
需要订阅 JoVE 才能查看此. 登录或开始免费试用。
Method Article
结合周围神经刺激和可控脉搏参数经颅磁刺激探测感觉运动控制和学习
摘要
短潜伏期传入抑制 (SAI) 是一种经颅磁刺激方案,用于探测感觉运动整合。本文介绍了如何使用SAI来研究感觉运动行为期间运动皮层中的收敛感觉运动环。
摘要
熟练的运动能力取决于将感觉亲和力有效地整合到适当的运动指令中。传入抑制为探索熟练运动动作过程中对感觉运动整合的程序性和陈述性影响提供了一种有价值的工具。本手稿描述了短潜伏期传入抑制(SAI)对理解感觉运动整合的方法和贡献。SAI 量化了收敛传入凌空抽射对经颅磁刺激 (TMS) 诱发的皮质脊髓运动输出量的影响。传入凌空抽射由周围神经的电刺激触发。TMS刺激被传递到初级运动皮层上的某个位置,该位置在该传入神经服务的肌肉中引起可靠的运动诱发反应。运动诱发反应的抑制程度反映了传入凌空收敛在运动皮层上的大小,并涉及中枢GABA能和胆碱能的贡献。胆碱能参与SAI使SAI成为感觉运动表现和学习中陈述程序相互作用的可能标志物。最近,研究已经开始操纵SAI中的TMS当前方向,以梳理初级运动皮层中不同感觉运动回路的功能意义,以熟练的运动动作。使用最先进的可控脉冲参数TMS(cTMS)控制其他脉冲参数(例如脉冲宽度)的能力增强了TMS刺激探测的感觉运动回路的选择性,并为创建更精细的感觉运动控制和学习模型提供了机会。因此,目前的手稿侧重于使用cTMS进行SAI评估。然而,这里概述的原则也适用于使用传统的固定脉冲宽度TMS刺激器和其他形式的传入抑制(例如长潜伏期传入抑制(LAI))评估的SAI。
引言
多个感觉运动环在运动皮层中汇聚,形成锥体束投影到脊髓运动神经元和中间神经元1。然而,这些感觉运动环如何相互作用以塑造皮质脊髓投射和运动行为仍然是一个悬而未决的问题。短潜伏期传入抑制(SAI)提供了一种工具来探测运动皮层输出中收敛感觉运动环的功能特性。SAI 将运动皮质经颅磁刺激 (TMS) 与相应外周传入神经的电刺激相结合。
TMS是一种非侵入性方法,可安全地刺激人脑中经突触的锥体运动神经元2,3。TMS涉及通过放置在头皮上的盘绕线传递大的瞬态电流。电流的瞬态性质会产生快速变化的磁场,从而在大脑中感应出电流4。在单个TMS刺激的情况下,感应电流激活锥体运动神经元5-7的一系列兴奋性输入。如果产生的兴奋性输入的强度足够,则下降活动会引起对侧肌肉反应,称为运动诱发电位(MEP)。MEP 的潜伏期反映了皮质运动传导时间8。MEP 的振幅指数了皮质脊髓神经元的兴奋性9.引发MEP的单个TMS刺激也可以在条件刺激10,11,12之前进行。这些配对脉冲范式可用于索引各种中间神经元池对皮质脊髓输出的影响。在SAI的情况下,外周电调节刺激用于探测传入凌空对运动皮质兴奋性的影响11,13,14,15。TMS刺激和外周电刺激的相对时间使TMS刺激对运动皮层的作用与到达运动皮层的传入投影保持一致。对于上肢远端肌肉中的 SAI,正中神经刺激通常比 TMS 刺激早 18-24 ms11,13,15,16。同时,SAI随着外周刺激诱导的传入凌空抽射强度增加而增加13,17,18。
尽管SAI与运动皮层传入投射的外在特性密切相关,但它是一种可延展的现象,与许多运动控制过程有关。例如,在即将进行的运动19,20,21之前,SAI在与任务相关的肌肉中减少,但在相邻的任务无关运动表示19,20,22中保持不变。假设对任务相关性的敏感性反映了旨在减少不需要的效应物募集的环绕抑制机制23。最近,有人提出,任务相关效应器中SAI的减少可能反映了一种运动相关的门控现象,旨在抑制预期的感觉情感21并促进感觉运动计划和执行期间的纠正24。无论具体的功能作用如何,SAI都与手动灵活性和处理效率的降低相关25。SAI 改变还与老年人 26 跌倒的风险增加以及帕金森病 26、27、28 和局灶性手肌张力障碍29 中的感觉运动功能受损有关。
临床和药理学证据表明,介导SAI的抑制途径对中枢胆碱能调节敏感30。例如,施用毒蕈碱乙酰胆碱受体拮抗剂东莨菪碱可降低SAI31。相反,通过乙酰胆碱酯酶抑制剂增加乙酰胆碱的半衰期可增强SAI32,33。与药理学证据一致,SAI对中枢胆碱能参与的几种认知过程敏感,包括唤醒34,奖励35,注意力分配21,36,37和记忆38,39,40。在与胆碱能神经元缺失相关的认知缺陷的临床人群中,SAI 也会发生改变,例如阿尔茨海默病 41,42,43,44,45,46,47、帕金森病(伴轻度认知障碍)48,49,50 和轻度认知障碍 47,51,52.对各种γ-氨基丁酸A型(GABAA)受体亚基类型具有差异亲和力的各种苯二氮卓类药物对SAI的差异调节表明,SAI抑制途径不同于介导其他形式的配对脉冲抑制的途径30。例如,劳拉西泮降低SAI,但增强短间隔皮质抑制(SICI)53。唑吡坦可降低SAI,但对SICI53影响不大。地西泮增加SICI,但对SAI53影响不大。GABAA受体功能的这些正变构调节剂降低SAI,再加上观察到GABA控制脑干和皮层中乙酰胆碱的释放54,导致了GABA调节胆碱能途径的假设,该途径投射到感觉运动皮层以影响SAI55。
最近,SAI已被用于研究设置程序运动控制过程的感觉运动环与将程序过程与明确的自上而下目标和认知控制过程对齐的感觉运动回路之间的相互作用21,36,37,38。SAI31 中枢胆碱能受累表明 SAI 可能指对程序性感觉运动控制和学习的执行影响。重要的是,这些研究已经开始通过使用不同的TMS电流方向评估SAI来确定认知对特定感觉运动回路的独特影响。SAI研究通常使用后-前(PA)感应电流,而只有少数SAI研究使用前后(AP)感应电流55。然而,在SAI评估期间,使用TMS诱导AP与PA电流相比,招募了不同的感觉运动回路16,56。例如,对 AP 敏感但不对 PA 敏感的感觉运动回路被小脑调节改变37,56。此外,对AP敏感但不对PA敏感的感觉运动电路由注意力负荷36调制。最后,注意力和小脑影响可能汇聚在相同的AP敏感感觉运动回路上,导致这些回路的适应不良改变37。
TMS技术的进步为操纵单脉冲,配对脉冲和重复应用期间使用的TMS刺激的配置提供了额外的灵活性57,58。可控脉冲参数TMS(cTMS)刺激器现已在全球范围内商业化用于研究用途,这些刺激器提供了对脉冲宽度和形状的灵活控制57。灵活性的提高源于控制两个独立电容器的放电持续时间,每个电容器负责TMS激励的独立相位。激励的双相或单相性质由每个电容器的相对放电幅度(称为M比)控制。cTMS研究将脉冲宽度操作与不同的电流方向相结合,以证明传统TMS刺激器使用的固定脉冲宽度(70-82μs)59,60可能在SAI56期间招募功能不同的感觉运动回路的混合。因此,cTMS是一个令人兴奋的工具,可以进一步解开各种收敛的感觉运动环在感觉运动表现和学习中的功能意义。
这份手稿详细介绍了一种独特的SAI方法来研究感觉运动整合,该方法在感觉运动行为期间将外周电刺激与cTMS相结合。这种方法通过评估传入投影对运动皮层中控制皮质脊髓输出的运动皮层中特定中间神经元群体的影响,改进了典型的SAI方法。虽然相对较新,但cTMS在研究典型和临床人群的感觉运动整合方面具有明显的优势。此外,目前的方法可以很容易地适应于与传统的TMS刺激器一起使用,并量化其他形式的传入抑制和促进,例如长潜伏期传入抑制(LAI)13 或短潜期传入促进(SAF)15。
Access restricted. Please log in or start a trial to view this content.
研究方案
以下协议可应用于各种实验。所提供的信息详细介绍了一个实验,其中SAI用于量化手指对有效或无效提示探针的反应期间的感觉运动整合。在该协议中,SAI在没有任务的情况下进行评估,然后在提示的感觉运动任务期间同时评估,然后在没有任务的情况下再次评估。cTMS刺激器可以被任何市售的常规TMS刺激器取代。然而,传统TMS刺激器的脉冲宽度将固定在70-82μs之间,具体取决于特定的硬件59,60。这项研究得到了滑铁卢大学研究伦理办公室的批准。所有参与者都提供了书面知情同意书。
1. 硬件/软件要求
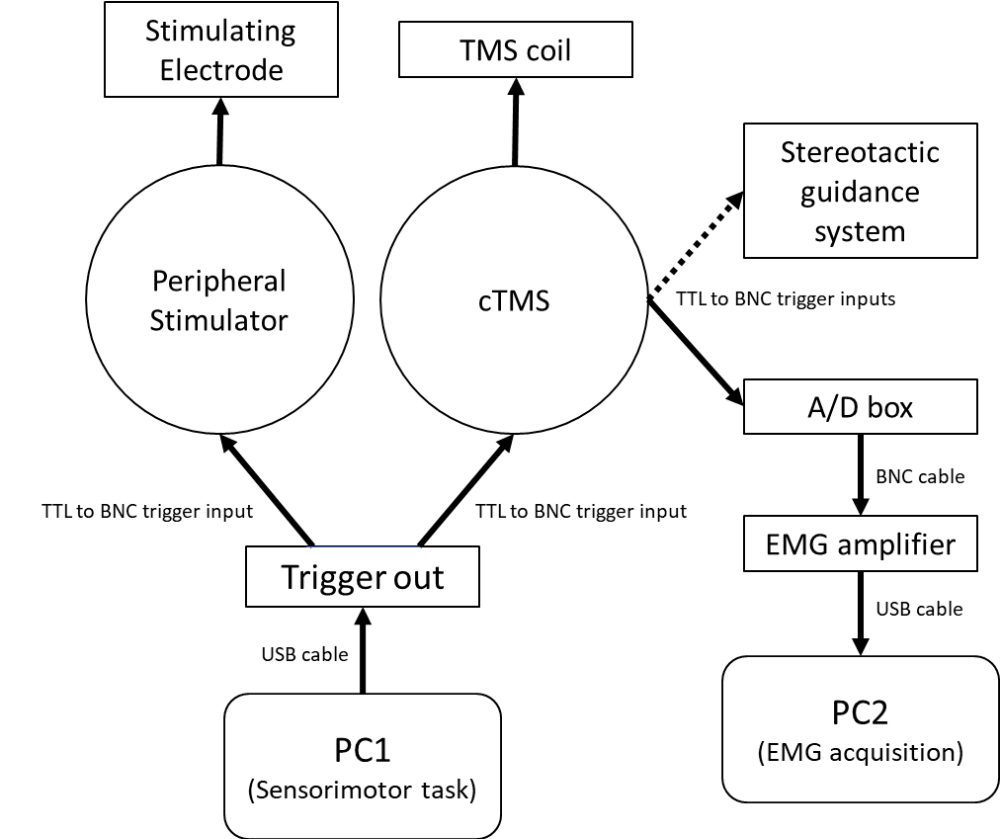
注意: 图1 显示了将外围电气和TMS刺激器与计算机控制的感觉运动任务集成的硬件要求示意图。 图2A描述了PA 感应电流和AP感应电流的SAI设置。 图2B 说明了提示感觉运动任务的事件顺序和SAI评估的相对时间。强烈建议使用立体定向引导系统来跟踪TMS线圈相对于参与者的方向,以减少与线圈位置和轨迹变化相关的生理反应的逐个试验变异性61。

图 1:用于评估静息和并发感觉运动行为期间 SAI 的硬件示意图。 PC1用于控制感觉运动任务和cTMS刺激/外周电刺激的定时,连接到能够通过USB电缆 产生 5 V TTL输出触发的数模转换器。对于无条件试验,来自数字输入输出通道1的触发器 通过 BNC电缆发送到cTMS刺激器。对于条件试验,从数字输入输出通道1触发到cTMS刺激器之前,从数字输入输出通道2触发到外围电刺激器。来自cTMS单元上触发输出通道的BNC电缆被发送到EMG系统模数板,以触发EMG放大器记录,并通过PC2上的EMG采集软件显示/保存数据。来自cTMS触发输出的可选BNC电缆也被发送到立体定向引导系统,以记录cTMS激励时的线圈位置和轨迹。缩写:PC = 个人计算机;USB = 通用串行总线;TTL = 晶体管-晶体管逻辑触发电缆;BNC = 刺刀尼尔-康塞尔曼连接器;cTMS = 可控脉冲参数经颅磁刺激器;TMS = 经颅磁刺激;A/D = 模拟数字;肌电图=肌电图。 请点击此处查看此图的大图。
{kind=link}

图 2:SAI 设置和感觉运动任务。 (A)FDI肌肉中SAI评估的设置示意图。值得注意的是,大脑中的感应电流与TMS线圈中的电流方向相反。(B) 对有效食指提示(顶部)和无效食指提示(底部)试验的描述。提示始终被描述为顶部刺激(由虚线圆圈突出显示)。提示颜色对应于特定的手指响应。参与者被指示尽可能快速准确地响应探针颜色。提示和探针可以是任何颜色。有效提示的概率为 70%。无效线索发生在30%的试验中。缩写:SAI = 短潜伏期传入抑制;PA = 后-前;AP = 前后;FDI = 第一背侧骨间;肌电图=肌电图;MNS = 正中神经刺激。请点击此处查看此图的大图。
{kind=link}
- 为一台个人计算机 (PC1) 配备软件,通过带有两个数字输出通道的 USB(或串行端口)数模板 控制 感觉运动任务。
- 设置一个无任务软件例程来控制无条件cTMS刺激和cTMS刺激的顺序,这些刺激将由外周电刺激调节,刺激间隔(ISI)为21毫秒。使用持续时间在 5-8 秒之间的矩形分布随机化任何两个刺激(例如,有条件或无条件)之间的间隔。
- 确保例程向cTMS单元端口中的触发器发送一个数字输出触发器,用于无条件激励。确保例程将单独的数字输出发送到cTMS单元和外围电刺激器,以用于条件刺激。
- 确保外周刺激器的触发比cTMS触发早21 ms。确保无条件和条件刺激的数量在 8 到 24 之间。理想情况下,无条件试验和有条件试验的顺序应该是随机的。
- 设置软件例程来控制感觉运动任务。确保该软件还将发送到cTMS和外围电刺激器的数字输出触发器的时间锁定到行为期间的特定点。
注意:概述的实验使用提示感觉运动任务(图2B)。使用矩形分布将外周刺激器和cTMS刺激器的触发定时为在响应提示开始后225-275 ms发生。该时间的目的是根据反应线索和先前准备线索之间的有效性评估感觉运动整合的变化,这在所有试验中70%是有效的。 - 为第二台个人计算机 (PC2) 配备连接到模数转换器的双通道肌电图 (EMG) 放大器。确保数模转换器具有数字输入通道,以将EMG时间锁定到TMS激励。确保PC2配备了肌电图数据采集软件,以记录TMS诱发的肌肉反应。
注意:PC1可用于控制感觉运动任务并记录肌电图。然而,研究人员应该独立验证TMS刺激器、外周刺激器和肌电图系统的触发时间。连接到单个 PC 的多个设备会增加中央处理器冲突的可能性,从而导致事件标记的相对计时不稳定。 - 使用以下设置设置EMG数据采集软件:三个记录通道,2个EMG,一个输入触发,TTL触发周围周期为-0.3 s至0.5 s的触发记录,EMG放大因子为1,000x,采样率为4,000 Hz,带通滤波器为3 Hz至1 kHz,电源滤波器(可选)。
注意:当前协议使用划时代的记录方法。肌电图采集软件持续监测肌电图信号。但是,仅显示和记录与TMS刺激时间锁定的纪元数据。 - 将PC1的一个数字输出通道连接到cTMS刺激器上的触发输入。将PC1的第二个数字输出通道连接到外围电刺激器上的触发输入。使用PC的操作系统时,请独立确认PC1的两个数字输出的相对时序。
- 将触发输出连接到EMG系统的数字输入。如果使用立体定向引导系统,则可以将触发输出拆分到引导系统,以记录cTMS刺激时cTMS线圈的试验位置。
2. 参与者筛选和知情同意
- 筛查参与者的TMS 9,62,63,64,65禁忌症。
- 告知参与者研究目标和程序。审查机构道德审查委员会批准的同意文件中概述的风险。回答有关潜在风险的任何问题。在开始任何研究程序之前获得书面知情同意。
3. 肌电图(EMG)电极放置
- 指导参与者坐在实验椅上,肘部放在椅子的扶手上并弯曲,让手腕/手舒适地放在办公桌工作区上。根据需要调整椅子和办公桌工作区的高度。
- 使用放置在圆形化妆棉上的轻度研磨霜清洁第一背骨间 (FDI)、拇短外展肌 (APB) 和尺骨茎突的皮肤。使用酒精准备垫擦去任何残留物。
- 对于每块肌肉,在肌肉腹部放置一个一次性 Ag-AgCl 粘性电极。将第二个电极放在附近的骨地标上作为参考。最后,在尺骨茎突上放置一个额外的Ag-AgCl粘合电极作为接地。
注:一个常见的FDI参考部位是手桡侧第二近端指骨基部的骨突起。一个常见的APB参考部位是拇指桡侧近端指骨突起。 - 将每对电极和接地连接到EMG放大器和数据采集系统。将通道 1 用于 FDI,将通道 2 用于 APB。
4. 外围电刺激器电极放置
- 将外周刺激器的数字输出触发连接到肌电图系统上的触发输入通道,以便在外周刺激传递时触发肌电记录。
- 使用温和的研磨霜清洁前臂内侧的皮肤。从手腕屈曲折痕开始,延伸至~6厘米近端。将清洁范围从手腕中线延伸到前臂桡侧的区域。使用酒精准备垫擦去任何残留物。
- 将导电凝胶涂在可重复使用的刺激棒电极上。使用足够的凝胶覆盖阳极和阴极接触点的金属盘。将刺激电极放在手腕掌侧的皮肤上,阴极靠近阳极。将阴极稍微放在径向茎突的内侧和近端。
- 不要使用过多的凝胶。如果凝胶在阳极和阴极端子之间形成桥梁,请清洁电极以取出所有凝胶,然后重新涂抹。阳极和阴极之间的凝胶桥将沿皮肤转移大量电流,从而难以刺激正中神经。
- 在外围刺激器上,将激励类型选择器设置为单相,将激励持续时间设置为200 μs,并选择合适的电压和安培数,仔细检查任何乘法因子。此处使用的硬件的电压 (Vmax) 设置为 200 V,初始安培数为 0.05 x 10 mA。
- 握住刺激电极的同时,通过按下恒流刺激器上的触发开关来提供单个电刺激。然后,目视检查APB肌肉和EMG显示器(通道2)是否有肌肉收缩的证据。肌肉收缩,称为M波,由电刺激直接激活运动轴突引起,应在外周电刺激伪影后6-9毫秒之间发生。
- 如果没有肌肉收缩的证据,那么询问参与者是否感觉到刺痛感辐射到手指或电极下方。最佳位置是在当前刺激强度下引起最显着的APB肌肉收缩的电极位置。
- 如果没有报告感觉或感觉仅限于电极正下方的皮肤,则以 0.05 的增量增加安培数(乘以 10 倍),直到参与者报告刺痛感辐射到手指/拇指。如果报告在拇指以外的手指有放射感,请通过径向移动电极来重新定位电极,直到感觉辐射到拇指。
- 确定刺激电极的最佳位置后,使用三条胶带将电极固定在手腕上。将第一块放在电极的中间,然后使用第二块和第三块固定电极的顶部和底部。
注意:根据经验,建议先将胶带固定在电极背面,然后将胶带沿着电极侧面敷到皮肤上。这种方法似乎可以固定电极,并最大限度地减少实验过程中横向移动的可能性。 - 固定电极后,要求参与者假设在TMS刺激期间使用的所需肢体方向。检查以确保仍然引起拇指抽搐。
5.正中神经刺激强度的测定
- 通过调整外围刺激强度的安培数来确定外围刺激阈值,直到引发 0.2 mV 的 M 波37,56。如果M波在三次连续刺激上超过所需的0.2 mV目标幅度,则降低安培数。如果 M 波在三个后续刺激下低于所需的 0.2 mV 目标幅度,请增加安培数。阈值是M波超过0.2 mV的第一个安培数值。
注意:一种常见的替代方法是将强度设置为感知感觉阈值的 3 倍或运动阈值 11,16,17,66,67,68 的 1 倍。感觉阈值是参与者正确报告10个电刺激中的5个的感觉的刺激强度。运动阈值是在 10 次刺激中的 5 次中引起可见抽搐的刺激强度。
6. 确定经颅磁刺激的最佳线圈轨迹
- 使用模板磁共振图像 (MRI) 文件创建新的立体定向引导系统项目文件,以监控参与者的位置和线圈方向。然后,将TMS刺激器的数字输出触发器连接到EMG系统上的触发输入通道,以便在TMS刺激传递时触发EMG记录。
注意:如果可用,可以使用特定于受试者的MRI。然而,MEP 足以确定运动皮层刺激研究的最佳线圈位置。 - 将引导系统的线圈跟踪工具固定在 PA TMS 线圈上。使用线圈校准工具将线圈跟踪工具的方向校准到TMS线圈的中点。使用第二个线圈跟踪工具对与PA线圈具有相同几何形状的AP线圈重复此步骤。
- 使用两个肌电图电极将引导系统的受试者跟踪工具固定在参与者的额头上。使用细尖干擦记号笔或眼线笔涂抹器在鼻尖中间、鼻腔以及左右耳前凹陷处放置标记。使用制导系统的被摄体校准工具触摸并记录每个标记的位置。
- 通过将线圈放在参与者的头上并记录线圈轨迹来设置初始线圈位置。确保线圈的中心表面与头皮相切。将线圈的中线与参与者头部的矢状面中平面呈 45° 对齐。
- 为了获得运动皮层热点的起始近似值,想象一条切线连接顶点前 5 厘米和顶点外侧 5 厘米的点,并沿切线在距前点约 2 厘米处放置一个 70 毫米的线圈。
注意:近似对侧手远端肌肉皮质运动热点的另一种方法是让实验者将左手食指(如果刺激参与者的左运动皮层)放在头顶点上,左手拇指放在左耳的耳前点。食指掌指关节的位置可用于可视化放置线圈中心的近似位置。
- 为了获得运动皮层热点的起始近似值,想象一条切线连接顶点前 5 厘米和顶点外侧 5 厘米的点,并沿切线在距前点约 2 厘米处放置一个 70 毫米的线圈。
- 在cTMS刺激器上,将脉冲类型选择器设置为单相阳性,以在下面的神经组织中感应PA电流。接下来,将M比设置为0.2,将刺激强度(也称为功率)设置为最大刺激器输出的30%。最后,将脉冲宽度(也称为正相位持续时间)设置为120 μs(研究中使用的最长脉冲宽度)。
注意: 使用 PA 感应电流确定的线圈位置和轨迹将用于 AP 感应电流 16,36,37,38,56,69。 - 提供三到五个TMS刺激,同时参与者保持FDI肌肉的轻微收缩(~最大自愿收缩的~5%-10%)。如果没有引起运动诱发电位(MEP),将刺激器强度增加10%,并提供三到五个额外的TMS刺激。
- 重复上一步,直到每次刺激始终触发至少0.2mV的MEP,或者直到刺激器强度达到最大刺激器输出的60%-70%。如果没有引出可靠的MEP,请保持刺激参数恒定,并在原始刺激部位周围以~2cm直径的圆圈移动TMS刺激器。如果在原始圆的任何时候仍未引出可靠的 MEP,则将圆的直径增加 1 厘米。
- 一旦引出可靠的 MEP,通过保持刺激参数恒定并将 TMS 刺激器移动到当前线圈位置的北、东、南和西 2 cm 来确认 FDI 电机热点。在每个位置提供三到五个TMS刺激70。如果在四个象限中的任何一个引起持续较大的 MEP,则记录新的线圈位置和轨迹。使用新的线圈位置和轨迹作为皮质运动热点。
7.经颅磁刺激刺激强度的测定
- 启动免费提供的TMS运动阈值评估工具(MTAT 2.1)71,72,73,以确定引发1 mV(1 mV阈值)的MEP所需的刺激强度16,67,74。将估计方法设置为“没有先验信息”,然后单击“开始”。
注意:当前协议使用的TMS强度为1 mV16。然而,一些研究倾向于将强度设置为个体静息运动阈值的 120%。对于AP电流,可能无法获得1 mV MEP。在这种情况下,确定触发 AP 激励配置引发的最大 MEP 的刺激器输出,前提是最大 MEP 至少为 0.5 mV。 - 确定脉冲宽度为 120 μs 的最大刺激器输出。然后,使用转换图表将刺激器输出的范围从 0 重新调整到 100,以便刺激器输出与 MTAT 2.1 软件的比例相匹配。
注意:对于当前研究中使用的模型,脉冲宽度为120 μs的最大刺激器输出为50%。因此,MTAT 2.1软件提供的值除以2以确定在刺激器上设置的值。对于 70 μs 的脉冲宽度,最大刺激器输出为 66%,因此 MTAT 2.1 软件提供的所有值均乘以 0.66(并四舍五入到最接近的 0.5%)。对于30 μs的脉冲宽度,最大刺激器输出为100%。因此,无需调整缩放比例。 - 将 TMS 刺激器强度设置为 MTAT 2.1 软件指示的最大刺激器输出的初始百分比,并提供单个 TMS 刺激。如果在TMS刺激超过1 mV后20-50毫秒的时间范围内记录的MEP,请按 Y 键指示“是”。如果记录的 MEP 小于 1 mV,请按 N 键指示“否”。重复此步骤,直到MTAT软件显示的刺激强度从黑色变为绿色。
注意:MTAT 2.1 软件指示的初始值始终为 37%。对于120 μs的脉冲宽度,实际刺激器值为18.5%。对于70 μs的脉冲宽度,实际刺激器值为24%。对于30μs的脉冲宽度,刺激器值为37%。 - 对当前方向和刺激持续时间的每个组合重复此操作。对于 AP 电流,通过物理旋转线圈将电流方向旋转到 180°,使 PA 电流感应 180°,或使用制造的定制线圈感应 AP 电流。
注意:当使用多个TMS电流方向和脉冲宽度时,所有阈值都可以在数据收集之前或在协议中使用电流方向和脉冲宽度的特定组合之前确定。
8. 短潜伏期传入抑制(无任务基线)
- 将诱导大脑中PA电流的线圈连接到cTMS刺激器。将脉冲类型设置为单相阳性,将 M 比设置为 0.2。将脉冲宽度设置为 120 μs。最后,将刺激强度设置为步骤7中确定的1 mV阈值。
注意:如果同时使用 PA 和 AP 电流方向,则执行步骤 8 的顺序应在参与者之间随机化。如果使用多个脉冲宽度,则执行步骤8的顺序应在参与者之间平衡。PA120 和AP30 是所述实验中唯一采用的电流配置。 - 将外围电刺激强度设置为步骤5中确定的强度。然后,在 PC1 上启动无任务软件例程。接下来,将外围电刺激和TMS刺激之间的刺激间隔设置为21 ms。
- 将TMS线圈放置在步骤6中确定的FDI电机热点上。要求参与者保持FDI肌肉的轻微收缩(~最大自愿收缩的5%-10%)。接下来,在PC1上运行无任务软件以触发外设和cTMS刺激器。
- 使用在大脑中感应 AP 电流的线圈重复 AP30 电流配置的步骤。
注意:建议在时间允许的情况下,在实验结束时重复无任务基线。强烈建议进行无任务前和无任务后的SAI评估,以提供SAI基线并确定组间任何预先存在的差异(如果适用)。
9. 短潜伏期传入抑制(感觉运动任务)
- 将PA线圈连接到cTMS刺激器。将脉冲类型设置为单相阳性,将 M 比设置为 0.2。将脉冲宽度设置为 120 μs。最后,将刺激强度设置为步骤7中确定的1 mV阈值。
注意:当使用多个TMS电流配置(例如,PA120,AP 30)时,在感觉运动任务期间采用的电流配置应在参与者之间平衡。建议使用与确定无任务基线评估顺序相同的平衡。 - 将外围电刺激强度设置为步骤5中确定的强度。然后,在 PC1 上启动感觉运动任务软件例程。将外围电和TMS刺激之间的刺激间隔设置为21毫秒。
- 将TMS线圈放置在步骤6中确定的FDI电机热点上。要求参与者保持FDI肌肉的轻微收缩(~最大自愿收缩的5%-10%)。
- 运行感觉运动任务软件例程来控制感觉运动任务,并将行为锁定的数字触发器发送到外周和cTMS刺激器。将所需数量的无条件和条件试验保持在每种条件下 8 到 24 次刺激之间。
- 使用线圈在大脑中感应 AP 电流,重复 AP30 电流配置的步骤。
10. 数据处理和分析
- 离线目视检查肌电图数据,并丢弃刺激肌电图前均方根(刺激开始的−50)超过标准幅度的任何迹线。计算每个试验的均方根误差,如下所示:

其中 N 是−50和刺激开始之间的数据点数,肌电图是点 n处的电压。对于在静止时肌肉进行的SAI,使用10-15μV的标准幅度。对于以轻微强直收缩评估的SAI,假设在研究期间监测了收缩水平,则使用标准振幅,即所有试验的平均RMSE加上两个标准差。 - 对于每个试验,计算FDI的峰峰值MEP幅度,作为通道1 70中TMS刺激伪影后20 ms至50 ms之间时间窗口中最小值和最大值之间的差异。
- 对于条件试验,计算APB的峰峰值M波幅度,即通道2中外围激励伪影后5 ms至15 ms的峰峰值幅度。
注意:计算峰峰值M波幅度是一种确认刺激强度在整个实验过程中在不同条件下没有变化的方法。 - 计算TMS电流方向,脉冲宽度和行为条件的每种组合的无条件和条件试验的平均MEP幅度和条件试验的平均M波。
- 使用以下公式11 将条件 MEP 振幅表示为每个参与者的非条件 MEP 振幅之比:

注意:较低的比率反映了更有效的抑制。将比率乘以 100% 通常将条件 MEP 振幅表示为非条件 MEP 振幅的百分比。 - 计算每个TMS电流方向,脉冲宽度和行为条件组合的所有参与者的平均值。报告这些值。尽管通常报告平均值,但请尽可能以数字显示单个数据。
Access restricted. Please log in or start a trial to view this content.
结果
图3 显示了使用PA120-和AP30-(下标表示脉冲宽度)感应电流在感觉运动任务期间在FDI肌肉中引发的单个参与者的无条件和条件MEP的示例。中间列中的条形图说明了无条件试验和有条件试验的原始平均峰峰值MEP振幅。右侧的条形图显示了同一参与者的 PA120 和 AP30 感应电流的 SAI 和 MEP 起始延迟。
外周电调节刺激的平均效果是...
Access restricted. Please log in or start a trial to view this content.
讨论
这里描述的SAI方法探测了在感觉运动表现和学习中发挥作用的神经通路子集。在参与者执行受控感觉运动任务时评估 SAI 对于解开众多感觉运动环的复杂贡献至关重要,这些感觉运动环会聚在运动皮质脊髓神经元上,以塑造健康和临床人群的运动输出。例如,类似的方法已被用于确定小脑对程序性运动控制过程的影响37,56以及声明性记忆系统可能影响健康人群21,36,37,38和先前脑震?...
Access restricted. Please log in or start a trial to view this content.
披露声明
作者没有什么可透露的。
致谢
作者感谢自然科学和工程研究委员会(NSERC),加拿大创新基金会(CFI)和安大略省研究基金(ORF)授予S.K.M.的资助。
Access restricted. Please log in or start a trial to view this content.
材料
| Name | Company | Catalog Number | Comments |
| Acquisition software (for EMG) | AD Instruments, Colorado Springs, CO, USA | PL3504/P | LabChart Pro version 8 |
| Alcohol prep pads | Medline Canada Corporation, Mississauga, ON, Canada | 211-MM-05507 | Alliance Sterile Medium, Antiseptic Isopropyl Alcohol Pad (200 per box) |
| Amplifier (for EMG) | AD Instruments, Colorado Springs, CO, USA | FE234 | Quad Bio Amp |
| Cotton round | Cliganic, San Francisco, CA, USA | CL-BE-019-6PK | Premium Cotton Rounds (6-pack, 90 per package) |
| cTMS coils | Rogue Research, Montréal, QC, Canada | COIL70F80301 | 70 mm Medium Inductance Figure-8 coil |
| cTMS coils | Rogue Research, Montréal, QC, Canada | COIL70F80301-IC | 70 mm Medium Inductance Figure-8 coil (Inverted Current) |
| cTMS stimulator | Rogue Research, Montréal, QC, Canada | CTMSMU0101 | Elevate cTMS stimulator |
| Data acquisition board (for EMG) | AD Instruments, Colorado Springs, CO, USA | PL3504 | PowerLab 4/35 |
| Digital to analog board | National Instruments, Austin, TX, USA | 782251-01 | NI USB-6341, X Series DAQ Device with BNC Termination |
| Dispoable adhesive electrodes (for EMG) | Covidien, Dublin, Ireland | 31112496 | Kendal 130 Foam Electrodes |
| Electrogel | Electrodestore.com | E9 | Electro-Gel for Electro-Cap (16 oz jar) |
| Nuprep | Weaver and Company, Aurora, CO, USA | 10-30 | Nuprep skin prep gel (3-pack of 4 oz tubes) |
| Peripheral electrical stimulator | Digitimer, Hertfordshire, UK | DS7R | DS7R High Voltage Constant Current Stimulator |
| Reusable bar electrode | Electrodestore.com | DDA-30 | Black Bar Electrode, Flat, Cathode Distal |
| Software (for behaviour and stimulator triggering) | National Instruments, Austin, TX, USA | 784503-35 | Labview 2020 |
| TMS stereotactic coil guidance system | Rogue Research, Montréal, QC, Canada | KITBSF0404 | BrainSight Neuronavigation System |
| Transpore tape | 3M, Saint Paul, MN, USA | 50707387794571 | Transpore Medical Tape (1 in x 10 yds) |
参考文献
- Bizzi, E., Ajemian, R. From motor planning to execution: a sensorimotor loop perspective. Journal of Neurophysiology. 124 (6), 1815-1823 (2020).
- Chen, R. Studies of human motor physiology with transcranial magnetic stimulation. Muscle & Nerve Supplement. 9, S26-S32 (2000).
- Hallett, M. Transcranial magnetic stimulation: A primer. Neuron. 55 (2), 187-199 (2007).
- Hallett, M. Transcranial magnetic stimulation and the human brain. Nature. 406 (6792), 147-150 (2000).
- Day, B. L., et al. Electric and magnetic stimulation of human motor cortex - Surface EMG and single motor unit responses. Journal of Physiology. 412, 449-473 (1989).
- Di Lazzaro, V., et al. Comparison of descending volleys evoked by transcranial magnetic and electric stimulation in conscious humans. Electroencephalography and Clinical Neurophysiology/Electromyography and Motor Control. 109 (5), 397-401 (1998).
- Di Lazzaro, V., Rothwell, J. C. Corticospinal activity evoked and modulated by non-invasive stimulation of the intact human motor cortex. Journal of Physiology. 592 (19), 4115-4128 (2014).
- Chen, R., et al. The clinical diagnostic utility of transcranial magnetic stimulation: Report of an IFCN committee. Clinical Neurophysiology. 119 (3), 504-532 (2008).
- Rossini, P. M. Non-invasive electrical and magnetic stimulation of the brain, spinal cord, roots and peripheral nerves: Basic principles and procedures for routine clinical and research application. An updated report from an I.F.C.N. Committee. Clinical Neurophysiology. 126 (6), 1071-1107 (2015).
- Kujirai, T., et al. Corticocortical inhibition in human motor cortex. The Journal of Physiology. 471, 501-519 (1993).
- Tokimura, H., et al. Short latency inhibition of human hand motor cortex by somatosensory input from the hand. The Journal of Physiology. 523, 503-513 (2000).
- Nakamura, H., Kitagawa, H., Kawaguchi, Y., Tsuji, H. Intracortical facilitation and inhibition after transcranial magnetic stimulation in conscious humans. The Journal of Physiology. 498, 817-823 (1997).
- Chen, R., Corwell, B., Hallett, M. Modulation of motor cortex excitability by median nerve and digit stimulation. Experimental Brain Research. 129 (1), 77-86 (1999).
- Asmussen, M. J., Jacobs, M. F., Lee, K. G., Zapallow, C. M., Nelson, A. J. Short-latency afferent inhibition modulation during finger movement. PLoS One. 8 (4), e60496(2013).
- Devanne, H. Afferent-induced facilitation of primary motor cortex excitability in the region controlling hand muscles in humans. European Journal of Neuroscience. 30 (3), 439-448 (2009).
- Ni, Z., et al. Transcranial magnetic stimulation in different current directions activates separate cortical circuits. Journal of Neurophysiology. 105 (2), 749-756 (2011).
- Bailey, A. Z., Asmussen, M. J., Nelson, A. J. Short-latency afferent inhibition determined by the sensory afferent volley. Journal of Neurophysiology. 116 (2), 637-644 (2016).
- Fischer, M., Orth, M. Short-latency sensory afferent inhibition: conditioning stimulus intensity, recording site, and effects of 1 Hz repetitive TMS. Brain Stimulation. 4 (4), 202-209 (2011).
- Voller, B., et al. Short-latency afferent inhibition during selective finger movement. Experimental Brain Research. 169 (2), 226-231 (2006).
- Asmussen, M. J., et al. Modulation of short-latency afferent inhibition depends on digit and task-relevance. PLoS One. 9 (8), e104807(2014).
- Suzuki, L. Y., Meehan, S. K. Attention focus modulates afferent input to motor cortex during skilled action. Human Movement Science. 74, 102716(2020).
- Bonassi, G., et al. Selective sensorimotor modulation operates during cognitive representation of movement. Neuroscience. 409, 16-25 (2019).
- Beck, S., Hallett, M. Surround inhibition in the motor system. Experimental Brain Research. 210 (2), 165-172 (2011).
- Seki, K., Fetz, E. E. Gating of sensory input at spinal and cortical levels during preparation and execution of voluntary movement. Journal of Neuroscience. 32 (3), 890-902 (2012).
- Young-Bernier, M., Davidson, P. S., Tremblay, F. Paired-pulse afferent modulation of TMS responses reveals a selective decrease in short latency afferent inhibition with age. Neurobiology of Aging. 33 (4), 1-11 (2012).
- Pelosin, E., et al. Attentional control of gait and falls: Is cholinergic dysfunction a common substrate in the elderly and Parkinson's disease. Frontiers in Aging Neuroscience. 8, 104(2016).
- Dubbioso, R., Manganelli, F., Siebner, H. R., Di Lazzaro, V. Fast intracortical sensory-motor integration: A window into the pathophysiology of Parkinson's disease. Frontiers in Human Neuroscience. 13, 111(2019).
- Oh, E., et al. Olfactory dysfunction in early Parkinson's disease is associated with short latency afferent inhibition reflecting central cholinergic dysfunction. Clinical Neurophysiology. 128 (6), 1061-1068 (2017).
- Richardson, S. P., et al. Changes in short afferent inhibition during phasic movement in focal dystonia. Muscle & Nerve. 37 (3), 358-363 (2008).
- Ziemann, U., et al. TMS and drugs revisited 2014. Clinical Neurophysiology. 126 (10), 1847-1868 (2015).
- Di Lazzaro, V. Muscarinic receptor blockade has differential effects on the excitability of intracortical circuits in the human motor cortex. Experimental Brain Research. 135 (4), 455-461 (2000).
- Di Lazzaro, V., et al. Neurophysiological predictors of long term response to AChE inhibitors in AD patients. Journal of Neurology, Neurosurgery and Psychiatry. 76 (8), 1064-1069 (2005).
- Fujiki, M., Hikawa, T., Abe, T., Ishii, K., Kobayashi, H. Reduced short latency afferent inhibition in diffuse axonal injury patients with memory impairment. Neuroscience Letters. 405 (3), 226-230 (2006).
- Koizume, Y., Hirano, M., Kubota, S., Tanaka, S., Funase, K. Relationship between the changes in M1 excitability after motor learning and arousal state as assessed by short-latency afferent inhibition. Behavioral Brain Research. 330, 56-62 (2017).
- Thabit, M. N., et al. Momentary reward induce changes in excitability of primary motor cortex. Clinical Neurophysiology. 122 (9), 1764-1770 (2011).
- Mirdamadi, J. L., Suzuki, L. Y., Meehan, S. K. Attention modulates specific motor cortical circuits recruited by transcranial magnetic stimulation. Neuroscience. 359, 151-158 (2017).
- Mirdamadi, J. L., Meehan, S. K. Specific sensorimotor interneuron circuits are sensitive to cerebellar-attention interactions. Frontiers in Human Neuroscience. 16, 920526(2022).
- Suzuki, L. Y., Meehan, S. K. Verbal working memory modulates afferent circuits in motor cortex. European Journal of Neuroscience. 48 (10), 3117-3125 (2018).
- Mineo, L., et al. Modulation of sensorimotor circuits during retrieval of negative autobiographical memories: Exploring the impact of personality dimensions. Neuropsychologia. 110, 190-196 (2018).
- Bonnì, S., Ponzo, V., Di Lorenzo, F., Caltagirone, C., Koch, G. Real-time activation of central cholinergic circuits during recognition memory. European Journal of Neuroscience. 45 (11), 1485-1489 (2017).
- Nardone, R., et al. Abnormal short latency afferent inhibition in early Alzheimer's disease: A transcranial magnetic demonstration. Journal of Neural Transmission. 115 (11), 1557-1562 (2008).
- Nardone, R., Bratti, A., Tezzon, F. Motor cortex inhibitory circuits in dementia with Lewy bodies and in Alzheimer's disease. Journal of Neural Transmission. 113 (11), 1679-1684 (2006).
- Di Lazzaro, V., et al. In vivo cholinergic circuit evaluation in frontotemporal and Alzheimer dementias. Neurology. 66 (7), 1111-1113 (2006).
- Di Lazzaro, V., et al. Functional evaluation of cerebral cortex in dementia with Lewy bodies. NeuroImage. 37 (2), 422-429 (2007).
- Di Lazzaro, V., et al. In vivo functional evaluation of central cholinergic circuits in vascular dementia. Clinical Neurophysiology. 119 (11), 2494-2500 (2008).
- Marra, C., et al. Central cholinergic dysfunction measured "in vivo" correlates with different behavioral disorders in Alzheimer's disease and dementia with Lewy body. Brain Stimulation. 5 (4), 533-538 (2012).
- Mimura, Y., et al. Neurophysiological biomarkers using transcranial magnetic stimulation in Alzheimer's disease and mild cognitive impairment: A systematic review and meta-analysis. Neuroscience & Biobehavioral Reviews. 121, 47-59 (2021).
- Yarnall, A. J., et al. Short latency afferent inhibition: a biomarker for mild cognitive impairment in Parkinson's disease. Movement Disorders. 28 (9), 1285-1288 (2013).
- Celebi, O., Temuçin, C. M., Elibol, B., Saka, E. Short latency afferent inhibition in Parkinson's disease patients with dementia. Movement Disorders. 27 (8), 1052-1055 (2012).
- Martin-Rodriguez, J. F., Mir, P. Short-afferent inhibition and cognitive impairment in Parkinson's disease: A quantitative review and challenges. Neuroscience Letters. 719, 133679(2020).
- Nardone, R., et al. Short latency afferent inhibition differs among the subtypes of mild cognitive impairment. Journal of Neural Transmission. 119 (4), 463-471 (2012).
- Tsutsumi, R., et al. Reduced interhemispheric inhibition in mild cognitive impairment. Experimental Brain Research. 218 (1), 21-26 (2012).
- Di Lazzaro, V., et al. Segregating two inhibitory circuits in human motor cortex at the level of GABAA receptor subtypes: A TMS study. Clinical Neurophysiology. 118 (10), 2207-2214 (2007).
- Giorgetti, M., et al. Local GABAergic modulation of acetylcholine release from the cortex of freely moving rats. European Journal of Neuroscience. 12 (6), 1941-1948 (2000).
- Turco, C. V., Toepp, S. L., Foglia, S. D., Dans, P. W., Nelson, A. J. Association of short- and long-latency afferent inhibition with human behavior. Clinical Neurophysiology. 132 (7), 1462-1480 (2021).
- Hannah, R., Rothwell, J. C. Pulse duration as well as current direction determines the specificity of transcranial magnetic stimulation of motor cortex during contraction. Brain Stimulation. 10 (1), 106-115 (2017).
- Peterchev, A. V., D'Ostilio, K., Rothwell, J. C., Murphy, D. L. Controllable pulse parameter transcranial magnetic stimulator with enhanced circuit topology and pulse shaping. Journal of Neural Engineering. 11 (5), 056023(2014).
- Peterchev, A. V., Murphy, D. L., Lisanby, S. H. Repetitive transcranial magnetic stimulator with controllable pulse parameters (cTMS). Annual International Conference of the IEEE Engineering in Medicine and Biology Society. 2010, 2922-2926 (2010).
- Rothkegel, H., Sommer, M., Paulus, W., Lang, N. Impact of pulse duration in single pulse TMS. Clinical Neurophysiology. 121 (11), 1915-1921 (2010).
- MagPro Family User Guide. MagVenture A/S. , Available from: https://tsgdoc.socsci.ru.nl/images/a/ac/Magpro_family.pdf (2022).
- Bashir, S., Edwards, D., Pascual-Leone, A. Neuronavigation increases the physiologic and behavioral effects of low-frequency rTMS of primary motor cortex in healthy subjects. Brain Topography. 24 (1), 54-64 (2011).
- Rossi, S., Hallett, M., Rossini, P. M., Pascual-Leone, A. Screening questionnaire before TMS: An update. Clinical Neurophysiology. 122 (8), 1686(2011).
- Keel, J. C., Smith, M. J., Wassermann, E. M. A safety screening questionnaire for transcranial magnetic stimulation. Clinical Neurophysiology. 112 (4), 720(2001).
- Wassermann, E. M. Risk and safety of repetitive transcranial magnetic stimulation: report and suggested guidelines from the International Workshop on the Safety of Repetitive Transcranial Magnetic Stimulation, June 5-7, 1996. Electroencephalography and Clinical Neurophysiology. 108 (1), 1-16 (1998).
- Rossi, S., et al. Safety and recommendations for TMS use in healthy subjects and patient populations, with updates on training, ethical and regulatory issues: Expert guidelines. Clinical Neurophysiology. 132 (1), 269-306 (2021).
- Udupa, K., Ni, Z., Gunraj, C., Chen, R. Effects of short latency afferent inhibition on short interval intracortical inhibition. Journal of Neurophysiology. 111 (6), 1350-1361 (2013).
- Udupa, K., Ni, Z., Gunraj, C., Chen, R. Interactions between short latency afferent inhibition and long interval intracortical inhibition. Experimental Brain Research. 199 (2), 177-183 (2009).
- Turco, C. V., El-Sayes, J., Fassett, H. J., Chen, R., Nelson, A. J. Modulation of long-latency afferent inhibition by the amplitude of sensory afferent volley. Journal of Neurophysiology. 118 (1), 610-618 (2017).
- Sakai, K., et al. Preferential activation of different I waves by transcranial magnetic stimulation with a figure-of-eight-shaped coil. Experimental Brain Research. 113 (1), 24-32 (1997).
- Groppa, S., et al. A practical guide to diagnostic transcranial magnetic stimulation: Report of an IFCN committee. Clinical Neurophysiology. 123 (5), 858-882 (2012).
- ClinicalResearcher.org. , Available from: https://www.clinicalresearcher.org/software.htm (2022).
- Awiszus, F. TMS and threshold hunting. Supplements to Clinical Neurophysiology. 56, 13-23 (2003).
- Silbert, B. I., Patterson, H. I., Pevcic, D. D., Windnagel, K. A., Thickbroom, G. W. A comparison of relative-frequency and threshold-hunting methods to determine stimulus intensity in transcranial magnetic stimulation. Clinical Neurophysiology. 124 (4), 708-712 (2013).
- Cash, R. F., Isayama, R., Gunraj, C. A., Ni, Z., Chen, R. The influence of sensory afferent input on local motor cortical excitatory circuitry in humans. Journal of Physiology. 593 (7), 1667-1684 (2015).
- Hayes, K. D., Khan, M. E. R., Barclay, N. E., Meehan, S. K. The persistent effects of sports-related concussion during adolescence on sensorimotor integration. Canadian Association for Neuroscience Meeting. , Canadian Association for Neuroscience. Victoria, Canada. (2022).
- Turco, C. V., et al. Short- and long-latency afferent inhibition; Uses, mechanisms and influencing factors. Brain Stimulation. 11 (1), 59-74 (2018).
- Casula, E. P., Rocchi, L., Hannah, R., Rothwell, J. C. Effects of pulse width, waveform and current direction in the cortex: A combined cTMS-EEG study. Brain Stimulation. 11 (5), 1063-1070 (2018).
- D'Ostilio, K., et al. Effect of coil orientation on strength-duration time constant and I-wave activation with controllable pulse parameter transcranial magnetic stimulation. Clinical Neurophysiology. 127 (1), 675-683 (2016).
- Barclay, N. E., Graham, K. R., Hayes, K. D., Meehan, S. K. Program No. 474.08.The contribution of oscillatory activity to the modulation of different sensorimotor circuits under varying working memory load. Society for Neuroscience Annual Meeting. , Society for Neuroscience. Washington, D.C. (2022).
- Dubbioso, R., Raffin, E., Karabanov, A., Thielscher, A., Siebner, H. R. Centre-surround organization of fast sensorimotor integration in human motor hand area. NeuroImage. 158, 37-47 (2017).
- Adams, F. C., et al. Tactile sensorimotor training does not alter short- and long-latency afferent inhibition. Neuroreport. 34 (3), 123-127 (2023).
- Paparella, G., Rocchi, L., Bologna, M., Berardelli, A., Rothwell, J. Differential effects of motor skill acquisition on the primary motor and sensory cortices in healthy humans. Journal of Physiology. 598 (18), 4031-4045 (2020).
- Deveci, S., et al. Effect of the brain-derived neurotrophic factor gene Val66Met polymorphism on sensory-motor integration during a complex motor learning exercise. Brain Research. 1732, 146652(2020).
- Turco, C. V., Locke, M. B., El-Sayes, J., Tommerdahl, M., Nelson, A. J. Exploring behavioral correlates of afferent inhibition. Brain Sciences. 8 (4), 64(2018).
- Mang, C. S., Bergquist, A. J., Roshko, S. M., Collins, D. F. Loss of short-latency afferent inhibition and emergence of afferent facilitation following neuromuscular electrical stimulation. Neuroscience Letters. 529 (1), 80-85 (2012).
- Mirdamadi, J. L., Block, H. J. Somatosensory changes associated with motor skill learning. Journal of Neurophysiology. 123 (3), 1052-1062 (2020).
- Bologna, M., et al. Bradykinesia in Alzheimer's disease and its neurophysiological substrates. Clinical Neurophysiology. 131 (4), 850-858 (2020).
- Schirinzi, T. Amyloid-mediated cholinergic dysfunction in motor impairment related to Alzheimer's disease. Journal of Alzheimer's Disease. 64 (2), 525-532 (2018).
- Cohen, L. G., Starr, A. Localization, timing and specificity of gating of somatosensory evoked potentials during active movement in man. Brain. 110 (2), 451-467 (1987).
- Brown, K. E., et al. The reliability of commonly used electrophysiology measures Active and resting motor threshold are efficiently obtained with adaptive threshold hunting. Brain Stimulation. 10 (6), 1102-1111 (2017).
- Turco, C. V., Pesevski, A., McNicholas, P. D., Beaulieu, L. D., Nelson, A. J. Reliability of transcranial magnetic stimulation measures of afferent inhibition. Brain Research. 1723, 146394(2019).
- Rehsi, R. S., et al. Investigating the intra-session reliability of short and long latency afferent inhibition. Clinical Neurophysiology Practice. 8, 16-23 (2023).
- Toepp, S. L., Turco, C. V., Rehsi, R. S., Nelson, A. J. The distribution and reliability of TMS-evoked short- and long-latency afferent interactions. PLoS One. 16 (12), e0260663(2021).
- Alle, H., Heidegger, T., Krivanekova, L., Ziemann, U. Interactions between short-interval intracortical inhibition and short-latency afferent inhibition in human motor cortex. Journal of Physiology-London. 587 (21), 5163-5176 (2009).
- Noda, Y., et al. A combined TMS-EEG study of short-latency afferent inhibition in the motor and dorsolateral prefrontal cortex. Journal of Neurophysiology. 116 (3), 938-948 (2016).
- Noda, Y. Reduced prefrontal short-latency afferent inhibition in older adults and its relation to executive function: A TMS-EEG study. Frontiers in Aging Neuroscience. 9, 119(2017).
- Noda, Y., et al. Reduced short-latency afferent inhibition in prefrontal but not motor cortex and its association with executive function in schizophrenia: A combined TMS-EEG study. Schizophrenia Bulletin. 44 (1), 193-202 (2018).
Access restricted. Please log in or start a trial to view this content.
转载和许可
请求许可使用此 JoVE 文章的文本或图形
请求许可探索更多文章
This article has been published
Video Coming Soon
版权所属 © 2025 MyJoVE 公司版权所有,本公司不涉及任何医疗业务和医疗服务。