
Method Article
Targeted Muscle Reinnervation: Surgical Protocol for a Randomized Controlled Trial in Postamputation Pain
In This Article
Summary
The protocol outlines the surgical procedure for the treatment of postamputation pain using Targeted Muscle Reinnervation (TMR). TMR will be compared with two other surgical techniques, specifically Regenerative Peripheral Nerve Interface (RPNI) and neuroma excision, followed by immediate burying within muscle under the context of an international, randomized controlled trial.
Abstract
Over the past decade, the field of prosthetics has witnessed significant progress, particularly in the development of surgical techniques to enhance the functionality of prosthetic limbs. Notably, novel surgical interventions have had an additional positive outcome, as individuals with amputations have reported neuropathic pain relief after undergoing such procedures. Subsequently, surgical techniques have gained increased prominence in the treatment of postamputation pain, including one such surgical advancement - targeted muscle reinnervation (TMR). TMR involves a surgical approach that reroutes severed nerves as a type of nerve transfer to "target" motor nerves and their accompanying motor end plates within nearby muscles. This technique originally aimed to create new myoelectric sites for amplified electromyography (EMG) signals to enhance prosthetic intuitive control. Subsequent work showed that TMR also could prevent the formation of painful neuromas as well as reduce postamputation neuropathic pain (e.g., Residual and Phantom Limb Pain). Indeed, multiple studies have demonstrated TMR's effectiveness in mitigating postamputation pain as well as improving prosthetic functional outcomes. However, technical variations in the procedure have been identified as it is adopted by clinics worldwide. The purpose of this article is to provide a detailed step-by-step description of the TMR procedure, serving as the foundation for an international, randomized controlled trial (ClinicalTrials.gov, NCT05009394), including nine clinics in seven countries. In this trial, TMR and two other surgical techniques for managing postamputation pain will be evaluated.
Introduction
Chronic neuropathic postamputation pain after a major limb amputation is, unfortunately, a common occurrence. This issue represents a complex and multifaceted challenge, significantly impacting the quality of life for individuals suffering from limb loss. Postamputation pain encompasses a broad spectrum of discomforting sensations, categorized as either pain perceived in the remaining limb, known as residual limb pain (RLP), or pain experienced in the absent extremity, referred to as phantom limb pain (PLP)1. The origins of RLP are diverse, arising from various factors such as inflammation, infection, neuromas, heterotopic ossification, bursae, complex regional pain syndrome, and anomalies in muscles and bones2. On the other hand, the precise roots of PLP remain only partially understood, with its neurogenesis believed to involve a complex interplay between peripheral and central nervous system influences3,4.
In cases of peripheral nerve injury, the nerve typically initiates a process of regeneration, aiming to re-establish connections with its target organs5. However, in the context of amputation, where the target organs are lost, an atypical phenomenon occurs where the axons sprout abnormally into the surrounding scar tissue, giving rise to what is known as a neuroma. Damaged nociceptive fibers within the neuroma exhibit a reduced activation threshold, causing them to transmit action potentials even in the absence of external stimuli6. Additionally, neuromas release inflammatory cytokines, which are linked to modifications in the processing of pain signals within the somatosensory cortex. This can result in unfavorable adjustments within the central nervous system, perpetuating and intensifying the pain response7,8. Complex and bidirectional interactions exist between the peripheral and central nervous systems, playing a pivotal role in the development of chronic pain. For instance, individuals with persistent peripheral neuropathy may undergo central sensitization, leading to altered processing of new sensory input, in contrast to individuals without a history of chronic pain9. Neuromas emerge as a contributor among the various sources of both RLP and PLP. Consequently, directing attention toward effective painful neuroma management represents a pivotal measure in reducing the occurrence and prevalence of postamputation neuropathic pain.
Historically, managing neuroma-induced pain has been a challenging endeavor. Traditional treatments have included various medications, physical therapy, and surgical interventions, each with its own set of limitations and variable outcomes. These conventional methods, while helpful to some extent, have not always provided consistent relief from postamputation pain10,11. Today, surgical interventions are one of the most common treatment strategies. These surgical approaches can generally be classified as non-reconstructive or reconstructive. Non-reconstructive approaches have often involved neuroma excision without the intention of allowing the severed nerve to re-establish connections with a physiologically appropriate target12. In contrast, reconstructive interventions are specifically designed to foster a "healthy" and natural regeneration of nerves following neuroma removal with the goal of providing terminal nerve receptors able to receive regenerating axonal growth cones13.
Various non-reconstructive techniques include procedures like nerve implantation into nearby tissues, nerve capping, the application of proximal pressure, or controlled thermal procedures on the distal nerve end12,14. Among these, one of the most utilized treatments entails excising the neuroma and transposing it into adjacent tissues like muscle, bone, or veins15. However, it is essential to consider neurophysiology principles, which indicate that freshly transected peripheral nerves will undergo axonal sprouting and elongation. This process can lead to the recurrence of the painful neuroma as the regenerating axons lack appropriate targets for reinnervation16. The outcomes of this technique have been diverse, with some patients experiencing no pain relief, while others report gradual or complete pain alleviation. Conversely, there are cases where patients initially experience pain relief after surgery but subsequently develop neuropathic pain again over time15,17. Nevertheless, even if this technique has shown limited success in pain alleviation, neuroma transposition with implantation into muscle tissue continues to be widely practiced in amputation care. It has traditionally, to a significant extent, been regarded as the "gold standard" for surgical treatments of painful terminal neuromas10,12.
Nevertheless, the landscape of pain management is continually evolving, with an increasing focus on proactive strategies to optimize the treatment of nerve endings following neuroma removal. The primary objective is to create a favorable environment for the nerve endings, fostering a more natural and satisfactory process of neuronal regeneration12. One such approach is Targeted Muscle Reinnervation (TMR). The TMR procedure was developed in the early 2000's by Dr. Todd Kuiken and Dr. Gregory Dumanian in Chicago, USA. TMR is a surgical technique that involves rerouting nerves through a formal nerve transfer procedure to "target" motor nerves and accompanying motor end plates supplying nearby muscle18. The primary purpose behind the development of this technique was to enhance the intuitive control of prosthetic limbs19,20,21,22. As a secondary and noteworthy benefit, patients who underwent TMR reported an improvement in their pain23. The TMR procedure has been adopted by numerous clinics worldwide and has become one of the standard practices in the field of amputation care. However, disparities among the TMR protocol have been reported24. Therefore, we put forth a unified consensus of the technique in this article, which includes some of the most active surgeons on this procedure worldwide.
Here, we provide a complete step-by-step protocol for the TMR procedure, which is used in a randomized controlled trial (RCT) (ClinicalTrials.gov as NCT05009394). The primary objective of the international RCT is to evaluate the efficacy of treating postamputation pain with two widely employed reconstructive techniques, namely TMR and the Regenerative Peripheral Nerve Interface (RPNI)25,26,27, in comparison to a commonly practiced and standard surgical treatment28. The primary objective of this methodological article is to present the standardized protocol of TMR for the international RCT and make it accessible to all those interested in incorporating it into the care of individuals with amputations.
Protocol
The RCT was approved in Sweden by the Swedish Ethics Review Authority, Etikprövningsmyndigheten, on 30 June 2021 with the application number 2021-0234628. Further details on the RCT are outlined in protocol28. The Ethical Committee in the Region of Emilia Romagna in Italy approved the participation of the human subject in the surgery. Written consent was obtained from the participant.
NOTE: The important terminologies to be noted are:
Donor nerve: a nerve with a painful neuroma to be transferred to a recipient residual or "target" nerve.
Recipient residual nerve: the transected segment of a nerve (freshly prepared nerve stump) natively innervating a target muscle.
Target muscle: a viable muscle supplied by the recipient residual or "target" motor nerve in or near the residual limb.
1. Presurgical preparations
- Diagnose the painful neuroma(s) following the international RCT protocol28.
- Conduct a thorough physical assessment to detect potential muscle targets and evaluate the flexibility of the soft tissue surrounding the nerve. Perform an EMG evaluation of those target muscles in case muscle contraction is hardly assessable.
- Plan the skin incisions depending on the results from steps 1.1-1.2.
- Dilute the epinephrine solution (1:500,000), which may be used before incisions to reduce intra-operative bleeding.
2. Preparation of the donor nerve
- Perform either regional or general anesthesia without the use of muscle relaxants to allow for effective nerve stimulation.
NOTE: The type of anesthesia depends on the site of the procedure. - Depending on the site of the painful neuroma, place the patient in a supine or prone position. For painful neuromas present in the upper extremity, use a surgical arm board to place the arm.
- Carry out the skin incision using a scalpel. The length and shape of the skin incision depend on the location of the painful neuroma.
- Identify the donor nerve under blunt dissection.
- Gently isolate the donor nerve and the neuroma under loupe magnification using microsurgical instruments as needed.
NOTE: Isolation of the neuroma is optional. - Mobilize the donor nerve for as long as necessary to reach the recipient site, considering that the following nerve sutures are free of tension in all range of motions in the proximal joints. Transect the neuroma using a commercial nerve cutting/preparation set.
NOTE: Resection of the neuroma is optional when challenging. - Repeat steps 2.4-2.6 for each nerve with an identified painful neuroma in the current exposed area.
3. Motor point identification
- Identify all motor nerve branches to the target muscle by blunt dissection.
- Set the hand-held-nerve stimulator at 0.5-1.0 mA, put it in contact with the nerve branches, and stimulate each of them. During stimulation, the nerve that provides the largest muscle contraction is the one that will be used as the recipient nerve. In Table 1, target muscles are suggested for each nerve at a specific amputation level.
- Use the known proximal innervation points as the targets when possible.
- Denervate the target muscle completely when possible.
- Once active contraction is confirmed, transect the nerve using straight microscissors without tension as close as possible to its entry point. Aim for less than 1 cm.
- Transpose the proximal stump of the transected donor nerve proximally away from the coaptation site without any specific management.
Table 1: Suggested target muscle(s) for each donor nerve. Please click here to download this Table.
4. Nerve-to-nerve coaptation
- Suture the donor nerve to the recipient residual or "target" motor nerve with an 8-0 non-resorbable monofilament suture, placing the stitch in the center of the donor nerve.
NOTE: Each donor nerve is larger in caliber with more fascicles than the recipient motor nerve. Significant mismatch is usually encountered. - Reinforce with two or three 8-0 non-resorbable monofilament sutures that secure the donor nerve epineurium to the fascia and epimysium that surrounds the recipient nerve. Ensure that the coaptation is performed with neither tension nor excessive redundancy.
- Close the surgical wounds in layers.

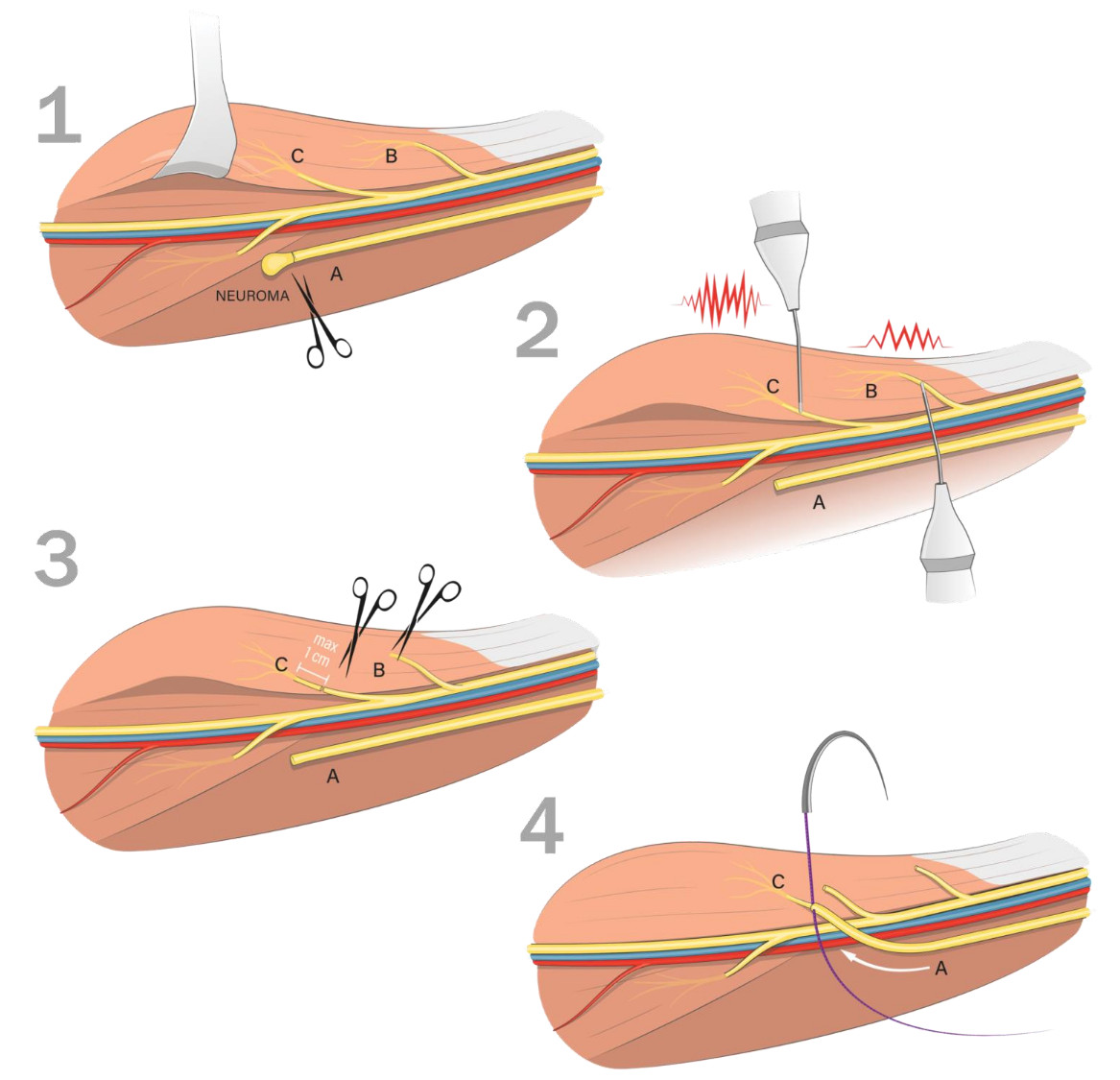
Figure 1: Flowchart of the Targeted Muscle Reinnervation (TMR) technique. 1) Identify and isolate the donor nerve with the painful neuroma (A). Mobilize the donor nerve and transect the neuroma up to healthy neural fascicles; 2) Identify motor nerve(s) to the target muscle and confirm muscle contraction using a hand-held nerve stimulator; 3) If several motor branches are identified, choose the motor branch that results in the largest contraction (C). Transect the nervewithout tension as close as possible to its entry point (maximum 1 cm). Dennervate other identified motor branches to the same muscle when possible (B); 4) Suture the prepared donor nerve to the recipient residual or "target" nerve with the stitch placed in the center of the donor nerve. Reinforce with two or three microsutures that secure the donor nerve epineurium to the fascia and epimysium that surrounds the recipient nerve. Please click here to view a larger version of this figure.
{kind=link}
Results
Over the past decade, the TMR procedure has gained significant traction in managing neuroma-related pain. Initially, this technique found its primary application in upper limb amputations, particularly in cases involving transhumeral and shoulder disarticulation amputations23,29. However, in recent years, TMR has seen expanded use and development in transfemoral, transradial, and hand and digit amputations30,31,32,33,34. The initial report of TMR as a treatment for pain was in 2014 by Souza et al. In this article, the authors present retrospective data of the effect of TMR for treating RLP in 26 patients with an upper extremity amputation between 2002 and 201223. All patients were treated with TMR for the primary purpose of improved myoelectric control, and 15 patients had documented postamputation pain before the TMR treatment. The patients were followed at least 6 months after surgery, and 14 of the patients experienced complete pain resolution, and 1 had improvement in the pain. None of the patients who did not experience neuroma pain before TMR developed painful neuromas after the treatment23.
Subsequently, in 2019, Dumanian et al. conducted a single-blinded RCT comparing the outcomes of TMR to an active control that underwent neuroma excision and implantation into muscle tissue, similar to our RCT28 (Table 2). The study included twenty-eight participants with either upper or lower limb amputations who were tracked for 1 year post-surgery. The change in the numerical rating score (NRS) for RLP before and after TMR yielded positive results for the TMR group, although these differences did not reach statistical significance (p > 0.05). Similarly, no statistical significant differences were observed in the change in NRS for PLP between TMR and control groups35. Furthermore, patients who did not meet the inclusion criteria and were declined to participate in the RCT, were enrolled in a prospective study where all the study participants received the TMR treatment. Thirty-three patients were followed up one year after TMR and were included in the analyses. NRS scores for RLP decreased from an initial value of 6.4 (±2.6) to 3.6 (±2.2), reflecting a mean difference of -2.7 (95% CI -4.2 to -1.3; p < 0.001) 1-year post TMR. Additionally, phantom limb pain decreased from an initial score of 6.0 (±3.1) to 3.6 (±2.9), with a mean difference of -2.4 (95% CI -3.8 to -0.9; p < 0.001)36.
Table 2: Studies investigating the effect of targeted muscle reinnervation (TMR) as a treatment for postamputation pain in secondary amputations. High values of RLP, NP, and PLP reduction indicate higher efficacy of TMR as a treatment of postamputation pain. Please click here to download this Table.
TMR has also found utility when employed at the time of primary amputation, serving as a preventive measure against the development of painful neuromas (Table 3). One of the first documented cases of this approach dates to 2014 when Cheesborough et al. conducted TMR just one week after the traumatic amputation of an upper limb. The patient reported a complete absence of neuroma-related pain and exhibited minimal pain-related behaviors or interference 8 months post-TMR, as assessed through the Patient Reported Outcomes Measurement Information System (PROMIS)37. Later, Valerio et al. conducted a retrospective study where 51 patients who received TMR at primary amputation were compared to a control group with 438 unselected major limb amputations. Patients in the TMR group reported significantly less RLP and PLP compared to the control group (NRS), and the TMR group also reported lower median PROMIS t-scores38. Similar results in the prevention of RLP and PLP have been reported by other retrospective studies39,40.
Table 3: Studies examining targeted muscle reinnervation (TMR) as a prophylactic treatment for the prevention of postamputation pain at the time of primary amputation. Low percentage values of RLP, NP, and PLP incidence indicate higher efficacy of TMR as a prevention treatment. Please click here to download this Table.
In recent years, several researchers have incorporated the TMR procedure into their clinics for both treatment and prophylactic purposes. They have shared their data and experience of the procedure for pain management39,40,41,42,43,44,45,46. The majority of these studies are of a retrospective nature; however, they all report favorable outcomes of using the TMR procedure. Notably, the procedure has shown to be effective in pain relief for patients with multiple comorbidities40, patients with longstanding amputation42, and in children44,45. Surgical complications associated with TMR have not shown a higher risk when compared to standard techniques35. On the contrary, the literature demonstrates a significant reduction in complications when TMR is performed, including stump wounds and infections requiring operative debridement and revision40.
Discussion
TMR is a contemporary procedure in amputation care used to improve myoelectric control of a prosthesis and has proven to have a beneficial effect in reducing and preventing postamputation neuropathic pain. The TMR procedure distinguishes itself fundamentally from alternative non-reconstructive methods for managing neuromas by its core objective, the reconnection of the severed nerve to a physiologically appropriate target that supports nerve regeneration and reinnervation of an end organ. Moreover, a significant contrast arises between TMR and techniques like neuroma transposition and muscle implantation, where the donor nerve's end organ of the muscle is appropriate but remains innervated by its native nerve. Thus, it does not support nerve regeneration or reinnervation of the target muscle via its motor nerve. When the muscle is already innervated, native nerve fibers occupy muscle fibers, creating a challenge for the freshly cut donor nerve to establish a connection with the new host muscle. This situation could potentially result in the formation of a new terminal symptomatic neuroma. Additionally, when comparing TMR to RPNI surgery, where both techniques entail the use of a denervated target muscle, a substantial distinction comes into play. In TMR, the freshly cut nerve end is coapted to a nearby expendable motor nerve, ensuring reinnervation of a vascularized muscle. Conversely, in RPNI, a non-vascularized, denervated muscle graft is employed, highlighting a difference between the two procedures. Moreover, the TMR surgery entails sacrificing healthy innervations which might result in new symptomatic neuromas, albeit this is rarely reported in the literature. Another difference is the sizable mismatch between donor and recipient nerves, which could theoretically result in a neuroma-in-continuity, which is also rarely reported. Furthermore, the TMR procedure involves a series of intricate stages, encompassing nerve-to-nerve coaptation, and identification of motor branches to a muscle, potentially restricting the applicability of the procedure in common amputations. Ideally, this set of skills will be soon incorporated as part of the ongoing revolution on amputation procedures.
In cases focused solely on pain management, when multiple motor branches are present within the target muscle, there is no necessity for the selection of the motor branch with the strongest contraction. Our aim is to offer study participants in the RCT the opportunity to enhance their control over a myoelectric prosthesis when possible. This is why we suggest specific target muscle(s) for each nerve (Table 1). Furthermore, in scenarios where, for instance, painful neuromas are present in both the median and ulnar nerves at the transhumeral level, the biceps short-head muscle is recommended as the target for both nerves. If multiple innervation points are identified within the biceps, both the median and ulnar nerves can be coapted to different innervation points within the biceps muscle. While this may not be suitable for prosthetic control, it could be beneficial for pain management.
To reach successful outcomes of the TMR technique, one of the most important critical steps in the procedure is to ensure proper mobilization of the donor nerve stump to obtain tension free nerve sutures. Other critical steps for successful TMR include full denervation of the target muscle and usage of known proximal innervation points as the targets18. Furthermore, during the preparation of this protocol, a discussion regarding the surgical step "coaptation" was brought to the attention of the surgeons in the trial. The coaptation in the TMR technique could be performed in three different ways, including nerve-to-nerve coaptation with either short or long recipient nerve or nerve-to-neuromuscular entry zone (see Figure 2). In this RCT, we will prioritize nerve-to-nerve coaptation as described in the step-by-step protocol. Deviation from this technique will be documented during the trial.

Figure 2: Three different ways to perform TMR coaptation. (A) Nerve-to-nerve coaptation with long recipient residual nerve; (B) Nerve-to-nerve coaptation with short recipient residual nerve; (C) Nerve-to-neuromuscular entry zone coaptation. Please click here to view a larger version of this figure.
{kind=link}
It is important to note that the literature does not consistently demonstrate universal success with the TMR technique, and there have been instances of unsuccessful TMR surgeries. Felder et al. reported their experiences of technical challenges, including issues such as nerve redundancy, size mismatch, neuroma formation, the positioning of coaptation sites, full muscle denervation at the target site, and the selection of the optimal target for prosthetic functionality24. Alongside technical pitfalls, TMR procedures also necessitate a longer duration in the surgical theater compared to conventional techniques. Consequently, this extended surgical time results in higher overall expenses47. Moreover, failed TMRs might lead to muscle atrophy, resulting in a change in the residual limb and complicating prosthetic fitting. Furthermore, Felder et al. also highlight the considerable variability in surgical technique for TMR across different studies and among surgeons. They also emphasize that many reports lack the provision of sufficient technical details24. Discrepancies in the procedure were identified during the preliminary stages of this article's preparation, as the participating surgeons in the trial determined each step of the protocol. Consequently, the principal objective and driving force behind this methodological article is to establish a standardized protocol with comprehensive descriptions, thereby ensuring uniformity in the procedure across the trial.
As mentioned previously, the primary purpose behind the development of TMR was to enhance the control of myoelectric prostheses. This technique has undergone further development by incorporating sensory reinnervation of the skin, a variant known as Targeted Sensory Reinnervation (TSR). TSR has been instrumental in restoring sensation in the missing extremity48. When coupled with essential rehabilitation, the TMR procedure has significantly enhanced the control of myoelectric prostheses, often resulting in a significant increase of 2-3 degrees of freedom. Consequently, it has brought about a substantial improvement in the quality of life for many individuals living with limb amputations. Moreover, TMR has recently been employed in conjunction with RPNI, facilitating single-finger control for transhumeral amputee49, showcasing its potential to achieve remarkable outcomes in prosthetic functionality.
Disclosures
The authors have no disclosures.
Acknowledgements
The authors wish to express their gratitude to the funding organizations that supported this project: the Promobilia Foundation, the IngaBritt and Arne Lundbergs Foundation, and the Swedish Research Council (Vetenskapsrådet). Additionally, profound thanks are extended to those who graciously donated their bodies to science, enabling crucial anatomical research. The outcomes of such research hold the potential to enhance patient care and expand humanity's collective understanding. Therefore, sincere appreciation is owed to these donors and their families. The authors also wish to acknowledge the invaluable collaboration of Professors Lucia Manzoli and Stefano Ratti from the Anatomy Center, Alma Mater Studiorum-University of Bologna. Special thanks are also extended to Carlo Piovani and Mirka Buist for their contributions to creating the illustrations.
Materials
| Name | Company | Catalog Number | Comments |
| #15 Scalpel | Swann-Morton | 0205 | The company and the catalog number is one example. |
| 8-0 Ethilon suture | Ethicon | W2808 | The company and the catalog number is one example. |
| Hand-held nerve stimulator | Checkpoint Surgical | Model 9094 | The company and the catalog number is one example. |
| Loupes | Zeiss | Various | User can choose loupes according to personal preferences. |
| Nerve cutting set | Checkpoint Surgical | 9250 | The company and the catalog number is one example. |
| Straight microscissors | S&T® | SAS-12 R-7 | The company and the catalog number is one example. |
References
- Schug, S. A., Lavand, P., Barke, A., Korwisi, B., Rief, W. The IASP classification of chronic pain for ICD-11 chronic postsurgical or posttraumatic pain. Pain. 160 (1), 45-52 (2019).
- Davis, R. W. Phantom sensation, phantom pain, and stump pain. Arch Phys Med Rehabil. 74 (1), 79-91 (1993).
- Flor, H. Phantom-limb pain: Characteristics, causes, and treatment. Lancet Neurol. 1 (3), 182-189 (2002).
- Ortiz-Catalan, M. The stochastic entanglement and phantom motor execution hypotheses: A theoretical framework for the origin and treatment of Phantom limb pain. Front Neurol. 9, 748(2018).
- Lee, M., Guyuron, B. Postoperative Neuromas. Nerves and Nerve Injuries. , Elsevier, Academic Press. (2015).
- Curtin, C., Carroll, I. Cutaneous neuroma physiology and its relationship to chronic pain. J Hand Surg Am. 34 (7), 1334-1336 (2009).
- Khan, J., Noboru, N., Young, A., Thomas, D. Pro and anti-inflammatory cytokine levels (TNF-α, IL-1β, IL-6 and IL-10) in rat model of neuroma. Pathophysiology. 24 (3), 155-159 (2017).
- Clark, A. K., Old, E. A., Malcangio, M. Neuropathic pain and cytokines: current perspectives. J Pain Res. 6, 803(2013).
- Costigan, M., Scholz, J., Woolf, C. J. Neuropathic pain: A maladaptive response of the nervous system to damage. Annu Rev Neurosci. 32, 1-32 (2009).
- Eftekari, S. C., Nicksic, P. J., Seitz, A. J., Donnelly, D. T., Dingle, A. M., Poore, S. O. Management of symptomatic neuromas: a narrative review of the most common surgical treatment modalities in amputees. Plastic Aesthet Res. 9 (7), 43(2022).
- Chou, J., Liston, J. M., DeGeorge, B. R. Traditional neuroma management strategies. Ann Plastic Surg. 90 (6), S350-S355 (2023).
- Eberlin, K. R., Ducic, I. Surgical algorithm for neuroma management: A changing treatment paradigm. Plast Reconstr Surg Glob Open. 6 (10), e1952(2018).
- Langeveld, M., Hundepool, C. A., Duraku, L. S., Power, D. M., Rajaratnam, V., Zuidam, J. M. Surgical treatment of peripheral nerve neuromas: A systematic review and meta-analysis. Plast Reconstr Surg. 150 (4), 823-834 (2022).
- Ives, G. C., et al. Current state of the surgical treatment of terminal neuromas. Neurosurgery. 83 (3), 354-364 (2018).
- Dellon, A. L., Mackinnon, S. E. Treatment of the painful neuroma by neuroma resection and muscle implantation. Plast Reconstr Surg. 77, 427-438 (1986).
- Neumeister, M. W., Winters, J. N. Neuroma. Clin Plast Surg. 47 (2), 279-283 (2020).
- Guse, D. M., Moran, S. L. Outcomes of the surgical treatment of peripheral neuromas of the hand and forearm: A 25-year comparative outcome study. Ann Plastic Surg. 71 (6), 654-658 (2013).
- Eberlin, K. R., et al. A consensus approach for targeted muscle reinnervation in amputees. Plast Reconstr Surg Glob Open. 11 (4), e4928(2023).
- O'Shaughnessy, K. D., Dumanian, G. A., Lipschutz, R. D., Miller, L. A., Stubblefield, K., Kuiken, T. A. Targeted reinnervation to improve prosthesis control in transhumeral amputees: A report of three cases. J Bone Joint Surg. 90 (2), 393-400 (2008).
- Kuiken, T. A., et al. Targeted reinnervation for enhanced prosthetic arm function in a woman with a proximal amputation: a case study. Lancet. 369 (9559), 371-380 (2007).
- Kuiken, T., Dumanian, G., Lipschutz, R., Miller, L. A., Stubblefield, K. The use of targeted muscle reinnervation for improved myoelectric prosthesis control in a bilateral shoulder disarticulation amputee. Prosthet Orthot Int. 28 (3), 245-253 (2004).
- Hijjawi, J. B., Kuiken, T. A., Lipschutz, R. D., Miller, L. A., Stubblefield, K. A., Dumanian, G. A. Improved myoelectric prosthesis control accomplished using multiple nerve transfers. Plast Reconstr Surg. 118 (7), 1573-1578 (2006).
- Souza, J. M., Cheesborough, J. E., Ko, J. H., Cho, M. S., Kuiken, T. A., Dumanian, G. A. Targeted muscle reinnervation: A novel approach to postamputation neuroma pain. Clin Orthop Relat Res. 472 (10), 2984-2990 (2014).
- Felder, J. M., Pripotnev, S., Ducic, I., Skladman, R., Ha, A. Y., Pet, M. A. Failed targeted muscle reinnervation: Findings at revision surgery and concepts for success. Plast Reconstr Surg Glob Open. 10 (4), e4229(2022).
- Woo, S. L., Kung, T. A., Brown, D. L., Leonard, J. A., Kelly, B. M., Cederna, P. S. Regenerative peripheral nerve interfaces for the treatment of postamputation neuroma pain: A pilot study. Plast Reconstr Surg Glob Open. 4 (12), e1038(2016).
- Dean, R. A., Tsai, C., Chiarappa, F. E., Cederna, P. S., Kung, T. A., Reid, C. M. Regenerative peripheral nerve interface surgery: Anatomic and technical guide. Plast Reconstr Surg Glob Open. 11 (7), 5127(2023).
- Kubiak, C. A., Adidharma, W., Kung, T. A., Kemp, S. W. P., Cederna, P. S., Vemuri, C. Decreasing postamputation pain with the regenerative peripheral nerve interface (RPNI). Ann Vasc Surg. 79, 421-426 (2022).
- Pettersen, E., et al. Surgical treatments for postamputation pain study protocol for an international , double - blind , randomised controlled trial. Trials. 24 (1), 304(2023).
- Kuiken, T. A., Barlow, A. K., Feuser, A. E. S. Targeted Muscle Reinnervation. , Taylor & Francis Group, CRC Press. Boca Raton. (2013).
- Morgan, E. N., Potter, B. K., Souza, J. M., Tintle, S. M., Nanos, G. P. Targeted muscle reinnervation for transradial amputation: Description of operative technique. Tech Hand Up Extrem Surg. 20 (4), 166-171 (2016).
- Bowen, J. B., Ruter, D., Wee, C., West, J., Valerio, I. L. Targeted muscle reinnervation technique in below-knee amputation. Plast Reconstr Surg. 143 (1), 309-312 (2019).
- Fracol, M. E., Dumanian, G. A., Janes, L. E., Bai, J., Ko, J. H. Management of sural nerve neuromas with targeted muscle reinnervation. Plast Reconstr Surg Glob Open. 8 (1), 2545(2019).
- Fracol, M. E., Janes, L. E., Ko, J. H., Dumanian, G. A. Targeted muscle reinnervation in the lower leg: An anatomical study. Plast Reconstr Surg. 142 (4), 541-550 (2018).
- Daugherty, T. H. F., Bueno, R. A., Neumeister, M. W. Novel use of targeted muscle reinnervation in the hand for treatment of recurrent symptomatic neuromas following digit amputations. Plast Reconstr Surg Glob Open. 7 (8), e2376(2019).
- Dumanian, G. A., et al. Targeted muscle reinnervation treats neuroma and phantom pain in major limb amputees. Ann Surg. 270 (2), 238-246 (2019).
- Mioton, L. M., et al. Targeted muscle reinnervation improves residual limb pain, phantom limb pain, and limb function: A prospective study of 33 major limb amputees. Clin Orthop Relat Res. 478 (9), 2161-2167 (2020).
- Cheesborough, J. E., Souza, J. M., Dumanian, G. A., Bueno, R. A. Targeted muscle reinnervation in the initial management of traumatic upper extremity amputation injury. Hand. 9 (2), 253-257 (2014).
- Valerio, I. L., et al. Preemptive treatment of phantom and residual limb pain with targeted muscle reinnervation at the time of major limb amputation. J Ame Coll Surg. 228 (3), 217-226 (2019).
- O'Brien, A. L., Jordan, S. W., West, J. M., Mioton, L. M., Dumanian, G. A., Valerio, I. L. Targeted muscle reinnervation at the time of upper-extremity amputation for the treatment of pain severity and symptoms. J Hand Surg Am. 46 (1), 1-10 (2021).
- Chang, B. L., Mondshine, J., Attinger, C. E., Kleiber, G. M. Targeted muscle reinnervation improves pain and ambulation outcomes in highly comorbid amputees. Plast Reconstr Surg. 148 (2), 376-386 (2021).
- Vincitorio, F., et al. Targeted muscle reinnervation and osseointegration for pain relief and prosthetic arm control in a woman with bilateral proximal upper limb amputation. World Neurosurg. 143, 365-373 (2020).
- Michno, D. A., Woollard, A. C. S., Kang, N. V. Clinical outcomes of delayed targeted muscle reinnervation for neuroma pain reduction in longstanding amputees. J Plast Reconstr & Aesthet Surg. 72 (9), 1576-1606 (2019).
- Kang, N. V., Woollard, A., Michno, D. A., Al-Ajam, Y., Tan, J., Hansen, E. A consecutive series of targeted muscle reinnervation (TMR) cases for relief of neuroma and phantom limb pain: UK perspective. J Plast Reconstr Aesthet Surg. 75 (3), 960-969 (2021).
- Pires, G. R., Moss, W. D., Ormiston, L. D., Baschuk, C. M., Mendenhall, S. D. Targeted muscle reinnervation in children: A case report and brief overview of the literature. Plast Reconstr Surg Glob Open. 9 (12), e3986(2021).
- Bjorklund, K. A., et al. Targeted muscle reinnervation for limb amputation to avoid neuroma and phantom limb pain in patients treated at a pediatric hospital. Plast Reconstr Surg Glob Open. 11 (4), e4944(2023).
- Alexander, J. H., et al. Targeted muscle reinnervation in oncologic amputees: Early experience of a novel institutional protocol. J Surg Oncol. 120 (3), 348-358 (2019).
- Dellon, A. L., Aszmann, O. C. In musculus, veritas? Nerve "in muscle" versus targeted muscle reinnervation versus regenerative peripheral nerve interface: Historical review. Microsurgery. 40 (4), 516-522 (2020).
- Hebert, J. S., et al. Novel targeted sensory reinnervation technique to restore functional hand sensation after transhumeral amputation. IEEE Trans Neural Syst Rehabil Eng. 22 (4), 765-773 (2014).
- Zbinden, J., et al. Improved control of a prosthetic limb by surgically creating electro-neuromuscular constructs with implanted electrodes. Sci Transl Med. 15 (704), 3665(2023).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved