
A subscription to JoVE is required to view this content. Sign in or start your free trial.
Method Article
قياس النشاط الجبهي الحوفي باستخدام العاطفي غريب الاطوار العمل في الأطفال الذين يعانون من مخاطر عالية العائلي لمرض الفصام
In This Article
Summary
This paper describes how to use the emotional oddball task and fMRI to measure brain activation in children and adolescents at familial high risk for schizophrenia (FHR). FMRI was used to measure differences in fronto-striato-limbic regions during an emotional oddball task. Children with FHR exhibited abnormal functional activation during adolescence.
Abstract
Adolescence is a critical developmental period where the early symptoms of schizophrenia frequently emerge. First-degree relatives of people with schizophrenia who are at familial high risk (FHR) may show similar cognitive and emotional changes. However, the neurological changes underlying the emergence of these symptoms remain unclear. This study sought to identify differences in frontal, striatal, and limbic regions in children and adolescents with FHR using functional magnetic resonance imaging. Groups of 21 children and adolescents at FHR and 21 healthy controls completed an emotional oddball task that relied on selective attention and the suppression of task-irrelevant emotional information. The standard oddball task was modified to include aversive and neutral distractors in order to examine potential group differences in both emotional and executive processing. This task was designed specifically to allow for children and adolescents to complete by keeping the difficulty and emotional image content age-appropriate. Furthermore, we demonstrate a technique for suitable fMRI registration for children and adolescent participants. This paradigm may also be applied in future studies to measure changes in neural activity in other populations with hypothesized developmental changes in executive and emotional processing.
Introduction
Schizophrenia is a neurodevelopmental disorder with a known genetic component1,2 and with symptoms including deficits in both executive and emotional processing3,4. First-degree relatives are thought to be at an increased risk of developing schizophrenia, and have been shown to share some of these same neurocognitive deficits in both cognitive and social-emotional domains5. We therefore expect that brain activity in regions associated with executive and emotional processing may be altered in at-risk family members preceding the onset of clinical symptoms.
Previous studies have indicated that both adults with schizophrenia and adults at familial high risk show aberrant activity within executive and emotional processing networks; however it remains unclear how these changes come about during development. Demonstrating that these changes occur early in life will be a critical first step in understanding the pathophysiology of the disorder. Therefore, this study utilizes an emotional oddball paradigm during functional MRI (fMRI) scanning in order to measure brain activity during the completion of a task that requires both executive and emotional processing in adolescents who are at risk for developing schizophrenia. Oddball paradigms are frequently used to examine the function of fronto-striate circuitry in schizophrenia6 and in individuals with familial high risk7 by measuring selective attention processes allocated to task-relevant target stimuli. Here, a standard oddball task has been modified to include task-irrelevant aversive and neutral stimuli that have been shown to elicit changes in brain activity in patients with schizophrenia8.
This paper measures functional differences between healthy adolescents and adolescents at high familial risk for schizophrenia using an emotional oddball task. The task design is similar to that used by Fichtenholtz and colleagues9, but the selection of aversive emotional images has been modified to be appropriate for children between the ages of 9-18. The use of this task during functional MRI allowed for the identification of specific brain regions that showed patterns of hyperactivation and hypoactivation in children and adolescents with FHR for schizophrenia, in addition to age-related changes in neural activity during adolescent development.
Access restricted. Please log in or start a trial to view this content.
Protocol
تمت الموافقة على تقنيات البحث التي استخدمت خلال هذه الدراسة من قبل مجالس المراجعة المؤسسية (IRB) من جامعة ديوك وجامعة نورث كارولينا - تشابل هيل.
1. تصميم العمل التصوير
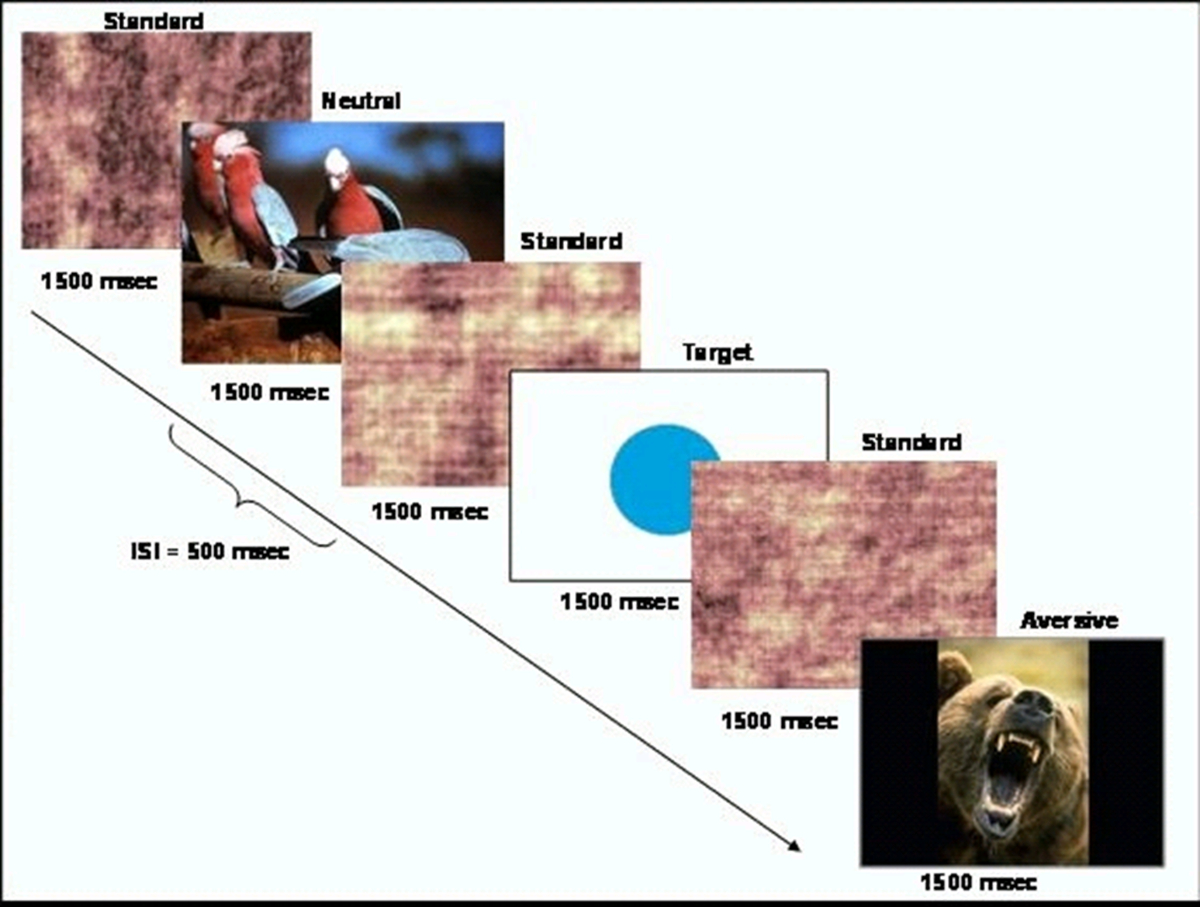
- توليد مهمة الحدث القائم السلوكية التي تقدم محفزات الهدف نادرة (دائرة) ضمن سلسلة من المحفزات مستوى أكثر تواترا (صور مشوشة). ويرد التخطيطي للمهمة في الشكل 1. تقديم المهمة باستخدام البرمجيات CIGAL 10.

الشكل 1. رسم تخطيطي للتصميم العمل. لقد تم تعديل هذا الرقم من هارت وآخرون 20، مع إذن. الرجاء انقر هنا لعرض نسخة أكبر من هذا الرقم.
{kind=link}
- كما حددوآخرون من المحفزات مكره ومجموعة من المحفزات محايدة من قاعدة البيانات الدولية العاطفية نظام صورة (IAPS). يتم تصنيف الصور IAPS على مقياس من 1-9 لكي تعكس مستويات من الإثارة والتكافؤ 11. أعداد كبيرة تشير التكافؤ الإيجابية العالية والإثارة. اختيار مجموعة من الصور التي تتناسب مع أعمارهم إلى مجموعة الدراسة مثل الصور من الثعابين، العناكب، أو غيرها من الحيوانات.
ملاحظة: وكانت الصور المحفزات مكره، مهمة ذات صلة المستخدمة في هذه الدراسة على تصنيف متوسط التكافؤ 3.38 (SD = 1.78)، ومتوسط تقييم الإثارة 6.14 (SD = 2.08). كانت الصور المحفزات محايدة متوسط التكافؤ من 6.21 (SD = 0.26)، ومتوسط تقييم الإثارة 3.72 (SD = 2.15). - البرنامج النصي مهمة بحيث يتم عرض الصور في ترتيب العشوائية الزائفة عن 1500 ميللي ثانية مع 500 مللي ثانية يعني الفاصل بين التحفيز. المحفزات الحالية الهدف والمهمة ذات صلة صور محايدة لا أكثر من مرة كل 15 ثانية، وجعل كل منها حوالي 4٪ من المحفزات. جيالحدث tter مرات الظهور من أجل توفير أفضل قرار من وظيفة استجابة الدورة الدموية.
- إنشاء 8 مجموعات من الصور، واحدة لكل من 8 أشواط وظيفية مثل التي يتم تقديمها للمشاركين مع ما مجموعه 40 هدفا و40 مهمة ذات صلة صور محايدة على مدار جميع أشواط 8.
2. إعداد المشاركين والمسح الضوئي
- تجنيد الأطفال والمراهقين الذين تتراوح أعمارهم بين 9 و 18 عاما الذين هم إما أشخاص الأصحاء أو الذين هم في خطر كبير عائلي للذهان.
- التأكد من أن الأفراد الأصحاء ليس لديهم أمراض نفسية أو أي من الدرجة الأولى أفراد الأسرة مع مرض نفسي. تأكد من أن المشاركين خطر العائلي يكون على درجة الأولى واحد على الأقل قريب (الوالدين أو الأخوة) مع الفصام. لا اقصائهم عن وجود أمراض نفسية أخرى في أقارب من الدرجة الأولى.
- عمر المباراة بين الجنسين المشاركين صحي مع المشاركين مجموعة المخاطر العائليةالصورة.
- الحصول على الموافقة المسبقة من المشاركين فوق سن ال 18. على سبيل القصر، والحصول على الموافقة المسبقة من الآباء / أولياء الأمور القانونية. بالإضافة إلى ذلك، الحصول على موافقة خطية من القاصرين الذين يشاركون في الدراسة.
- وضع المشاركين في الماسح الضوئي التصوير بالرنين المغناطيسي وهمية من أجل إطلاعهم على البيئة. تلعب تسجيل الصوت من الضوضاء الماسح الضوئي، ويكون لهم إكمال شوط ممارسة هذه المهمة السلوكية من أجل ضمان فهمهم الإرشادات المهمة.
- وضع المشاركين في التصوير بالرنين المغناطيسي الماسح الضوئي والحصول على أي اللازمة بالاشعة توطين الدماغ و / أو صور تشريحية.
- باستخدام مربع الإدخال-MRI آمن، أخبر المشاركين الضغط على زر واحد مع السبابة في الاستجابة لجميع المنبهات الهدف وزر أخرى مع الاصبع الوسطى من أجل جميع المحفزات الأخرى.
- بعد المسح الرنين المغناطيسي الوظيفي، وجمع تقييمات ذاتية من الإثارة والتكافؤ للصور التي استخدمت في الدراسة من مجموعة فرعية من المشاركين. وCURRENحصلت ر الدراسة التصنيفات من 15 الضوابط و13 مع مخاطر عالية العائلي.
3. الحصول على الصور
- المكان المشاركون إلى 3.0 تسلا التصوير بالرنين المغناطيسي الماسح الضوئي. أولا، الحصول على مجموعة من الصور الهيكلية بما في ذلك 3D متحد المستوى صورة تشريحية T1-التباين باستخدام عملية استحواذ تسلسل نبض أشار التدرج مدلل (TR: 5.16 ميللي ثانية، TE: 2.04 ميللي ثانية، مجال الرؤية: 24 سم؛ صورة مصفوفة: 256 × 256، فليب زاوية: 20؛ حجم فوكسل: 0.94 مم × 0.94 مم × 1.9 مم و 68 شرائح المحورية).
- الحصول على البيانات التصوير الوظيفية باستخدام التدرج صدى صدى مستو تسلسل التصوير مع تغطية كامل الدماغ (TR: 2000 مللي ثانية؛ TE: 27 ميللي ثانية، مجال الرؤية: 24 سم؛ صورة مصفوفة: 64 × 64؛ الوجه زاوية: 60؛ حجم فوكسل: 3.75 مم × 3.75 مم × 3.8 مم؛ 34 شرائح المحورية) بحيث يمكن قياسها أن نشاط الدماغ أثناء أداء المهمة السلوكية. تشغيل هذا التسلسل التصوير لكل شوط من هذه المهمة السلوكية. يجب أن تتكون كل شوط من 120 نقطة وقت التصوير.
- تقديم تاكورونا في 8 أشواط الوظيفية، استغرقت كل منهما ما يقرب من 4 دقيقة.
4. تحليلات
- صورة تجهيزها: افتح الرنين المغناطيسي الوظيفي أداة تحليل الخبراء (FEAT) في FSL 12. حدد تحليل المستوى الأول واحصائيات ما قبل.
- على "بيانات" علامة التبويب، حدد عدد الصور المدخلات وأدخل المسار إلى كل من صور MR أنت ذاهب إلى معالجة. تعيين الدليل الإخراج. أدخل مجموع مجلدات، عدد من عمليات الاستحواذ التخلص منها، وTR.
- على "احصائيات ما قبل" علامة التبويب، تعيين تصحيح الحركة إلى MCFLIRT، المكانية تجانس FWHM إلى 5 رسائل الوسائط المتعددة، و "تصحيح توقيت شريحة". حدد "BET استخراج الدماغ" و "وباس" تصفية الزمانية ولكن لم تقم بتحديد B0 unwarping (UNESS لديك خريطة حقل التدرج) أو "I ntensitiy normaization". 12،14.
- على "تسجيل" علامة التبويب، حدد "stru الرئيسيةصورة ctural ". أدخل مسار إلى تجريد الجمجمة المرجحة T1 صورة في هذا الموضوع. استخدم البحث العادي خطي مع لا يقل عن 6 DOF. حدد خانة الاختيار مساحة قياسي. أدخل المسار إلى صورة أطلس MNI. استخدم العادي، خطي بحث مع 12 DOF اضغط العودة.
- استبعاد المشاركين أكبر من 3 ملم رئيس الحركة في X، Y، Z أو الاتجاهات.
- المستوى 1: مقارنة البيانات بين الشروط المهمة في شوط واحد. فتح FEAT. حدد "تحليل المستوى الأول" و "الإحصائيات + بعد احصائيات".
- ضمن علامة التبويب بيانات، تعيين عدد من المدخلات وأدخل المسار إلى كل من صور MR. أدخل مسار "دليل إخراج" أدخل "مجموع أحجام"، عدد من عمليات الاستحواذ التخلص منها، وTR.
- على "الإحصاءات" علامة التبويب، حدد خانة الاختيار "استخدام FILM prewhitening" 16. اضغط على "نموذج كامل SEكبش "الزر. تعيين "عدد من المركبات الكهربائية الأصلي" إلى عدد من الشروط المهمة. لكل حالة، حدد "مخصص (3 شكل عمود)" من القائمة المنسدلة الشكل الأساسي و"انقر نقرا مزدوجا جاما HRF من" الإلتواء "القائمة المنسدلة 17،18 وحدد ملف نصي يحتوي على توقيت المهمة.
- تنسيق هذا الملف النصي في 3 أعمدة مع إدخال واحد لكل "الحدث" من نوع معين. يجب أن يحتوي العمود الأول في الوقت يصيب (بالثواني)، ينبغي أن تتضمن الثانية مدة (ثانية)، ويجب أن يحتوي على ثلث وزن الحدث. على علامة التبويب التباين & F-الاختبارات، وخلق النقيض واحد لكل حالة مهمة واحدة لكل المقارنة.
- على "ما بعد احصائيات" علامة التبويب، حدد "الكتلة" على "مستوى العتبة" القائمة المنسدلة وتعيين "Z عتبة" والكتلة P رhreshold إلى 2.3 و 0.05 على التوالي 8،19.
- على "تسجيل" علامة التبويب، حدد "صورة الهيكلية الرئيسية". أدخل المسار إلى تجريد الجمجمة المرجحة T1 صورة في هذا الموضوع. استخدام البحث العادي خطي مع لا يقل عن 6 DOF. حدد خانة الاختيار "قياسي الفضاء". أدخل المسار إلى MNI الأطلس الصورة. استخدام، بحث الخطي العادي مع 12 دائرة المالية. اضغط على "الذهاب".
- المستوى 2: مقارنة البيانات بين أشواط لكل حالة المهمة. فتح FEAT. حدد "تحليل مستوى أعلى" و "الإحصائيات + بعد احصائيات" من القائمة المنسدلة.
- على علامة التبويب البيانات، حدد "المدخلات هي الدلائل FEAT المستوى الأدنى". تعيين عدد من المدخلات وأدخل المسار إلى كل من صور MR. أدخل مسار "الدليل الإخراج".
- على "الإحصاءات" علامة التبويب، تغيير "آثار المختلطة: FLAME1" مربع التحديد إلى "ثابت Effects ". اضغط على" معالج الإعداد النموذجي "الزر. حدد" متوسط مجموعة واحدة "وانقر على زر" عملية ".
- على "ما بعد احصائيات" علامة التبويب، حدد "الكتلة" على "مستوى العتبة" القائمة المنسدلة وتعيين "Z عتبة" وعتبة "الكتلة P" إلى 2.3 و 0.05 على التوالي 8،19. اضغط على "الذهاب".
- المستوى 3: مقارنة البيانات بين المواضيع لكل حالة مهمة في جميع أشواط. فتح FEAT. حدد "تحليل مستوى أعلى" و "الإحصائيات + بعد احصائيات" من القائمة المنسدلة.
- على علامة التبويب البيانات، حدد "المدخلات هي 3D تعامل الصور من الدلائل FEAT." تعيين عدد من المدخلات وأدخل المسار إلى كل من صور MR. أدخل مسار "الدليل الإخراج".
- على "الإحصاءات" تيمن أساسها، اضغط على "إعداد نموذج كامل". ضبط عدد من المركبات الكهربائية مساو لعدد من المتغيرات مجموعة والمتغيرات مثل مجموعة التشخيص، العمر، الجنس، الخ أدخل القيم لكل موضوع (الإدخال 1 - الإدخال ن) لكل EV. يمكنك استخدام إطار "لصق" من أجل نسخ البيانات من هذه القيم.
- على "تناقضات & F-اختبارات" علامة التبويب، إضافة النقيض لكل متغير الاختبار ولكل النقيض من ذلك (على سبيل المثال، مجموعة التشخيص). لكل متغير الاختبار، تعيين المقابل عن طريق تحديد القيمة 1 في العمود تحت EV المناسب. لكل النقيض من ذلك، تعيين القيمة الأولى إلى 1 والثانية إلى -1. حدد "تم".
- على علامة التبويب "بعد احصائيات"، حدد "الكتلة" على "مستوى العتبة" القائمة المنسدلة وتعيين "Z عتبة" وعتبة "الكتلة P" إلى 2.3 و 0.05 على التوالي 8،19 . اضغط على "الذهاب".
Access restricted. Please log in or start a trial to view this content.
النتائج
لم تكن هناك فروق بين مجموعات على أساس الخصائص الديموغرافية 20. وأشارت البيانات السلوكية أن مهمة الكشف عن الهدف هي على مستوى مناسب من الصعوبة للأطفال والمراهقين الذين تتراوح أعمارهم بين 9-18. في الدراسة الحالية، والضوابط التي تم تحديدها بشكل صحيح 82.36٪ من الأهداف
Access restricted. Please log in or start a trial to view this content.
Discussion
The modified emotional oddball paradigm in the current study has been shown to elicit differences in neural recruitment during selective attention and emotional processing in children and adolescents at risk for schizophrenia. While existing paradigms using the emotional oddball task have been used to investigate neural changes in adult populations with psychiatric illness8, the current paradigm may be particularly useful for measurement of vulnerability markers in younger age groups.
Access restricted. Please log in or start a trial to view this content.
Disclosures
Dr. Perkins is currently receiving grant support from Janssen, and is a consultant to Dainippon. In the past, Dr. Perkins is or has been on speaker's bureau for Eli Lilly and AstraZeneca. Dr. Perkins has previously received grants from AstraZeneca, Bristol-Myers Squibb, Otsuka, Eli Lilly, Janssen and Pfizer; and consulting and educational fees from AstraZeneca, Bristol-Myers Squibb, Eli Lilly, Janssen, Glaxo Smith Kline, Forest Labs, Pfizer and Shire. All other authors declare no biomedical financial interests or potential conflict of interest.
Acknowledgements
We thank Erin Douglas, Anna Evans, and Carolyn Bellion for their contributions to participant recruitment and clinical assessment. We also thank Michael Casp, Zoe Englander, Justin Woodlief, and James Carter for their contributions to data collection and analysis, and Robert M. Hamer for consultation on statistical analysis and editing of the manuscript. Finally, we thank the individuals and their families who participated in this study.
This study was supported by Conte center grant P50 MH064065 from the National Institute of Mental Health. Dr. Hart was supported by T32 HD040127 from the National Institute of Child Health and Human Development.
Access restricted. Please log in or start a trial to view this content.
Materials
| Name | Company | Catalog Number | Comments |
| 3T MRI scanner | GE | BIAC 3T scanner (replaced) |
References
- Kety, S. S., Rosenthal, D., Wender, P. H., Schulsinger, F. Mental illness in the biological and adoptive families of adpoted schizophrenics. Am J Psyc. 128, 302-306 (1971).
- Weinberger, D. R. Implications of normal brain development for the pathogenesis of schizophrenia. Arch Gen Psychia. 44, 660-669 (1987).
- Nuechterlein, K. H., Dawson, M. E. Information processing and attentional functioning in the developmental course of schizophrenic disorders. Schizophr Bul. 10, 160-203 (1984).
- Nuechterlein, K. H. The vulnerability/stress model of schizophrenic relapse: a longitudinal study. Acta Psychiatr Scand, Supp. 382, 58-64 Forthcoming.
- Keshavan, M. S. Premorbid cognitive deficits in young relatives of schizophrenia patients. Front Hum Neurosc. 3 (62), (2010).
- Kiehl, K. A., Liddle, P. F. An event-related functional magnetic resonance imaging study of an auditory oddball task in schizophrenia. Schizophr Re. 48, 159-171 (2001).
- Bramon, E. Is the P300 wave an endophenotype for schizophrenia? A meta-analysis and a family study. Neuroimag. 27, 960-968 (2005).
- Dichter, G. S., Bellion, C., Casp, M., Belger, A. Impaired modulation of attention and emotion in schizophrenia. Schizophr Bul. 36, 595-606 (2010).
- Fichtenholtz, H. M. Emotion-attention network interactions during a visual oddball task. Brain Res Cogn Brain Re. 20, 67-80 (2004).
- Voyvodic, J. T. Real-time fMRI paradigm control, physiology, and behavior combined with near real-time statistical analysis. Neuroimag. 10, 91-106 (1999).
- International affective picture system (IAPS): Digitized photographs, instruction manual and affective ratings. Technical Report A-6. , The Center for Research in Psychophysiology, University of Florida. (2005).
- Smith, S. M. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimag. 23, 208-219 (2004).
- Smith, S. M. Fast robust automated brain extraction. Hum Brain Map. 17, 143-155 (2002).
- Jenkinson, M., Bannister, P., Brady, M., Smith, S. Improved optimization for the robust and accurate linear registration and motion correction of brain images. Neuroimag. 17, 825-841 (2002).
- Jenkinson, M., Smith, S. A global optimisation method for robust affine registration of brain images. Med Image Ana. 5, 143-156 (2001).
- Woolrich, M. W., Ripley, B. D., Brady, M., Smith, S. M. Temporal autocorrelation in univariate linear modeling of FMRI data. Neuroimag. 14, 1370-1386 (2001).
- Beckmann, C. F., Jenkinson, M., Smith, S. M. General multilevel linear modeling for group analysis in FMRI. Neuroimag. 20, 1052-1063 (2003).
- Woolrich, M. W., Behrens, T. E., Beckmann, C. F., Jenkinson, M., Smith, S. M. Multilevel linear modelling for FMRI group analysis using Bayesian inference. Neuroimag. 21, 1732-1747 (2004).
- Genovese, C. R., Lazar, N. A., Nichols, T. Thresholding of statistical maps in functional neuroimaging using the false discovery rate. Neuroimag. 15, 870-878 (2002).
- Hart, S. J. Altered fronto-limbic activity in children and adolescents with familial high risk for schizophrenia. Psychiatry Re. 212, 19-27 (2013).
- Hariri, A. R., Bookheimer, S. Y., Mazziotta, J. C. Modulating emotional responses: effects of a neocortical network on the limbic system. Neurorepor. 11, 43-48 (2000).
- Gottesman, I. I., Gould, T. D. The endophenotype concept in psychiatry: etymology and strategic intentions. Am J Psyc. 160, 636-645 (2003).
- Glahn, D. C., Thompson, P. M., Blangero, J. Neuroimaging endophenotypes: strategies for finding genes influencing brain structure and function. Hum Brain Map. 28, 488-501 (2007).
Access restricted. Please log in or start a trial to view this content.
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionExplore More Articles
This article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved