
Exame Abdominal IV: Avaliação da Dor Abdominal Aguda
Visão Geral
Fonte: Joseph Donroe, MD, Medicina Interna e Pediatria, Yale School of Medicine, New Haven, CT
A dor abdominal é uma preocupação frequente tanto no pronto-socorro quanto no ambiente do consultório. A dor abdominal aguda é definida como dor que dura menos de sete dias, enquanto um abdômen agudo refere-se ao início abrupto de dor abdominal severa com características que sugerem um processo cirurgicamente intervenível. O diagnóstico diferencial da dor abdominal aguda é amplo; assim, os médicos devem ter um método sistemático de exame orientado por um histórico cuidadoso, lembrando que a patologia fora do abdômen também pode causar dor abdominal, incluindo distúrbios pulmonares, cardíacos, retois e genitais.
A terminologia para descrever a localização da ternura abdominal inclui os quadrantes superior e inferior direito e esquerdo, e as regiões epigástrica, umbilical e hipogástrica(Figuras 1, 2). O exame minucioso requer uma abordagem organizada envolvendo inspeção, auscultação, percussão e palpação, com cada manobra realizada de forma proposital e com uma clara representação mental da anatomia. Em vez de palpating aleatoriamente através do abdômen, comece a palpating remotamente do local da ternura, movendo-se sistematicamente em direção à região terna, e pensando sobre o que está abaixo dos dedos em cada posição. Uma técnica útil é imaginar um relógio com o processo xifoide às 12:00 e a profífise púbica às 6:00(Figura 3). Quando palpating às 8:00, há pele, músculo, ceco, apêndice e ureteres. A realização do exame dessa forma auxilia no raciocínio clínico e minimiza a chance de faltar à patologia.
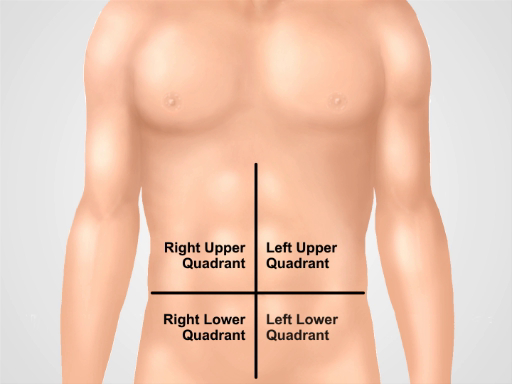
Figura 1. Quatro quadrantes abdominais. O abdômen pode ser dividido em quatro regiões por duas linhas imaginárias que se cruzam no umbigo. O quadrante superior direito (muitas vezes designado como RUQ), o quadrante superior esquerdo (LUQ), o quadrante inferior direito (RLQ) e o quadrante inferior esquerdo (LLQ) são mostrados.
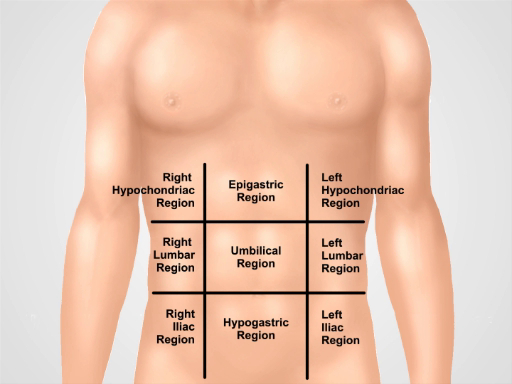
Figura 2. Nove regiões abdominais. Linhas midclaviculares e planos subcostais e intertuberculares separam o abdômen em nove regiões: região epigástrica, região hipocondríaca direita, região hipocondríaca esquerda, região umbilical, região lombar direita, região lombar esquerda, região hipogástrica, região inguinal direita e região inguinal esquerda.
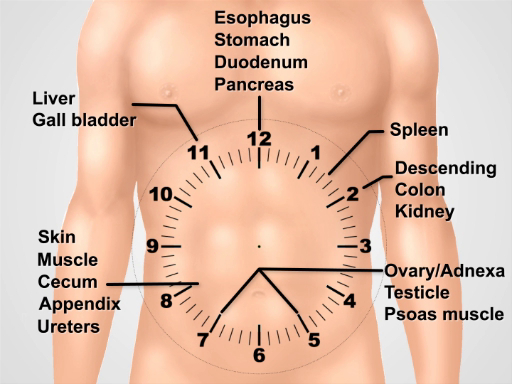
Figura 3. Visualizar um rosto de relógio sobre o abdômen para pensar sobre a anatomia subjacente durante a realização do exame.
Procedimento
1. Preparação
- Lave as mãos e aqueça-as antes de examinar o paciente.
- Que o paciente coloque um vestido. Uma cortina extra é necessária para cobrir a parte inferior do corpo.
- Comece com o paciente deitado na mesa de exame ou na cama.
2. Abordagem da dor abdominal aguda
- Comece com um conjunto completo de testes de sinais vitais.
- Depois de entrar na sala, comece imediatamente uma inspeção cuidadosa. Pacientes com peritonite podem preferir ficar quietos com quadris e joelhos flexionados.
- Coloque uma cortina sobre a parte inferior do corpo da paciente para a profífisis púbica e eleve o vestido para um pouco abaixo dos seios. Note distensão abdominal, cor da pele, sinais de má perfusão, como mottling, pulsação visível ou peristão, protuberâncias e cicatrizes.
- Se o paciente estiver alerta, peça ao paciente que use um dedo para apontar para a área dolorosa. Peça ao paciente para tossir (teste de tosse) ou bater suavemente na cama, o que pode localizar a dor da peritonite.
- Auscultar o quadrante inferior esquerdo usando o diafragma com pressão leve. Sons intestinais ausentes podem indicar um íleo, enquanto sons de alto tom sugerem obstrução mecânica iminente. A auscultação tem o menor rendimento das manobras diagnósticas para dor abdominal.
- Auscultate sobre quaisquer áreas saliente para avaliar para hérnia intestinal.
- Prossiga para usar a cabeça do estetoscópio para palpar os quatro quadrantes com pressão graduada, enquanto continua a auscultar. Observe o rosto do paciente em busca de sinais de angústia e sinta a parede abdominal para rigidez.
- Percusso o abdômen, começando com percussão muito leve (teste de percussão leve) sobre os quatro quadrantes. Isso pode localizar a dor peritoneal e distingui-la da dor visceral.
- Continue com um curso de percussão moderado nos quatro quadrantes, avaliando para tiranidade anormal, sugerindo ar (ar livre ou intestino cheio de gás), ou embotamento, sugerindo fluido ou massa.
- Peça ao paciente para flexionar as pernas nos quadris e joelhos.
- Comece a palpação colocando a mão direita aberta suavemente no abdômen com os dedos ligeiramente espalhados. Use um movimento de balanço leve enquanto o paciente respira, sentindo a rigidez da parede abdominal. Sinta cada quadrante desta forma, começando mais longe do local da dor. Distrair o paciente com a conversa pode servir para minimizar a guarda voluntária.
- Palpate novamente usando pressão moderada com as almofadas dos dedos (não as pontas dos dedos), de forma no sentido horário. No meio da cara do relógio, palpa a aorta.
- Palpate protuberâncias evocando suspeita de hérnias de parede abdominal, e tentam reduzir se presentes.
- Em pacientes selecionados, particularmente aqueles com dor quadrânge inferior ou suspeita de hemorragia gastrointestinal, realizam um exame retal.
- Faça um exame testicular em homens com dor abdominal inferior.
- Faça um exame pélvico em mulheres com dor abdominal.
3. Manobras Especiais em Pacientes Selecionados com Dor Abdominal.
- Teste para o sinal de Murphy em pacientes com dor no quadrante superior direito. Palpato na linha midclavicular, logo abaixo da borda do fígado.
- Peça ao paciente para respirar fundo enquanto você palpa profundamente. Dor acompanhada de cessação de inspiração sugere colecistite aguda.
- Para dor do quadrante inferior direito, as seguintes manobras podem ser diagnosticamente úteis:
- Provocar o sinal de Rovsing por profunda palpação do quadrante inferior esquerdo. Dor referida ao quadrante inferior direito sugere apendicite aguda.
- Realize o sinal de obturador flexionando o quadril direito e o joelho do paciente para 90° e girando internamente o quadril. Dor no quadrante inferior direito sugere apendicite aguda ou abscesso pélvico.
- Realize o sinal de psoas fazendo com que o paciente flexione a coxa direita contra a mão resistida do examinador. Dor abdominal inferior sugere uma apendicite retrocecal ou psoas abscesso. Para realizar um método alternativo do sinal de psoas, coloque o paciente na posição de decúbito lateral esquerdo e, de pé atrás do paciente, estenda a coxa do paciente.
- Realize o teste carnett para avaliar a dor na parede abdominal, que pode imitar patologia intra-abdominal e muitas vezes não diagnosticada. Identifique o ponto de dor máxima no paciente supino, e palpate lá com pressão moderada para obter ternura.
- Peça ao paciente para levantar os ombros da cama como se estivesse fazendo um abdominais, contraindo assim os músculos da parede abdominal. O aumento da dor sugere uma dor na parede abdominal, enquanto a dor melhorada sugere patologia intraperitoneal (agora protegida pelos músculos reto contraídos).
- Avalie-se para esplenomegalia em pacientes com dor do quadrante superior esquerdo ou sinais de hipertensão portal.
- Avalie ascites em pacientes com histórico sugestivo.
- Avaliação para hérnias na virilha: Hérnias sintomáticas na virilha podem estar presentes com dor na virilha, uma protuberância irredutível ou sinais de obstrução intestinal, como distensão abdominal, dor e vômito. A avaliação das hérnias na virilha deve ser realizada em pacientes selecionados com queixas abdominais ou virilha inferiores. Peça ao paciente para se levantar, pois esta é a posição preferida para avaliar hérnias na virilha. Passos 3.6.1. - 3.6.4. também pode ser realizada na posição supina se o paciente não conseguir ficar em pé, embora facilmente hérnias reduíveis possam ser perdidas nesta posição.
- Coloque luvas, e peça ao paciente para levantar o vestido na frente. Inspecione a área do canal inguinal, canal femoral e escroto (machos) em busca de protuberâncias em ambos os lados.
- Identifique o ligamento inguinal que se estende da coluna ilínica superior anterior ao tubérculo púbico. O canal inguinal corre paralelamente a ele, entre os anéis inguinais internos e externos. O anel interno, e a origem das hérnias indiretas, é apenas superior ao ponto médio do ligamento inguinal. O anel inguinal externo é ligeiramente superior e lateral ao tubérculo púbico. O triângulo inguinal, e área de origem das hérnias diretas, é delimitado pela artéria epigástrica inferior lateralmente, o ligamento inguinal inferiormente, e a linha semiclunaris medialmente. O canal femoral está abaixo do ligamento inguinal apenas medial para a veia femoral e artéria.
- Peça ao paciente para virar a cabeça para o lado, tosse ou simplesmente abaixe-se, e continue a observar para um novo abaulamento ou aumento do tamanho de uma protuberância existente.
- Usando as almofadas dos dedos da mão direita para examinar o lado direito, palpa sobre o canal femoral, e pedir ao paciente para tossir ou suportar novamente para avaliar as hérnias femorais. Hérnias femorais são mais comuns em mulheres e mais propensas do que hérnias inguinais a encarcerar.
- Em seguida, palpate sobre o canal inguinal direito. Peça ao paciente para tossir ou suportar para baixo, em seguida, sentir por quaisquer protuberâncias. Uma protuberância em expansão sentida em direção ao ponto médio do ligamento inguinal é provavelmente uma hérnia indireta. Uma protuberância sentida perto do tubérculo púbico é mais provável que uma hérnia direta.
- Auscultar sobre quaisquer protuberâncias, observando a presença ou ausência de sons intestinais.
- No sexo masculino, se uma massa escrotal for observada, palpa-a e tente palpar acima dela para diferenciá-la da patologia testicular.
- Se ainda não houver massa, use o dedo indicador da mão direita, com a almofada do dedo voltada para o paciente, para palpar o anel inguinal externo direito e o canal inguinal distal colocando o dedo no escroto, logo acima do testículo direito.
- Invagiar o escroto, seguindo o cordão espermático superiormente e na direção do canal inguinal até que a ponta do dedo passe do anel inguinal externo. O cordão espermático (machos) e o ligamento redondo (fêmeas) viajam pelo canal inguinal.
- Peça ao paciente para tossir ou suportar. Uma protuberância sentida na ponta do dedo pode ser uma hérnia indireta, enquanto uma sentida na lateral do dedo pode ser uma hérnia direta. Note-se que a capacidade do médico de distinguir entre hérnias diretas e indiretas no exame físico é imprecisa.
- Repita no lado esquerdo usando a mão esquerda.
- Tente reduzir suavemente qualquer suspeita de hérnia, evitando uma redução forçada. A redução é facilitada por ter o paciente deitado na posição Trendelenburg.
Aplicação e Resumo
Uma abordagem sistemática para examinar um paciente com dor abdominal aguda inclui inspeção, auscultação, percussão e palpação. Manobras especiais para detectar dor na parede abdominal, apendicite, colecisto e hérnias devem ser realizadas se houver suspeita para esses processos.
Os achados do exame mais úteis para aumentar a probabilidade de doença incluem rigidez e ternura de percussão para peritonite geral; A ternura pontual de McBurney, o sinal positivo de Rovsing e o sinal positivo de psoas para apendicite; sinal positivo murphy e ternura quadrante superior direito para colecisto; peristalse visível, distensão abdominal e sons intestinais hiperativos agudos para obstrução intestinal pequena.
Achados que diminuem a probabilidade de doença são um sinal positivo de Carnett e dor negativa com tosse para peritonite geral; ausência de ternura do quadrante inferior direito para apendicite; ausência de ternura do quadrante superior direito para colecisto; sons intestinais normais e ausência de distensão abdominal para obstrução intestinal pequena.
A produção do exame abdominal é muito melhor se o médico provocar um histórico efetivo, realizar uma inspeção cuidadosa e considerar a anatomia regional relevante ao percussão e palpação. A relação do médico com o paciente beneficia-se de ter uma abordagem suave para quem já está com dor e evitar manobras desnecessárias que podem aumentar o desconforto do paciente sem fornecer novas informações, como o teste tradicional de ternura de recuperação, onde o médico palpatiza profundamente sobre a área da dor e, em seguida, rapidamente remove a mão palpating, perguntando se a ternura era pior com palpação ou liberação. Um histórico eficaz e exame físico permitem a utilização econômica do diagnóstico por imagem e melhoram a interpretação clínica dos resultados por imagem, além de possibilitar a triagem de pacientes que podem precisar de cirurgia urgente.
Tags
Pular para...
Vídeos desta coleção:

Now Playing
Exame Abdominal IV: Avaliação da Dor Abdominal Aguda
Physical Examinations II
67.3K Visualizações

Exame ocular
Physical Examinations II
77.2K Visualizações

Exame oftalmoscópico
Physical Examinations II
68.0K Visualizações

Exame de orelha
Physical Examinations II
55.1K Visualizações

Exame de Nariz, Seios da face, Cavidade Oral e Faringe
Physical Examinations II
65.8K Visualizações

Exame de Tireóide
Physical Examinations II
105.0K Visualizações

Exame do Linfonodo
Physical Examinations II
387.4K Visualizações

Exame Abdominal I: Inspeção e Auscultação
Physical Examinations II
202.6K Visualizações

Exame Abdominal II: Percussão
Physical Examinations II
248.2K Visualizações

Exame Abdominal III: Palpação
Physical Examinations II
138.5K Visualizações

Exame Retal Masculino
Physical Examinations II
114.5K Visualizações

Exame Abrangente das Mamas
Physical Examinations II
87.6K Visualizações

Exame Pélvico I: Avaliação da Genitália Externa
Physical Examinations II
307.1K Visualizações

Exame Pélvico II: Exame Especular
Physical Examinations II
150.4K Visualizações

Exame Pélvico III: Exame Bimanual e Retovaginal
Physical Examinations II
147.7K Visualizações
Copyright © 2025 MyJoVE Corporation. Todos os direitos reservados