
Exploración abdominal IV: Evaluación de dolor abdominal agudo
Visión general
Fuente: José Donroe, MD, medicina interna y Pediatría, escuela de Yale de la medicina, New Haven, CT
Dolor abdominal es una preocupación frecuente que presenta en el Departamento de la emergencia y el ajuste de la oficina. Dolor abdominal agudo se define como el dolor dura menos de siete días, mientras que el abdomen agudo se refiere a la aparición brusca de dolor abdominal severo con características que sugerían un proceso quirúrgico intervenable. La diagnosis diferenciada del dolor abdominal agudo es amplia; por lo tanto, los clínicos deben tener un método sistemático de examen guiado por una historia cuidadosa, recordando que la patología fuera del abdomen también puede causar dolor abdominal, incluyendo trastornos pulmonares, cardiacos, rectales y genitales.
Terminología para describir la situación de sensibilidad abdominal incluye la derecha e izquierdas cuadrantes superiores e inferiores y las regiones epigástricas y umbilicales hipogástricas (figuras 1, 2). Examen exhaustivo requiere un enfoque organizado que implica inspección, auscultación, percusión y palpación, con cada maniobra realizada útil y con una representación mental clara de la anatomía. En vez de palpar al azar en el abdomen, comience a palpar remotamente desde el sitio de ternura, avanzar sistemáticamente hacia la región tierna y pensando en lo que se encuentra por debajo de los dedos en cada posición. Una técnica útil es imaginar una cara de reloj con el proceso de xiphoid en 12:00 y la sínfisis púbica en el 6:00 (figura 3). Cuando palpando en 8:00, hay piel, músculo, intestino ciego, apéndice y los uréteres. Realizar el examen de esta manera ayuda en el razonamiento clínico y minimiza la posibilidad de patología que falta.
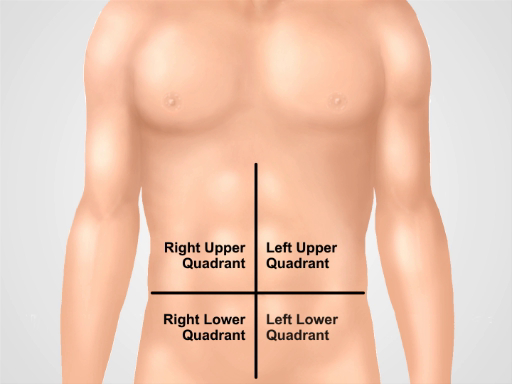
Figura 1. Cuatro cuadrantes abdominales. Abdomen se puede dividir en cuatro regiones por dos líneas imaginarias que se intersecan en el ombligo. Cuadrante superior derecho (a menudo señalado como en CSD), cuadrante (LUQ), superior derecho cuadrante inferior (CID) y cuadrante inferior izquierdo (CII) se muestran a la izquierda.
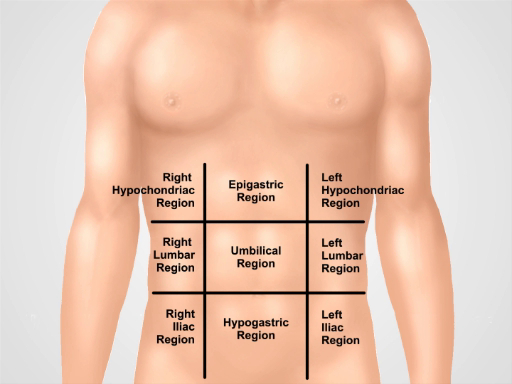
Figura 2. Nueve regiones abdominales. Midclavicular líneas y planos subcostal y intertubercular separan abdomen en nueve regiones: región epigástrica, región derecha hipocondríaco, región izquierda hypochondriac, región umbilical, región lumbar derecha, región lumbar izquierda, hypogastric de la región, región inguinal derecha y región inguinal izquierda.
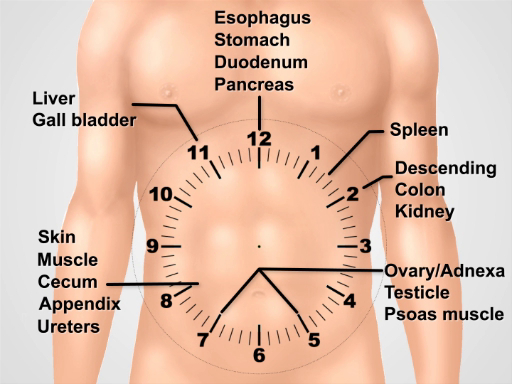
Figura 3. Visualizar una esfera de reloj sobre el abdomen para pensar acerca de la anatomía subyacente mientras se realiza el examen.
Procedimiento
1. preparación
- Lávese las manos y calentarlos antes de examinar al paciente.
- Que el paciente que se ponga una bata. Un paño adicional es necesario para cubrir la parte inferior del cuerpo.
- Comenzar con el paciente acostado decúbito supino en la cama o mesa de examen.
2. enfoque de dolor abdominal agudo
- Las pruebas comienzan con un conjunto completo de constantes vitales.
- Después de entrar a la sala, comenzar inmediatamente a inspecci
Aplicación y resumen
Un enfoque sistemático para examinar a un paciente con dolor abdominal agudo incluye inspección, auscultación, percusión y palpación. Maniobras especiales para detectar abdominal pared dolor, apendicitis, colecistitis, y hernias deben realizarse si existe sospecha de estos procesos.
Los resultados del examen que son más útiles para aumentar la probabilidad de enfermedad incluyen rigidez y percusión ternura por peritonitis general; De McBurney punto de ternura, de Rovsing positivo signo...
Tags
Saltar a...
Vídeos de esta colección:

Now Playing
Exploración abdominal IV: Evaluación de dolor abdominal agudo
Physical Examinations II
67.3K Vistas

Examen de la vista
Physical Examinations II
77.2K Vistas

Oftalmoscopía
Physical Examinations II
68.0K Vistas

Examen de los oídos
Physical Examinations II
55.1K Vistas

Exploración de la nariz, senos paranasales, cavidad oral y faringe
Physical Examinations II
65.8K Vistas

Exploración de la tiroides
Physical Examinations II
105.0K Vistas

Exploración de ganglios linfáticos
Physical Examinations II
387.4K Vistas

Exploración abdominal I: Inspección y auscultación
Physical Examinations II
202.6K Vistas

Exploración abdominal II: Percusión
Physical Examinations II
248.2K Vistas

Exploración abdominal III: Palpación
Physical Examinations II
138.5K Vistas

Tacto rectal masculino
Physical Examinations II
114.5K Vistas

Exploración mamaria
Physical Examinations II
87.6K Vistas

Exploración pélvica I: Evaluación de los genitales externos
Physical Examinations II
307.1K Vistas

Exploración pélvica II: Examen con espéculo
Physical Examinations II
150.4K Vistas

Exploración pélvica III: Bimanual y examen rectovaginal
Physical Examinations II
147.7K Vistas
ACERCA DE JoVE
Copyright © 2025 MyJoVE Corporation. Todos los derechos reservados