (1), 9-13 (2003).
- Valera-Calero, J. A., et al. Ultrasound imaging as a visual biofeedback tool in rehabilitation: an updated systematic review. International Journal of Environmental Research and Public Health. 18 (14), 7554 (2021).
- Cha, H. -. G., Kim, M. -. K., Shin, Y. -. J. The effects of visual biofeedback using ultrasonograpy on deep trunk muscle activation. Journal of Physical Therapy Science. 28 (12), 3310-3312 (2016).
- Van, K., Hides, J. A., Richardson, C. A. The use of real-time ultrasound imaging for biofeedback of lumbar multifidus muscle contraction in healthy subjects. The Journal of Orthopaedic and Sports Physical Therapy. 36 (12), 920-925 (2006).
- McPherson, S. L., Watson, T. Training of transversus abdominis activation in the supine position with ultrasound biofeedback translated to increased transversus abdominis activation during upright loaded functional tasks. PM&R. 6 (7), 612-623 (2014).
- Burden, A. M., Grimshaw, P. N., Wallace, E. S. Hip and shoulder rotations during the golf swing of sub-10 handicap players. Journal of Sports Sciences. 16 (2), 165-176 (1998).
- Magill, R. A., Anderson, D. . Motor Learning and Control: Concepts and Applications. , (2014).
- DeJong, A. F., Mangum, L. C., Hertel, J. Gluteus medius activity during gait is altered in individuals with chronic ankle instability: An ultrasound imaging study. Gait & Posture. 71, 7-13 (2019).
- Hume, P. A., Keogh, J., Reid, D. The role of biomechanics in maximising distance and accuracy of golf shots. Sports Medicine. 35 (5), 429-449 (2005).
- Smith, J., Finnoff, J. T. Diagnostic and interventional musculoskeletal ultrasound: Part 1. fundamentals. PM&R. 1 (1), 64-75 (2009).
- Smith, J., Finnoff, J. T. Diagnostic and interventional musculoskeletal ultrasound: Part 2. clinical applications. PM&R. 1 (2), 162-177 (2009).
- Ribeiro, D. C., Mącznik, A. K., Milosavljevic, S., Abbott, J. H. Effectiveness of extrinsic feedback for management of non-specific low back pain: A systematic review protocol. BMJ Open. 8 (5), 021259 (2018).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionExplore More Articles
This article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved