
Esame obiettivo dell'apparato respiratorio I: percussione e auscultazione
Panoramica
Fonte: Suneel Dhand,MD, Medico curante, Medicina interna, Beth Israel Deaconess Medical Center
Imparare la tecnica corretta per la percussione e l'auscultazione del sistema respiratorio è vitale e viene fornito con la pratica su pazienti reali. La percussione è un'abilità utile che viene spesso saltata durante la pratica clinica quotidiana, ma se eseguita correttamente, può aiutare il medico a identificare la patologia polmonare sottostante. L'auscultazione può fornire una diagnosi quasi immediata per una serie di condizioni polmonari acute, tra cui la broncopneumopatia cronica ostruttiva (BPCO), l'asma, la polmonite e lo pneumotorace.
Le aree per l'auscultazione dei polmoni corrispondono alle zone polmonari. Ogni lobo polmonare può essere raffigurato sotto la parete toracica durante la percussione e l'auscultazione (Figura 1). Il polmone destro ha tre lobi: i lobi superiori, medi e inferiori. Il polmone sinistro ha due lobi: i lobi superiori e inferiori. Il lobo superiore del polmone sinistro ha anche una proiezione separata nota come linguale.
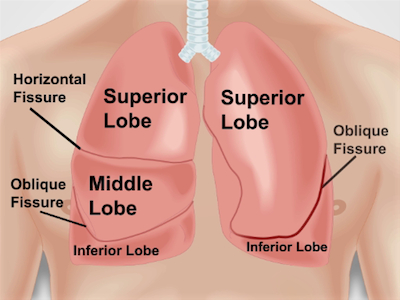
Figura 1. Anatomia dei polmoni rispetto alla parete toracica. Una proiezione approssimativa dei polmoni e delle loro fessure e lobi alla parete toracica anteriormente. RUL - lobo superiore destro; RML - lobo medio destro; RLL - lobo inferiore destro; LUL - lobo superiore sinistro; LLL - lobo inferiore sinistro.
Procedura
1. Posizionamento
- Assicurarsi che il paziente sia spogliato fino alla vita.
- Posizionare il paziente sul tavolo d'esame con un angolo da 30 a 45 gradi e avvicinarsi dal lato destro. L'esame della parte posteriore del polmone richiede che il paziente sia inclinato in avanti o seduto sul bordo del letto.
2. Percussioni
- Percuss sia posteriormente che anteriormente, a partire dalla schiena.
- Posizionare la mano non dominante con il dito medio (dito pless
Applicazione e Riepilogo
La percussione e l'auscultazione dovrebbero sempre essere eseguite in sequenza ogni volta che si esegue un esame respiratorio completo. Imparare a percuss correttamente richiede tempo e pratica (la pratica può essere fatta su te stesso o su altre superfici, come un tavolo). Nota come la nota di percussione cambia naturalmente su polmone pieno d'aria, costole e organi solidi, come il cuore.
L'auscultazione deve essere eseguita su ogni zona polmonare per dare al medico le migliori possibilità ..
Vai a...
Video da questa raccolta:

Now Playing
Esame obiettivo dell'apparato respiratorio I: percussione e auscultazione
Physical Examinations I
213.1K Visualizzazioni

Approccio generale all'esame obiettivo
Physical Examinations I
117.6K Visualizzazioni

Osservazione e ispezione
Physical Examinations I
95.1K Visualizzazioni

Palpazione
Physical Examinations I
84.5K Visualizzazioni

Percussione
Physical Examinations I
101.8K Visualizzazioni

Auscultazione
Physical Examinations I
62.3K Visualizzazioni

Adeguamento corretto dell'abbigliamento del paziente durante l'esame obiettivo
Physical Examinations I
83.4K Visualizzazioni

Misurazione della pressione sanguigna
Physical Examinations I
108.9K Visualizzazioni

Misurazione dei segni vitali
Physical Examinations I
115.0K Visualizzazioni

Esame obiettivo dell'apparato respiratorio I: ispezione e palpazione
Physical Examinations I
157.5K Visualizzazioni

Esame obiettivo del cuore I: ispezione e palpazione
Physical Examinations I
176.7K Visualizzazioni

Esame obiettivo del cuore II: auscultazione
Physical Examinations I
140.1K Visualizzazioni

Esame obiettivo del cuore III: suoni cardiaci anormali
Physical Examinations I
91.9K Visualizzazioni

Esame obiettivo della vascolatura periferica
Physical Examinations I
68.8K Visualizzazioni

Esame vascolare periferico utilizzando un Doppler a onda continua
Physical Examinations I
38.6K Visualizzazioni
Personale delle biblioteche
Copyright © 2025 MyJoVE Corporation. Tutti i diritti riservati