
Examen abdominal IV: Évaluation de la douleur abdominale aiguë
Vue d'ensemble
Source : Joseph Donroe, MD, médecine interne et pédiatrie, Yale School of Medicine, New Haven, CT.
La douleur abdominale est une préoccupation fréquente présente à la fois l’urgence et l’environnement de bureau. Une douleur abdominale aiguë est définie comme une durée inférieure à sept jours, tandis qu’un abdomen aigu se réfère à l’apparition brutale d’une douleur abdominale sévère caractéristiques suggérant un processus chirurgicalement intervenable la douleur. Le diagnostic différentiel d’une douleur abdominale aiguë est large ; ainsi, les cliniciens doivent avoir une méthode systématique de l’examen, guidé par une anamnèse rigoureuse, se souvenant que la pathologie en dehors de l’abdomen peut également causer des douleurs abdominales, notamment des troubles pulmonaires, cardiaques, rectales et génitales.
Terminologie pour décrire l’emplacement de la sensibilité abdominale comprend le droit et gauche quadrants supérieurs et inférieurs et les régions épigastriques, ombilicales et hypogastrique (Figures 1, 2). Examen approfondi nécessite une approche organisée impliquant l’inspection, l’auscultation, percussion et palpation, avec chaque manoeuvre effectuée délibérément et avec une représentation mentale précise de l’anatomie. Plutôt que de la palpation au hasard dans l’ensemble de l’abdomen, commencer palpant à distance à partir du site de tendresse, de passer systématiquement vers la région d’appel d’offres et penser à ce qui se cache sous les doigts à chaque position. Une technique utile consiste à imaginer un cadran avec le processus xiphoïde à 12:00 et la symphyse pubienne à 06:00 (Figure 3). Lorsque palpant à 08:00, il y a la peau, muscle, caecum, appendice et uretères. Effectuer l’examen de cette façon assiste au raisonnement clinique et réduit le risque de pathologie manquant.
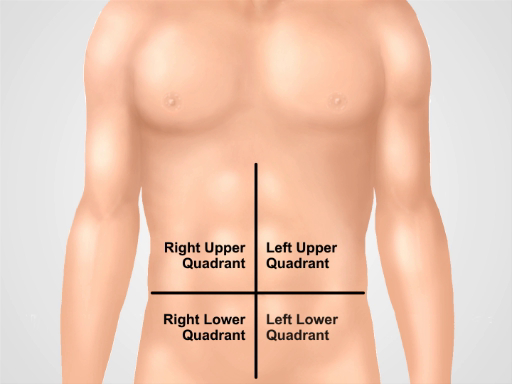
Figure 1. Quatre quadrants abdominaux. Abdomen se divisent en quatre régions par deux lignes imaginaires qui se croisent à l’ombilic. Quadrant supérieur droit (souvent dénommée dans le QSD), hypocondre (LUQ), de la droite, quadrant inférieur droit (RLQ) et quadrant inférieur gauche (LLQ) sont affichés à gauche.
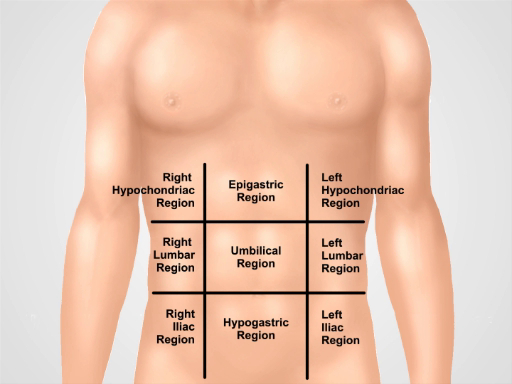
Figure 2. Neuf régions abdominales. Claviculaire lignes et plans sous-costales et intertubercular sépareront l’abdomen en neuf régions : région épigastrique, région droite hypocondriaque, région hypocondriaque gauche, région ombilicale, région lombaire droite, région lombaire gauche, région hypogastrique, région inguinale droite et gauche région inguinale.
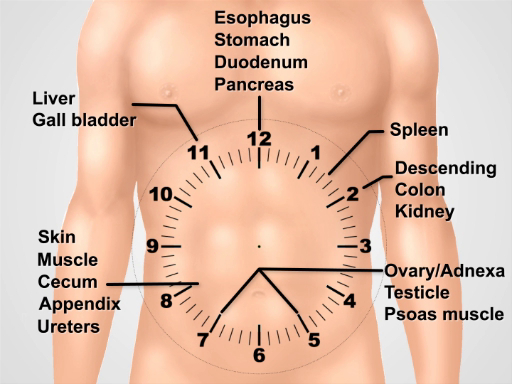
La figure 3. Visualiser un cadran sur l’abdomen pour penser l’anatomie sous-jacente lors de l’exécution de l’examen.
Procédure
1. préparation
- Lavez-vous les mains et les réchauffer avant d’examiner le patient.
- Que le patient soit mis sur une robe. Un drapé supplémentaire n’est nécessaire pour couvrir la partie inférieure du corps.
- Commencer avec le patient se trouvant en position couchée sur le lit ou la table d’examen.
2. approche de la douleur abdominale aiguë
- Commencez avec un jeu complet de tests des signes vitaux.
- Après être entré dans la salle, commencer immédiatement une inspection minutieuse. Les patients qui présentent une péritonite peuvent préférer se trouvent toujours avec flexion hanches et genoux.
- Placez un drap sur la partie inférieure du corps du patient à la symphyse pubienne et soulever la robe juste sous les seins. Notez la distension abdominale, couleur de la peau, signes de mauvaise perfusion, tels que les marbrures, pulsation visible ou péristaltisme, renflements et les cicatrices.
- Si le patient est alerte, demandez au patient d’utiliser un seul doigt pour pointer vers la zone douloureuse. Demandez au patient de tousser (test de la toux) ou cogner doucement le lit, ce qui peut localiser la douleur de la péritonite.
- Ausculter le quadrant inférieur gauche à l’aide de la membrane avec une légère pression. En l’absence de l’intestin sons peuvent indiquer un iléus, tandis que sons élevés suggèrent une obstruction mécanique imminente. L’auscultation a le rendement le plus bas des manœuvres diagnostiques pour des douleurs abdominales.
- Ausculter sur toutes les zones bombés à évaluer pour la hernie de l’intestin.
- Passez à la tête du stéthoscope permet de palper les quatre quadrants avec pression graduée, tout en continuant à ausculter. Observer le patient faire face à des signes de détresse et sentir la paroi abdominale pour la rigidité.
- Percuss l’abdomen, commençant très légère percussion (épreuve de percussion légère) sur les quatre quadrants. Cela peut localiser la douleur péritonéale et distinguer des douleurs viscérales.
- Continuer avec une course de percussion modérée dans les quatre quadrants, évaluer pour tympany anormale, suggérant l’air (air libre ou gazeuse de l’intestin), ou matité, suggérant des fluides ou massives.
- Demander au patient de fléchir les jambes sur les hanches et les genoux.
- Commencer palpation en plaçant la main droite ouverte doucement sur le ventre avec les doigts que légèrement se propager. Utiliser un léger mouvement à bascule que le patient respire, se sentant pour la rigidité de la paroi abdominale. Sentir chaque quadrant de cette façon, commençant plus éloigné du site de la douleur. Distraire le patient avec conversation peut servir à minimiser garde volontaire.
- Palper avec une pression modérée avec les pads de doigt (pas du bout des doigts), de manière dans le sens horaire. Au milieu du cadran, palper l’aorte.
- Palper les renflements évoquant les soupçons de hernies de la paroi abdominale et tenter de réduire le cas échéant.
- Chez certains patients, particulièrement ceux avec douleur du quadrant inférieur ou de suspicion de saignement gastro-intestinal, effectuez un examen rectal.
- Procédera à un examen testiculaire sur les hommes avec des douleurs abdominales basses.
- Effectuer un examen gynécologique sur les femmes souffrant de douleurs abdominales.
3. spéciales manoeuvres chez certains Patients souffrant de douleurs abdominales.
- Essai de signe de Murphy chez les patients souffrant de douleurs de l’hypocondre droit. Palper la ligne claviculaire, juste sous le bord du foie.
- Demander au patient de prendre une profonde respiration tandis que vous Palpez profondément. La douleur accompagnée de cessation d’inspiration suggère la cholécystite aiguë.
- Pour douleur du quadrant inférieure droit, les manoeuvres suivantes peuvent être diagnostique utiles :
- Susciter signe de Rovsing par palpation profonde du quadrant inférieur gauche. Dénommé le quadrant inférieur droit la douleur suggère l’appendicite aiguë.
- Effectuer le signe de l’obturateur en flexion de hanche droite du patient et le genou à 90° et rotation en interne de la hanche. Douleur dans le quadrant inférieur droit indique appendicite aiguë ou un abcès pelvien.
- Effectuer le signe du psoas en ayant le patient flex la cuisse droite contre main résistant de l’examinateur. Douleur abdominale basse suggère un abcès de retrocecal appendicite ou du psoas. Pour effectuer une autre méthode du signe du psoas, placer le patient en position de décubitus latéral gauche et placez-vous derrière le patient, s’étendent de la cuisse du patient.
- Effectuez le test de Carnett à évaluer pour la douleur de la paroi abdominale, qui peut imiter les pathologie intra-abdominale et va souvent non diagnostiqués. Identifier le point de douleur maximale chez le patient en décubitus dorsal et palper là avec une pression modérée pour susciter la tendresse.
- Demandez au patient de lever les épaules hors du lit, comme si faire un Sit-up, contractant ainsi les muscles de la paroi abdominale. Augmentation de la douleur suggère une douleur de la paroi abdominale, alors que la douleur améliorée suggère pathologie intrapéritonéale (maintenant protégée par les muscles contractés rectus).
- Évaluer pour splénomégalie chez des patients avec douleur du quadrant supérieur gauche ou des signes d’hypertension portale.
- Évaluer pour ascite chez les patients ayant des antécédents évocateurs.
- Évaluer pour les hernies de l’aine : hernie de l’aine symptomatiques peut-être être présents avec douleur à l’aine, un renflement unreducible ou des signes d’obstruction intestinale, tels que la distension abdominale, douleurs et de vomissements. Cotisation pour l’aine, il faudrait faire les hernies chez des patients sélectionnés avec inférieure abdominale ou aine plaintes. Demander au patient de se tenir, car c’est la position préférée à évaluer pour les hernies de l’aine. 3.6.1 les étapes. -3.6.4. peut également être effectuée en décubitus dorsal si le patient est incapable de se tenir, bien que facilement réductibles hernies peuvent manquer dans cette position.
- Mettez des gants, et demander au patient de soulever la robe à l’avant. Inspecter la zone du canal inguinal, canal fémoral et scrotum (mâles) de renflements sur les deux côtés.
- Identifier le ligament inguinal, qui s’étend de l’épine iliaque antéro-supérieure à du tubercule pubien. Le canal inguinal est parallèle, entre les anneaux inguinaux internes et externes. La bague intérieure et l’origine des hernies indirectes, est juste supérieur au point médian de l’arcade crurale. L’anneau inguinal externe est légèrement supérieure et latérale de la tubérosité du pubis. Le triangle inguinale et la zone d’origine des hernies directes, est limitée par l’artère épigastrique inférieure latéralement, le ligament inguinal inférieurement et la linea semilunaris médialement. Le canal fémoral se trouve au-dessous de l’arcade crurale juste médiale de la veine fémorale et artère.
- Demandez au patient de tourner la tête sur le côté et toux ou simplement porter vers le bas et continuer à observer pour nouveau bombé ou augmentation de la taille d’un renflement existant.
- Utilisez les touches de doigt de la main droite pour examiner le côté droit et palper sur le canal fémoral, et demandez au patient de tousser ou de porter vers le bas encore une fois d’évaluer pour hernie crurale apparaît. Les hernies fémorales sont plus fréquents chez les femmes et plus susceptibles que les hernies inguinales d’incarcérer.
- Ensuite, palper au-dessus du canal inguinal droit. Demandez au patient de tousser ou de porter vers le bas, puis se sentir pour les bosses. Un renflement en expansion senti vers le milieu de l’arcade crurale est probablement une hernie indirecte. Un renflement senti près le tubercule du pubis est plus probablement une hernie directe.
- Ausculter sur n’importe quel bombements, notant la présence ou l’absence de bruits intestinaux.
- Chez les hommes, si on observe une masse scrotale, palper elle et essayer de palper au-dessus de lui pour le différencier de pathologie testiculaire.
- Si aucune masse n’est encore évident, utiliser l’index de la main droite, avec le tampon de doigt vers le patient, à palper l’anneau inguinal droit externe et le canal inguinal distale en plaçant le doigt sur le scrotum, juste au dessus du testicule droit.
- Invaginent le scrotum, en suivant le cordon spermatique supérieurement et dans le sens du canal inguinal, jusqu'à ce que le doigt se trouve juste après l’anneau inguinal externe. Le cordon spermatique (mâles) et le ligament rond (femelles) traverse le canal inguinal.
- Demandez au patient de tousser ou de porter vers le bas. Un renflement ressenti au bout du doigt peut être une hernie indirecte, alors qu’un feutre sur le côté du doigt peut être une hernie directe. À noter, la capacité du médecin à distinguer les hernies directes et indirectes sur l’examen physique est imprécise.
- Répétez sur le côté gauche avec la main gauche.
- Essayer de réduire doucement tout présumés hernies, évitant la réduction énergique. La réduction est facilitée en ayant le mensonge patient vers le bas en position de Trendelenburg.
Applications et Résumé
Une approche systématique à l’examen d’un patient présentant une douleur abdominale aiguë comprend l’inspection, l’auscultation, percussion et palpation. Manœuvres spéciales pour détecter les abdominaux mur douleur, appendicite, cholécystite, et hernies est souhaitable si l'on soupçonne pour ces processus.
Les conclusions de l’examen les plus utiles pour augmenter la probabilité de la maladie incluent tendresse rigidité et percussions générales péritonite ; De McBurney point de tendresse, de Rovsing positif signe et psoas positive signent pour appendicite ; signe de Murphy positif et du quadrant supérieur droit pour cholécystite ; péristaltisme visible, distension abdominale et des sons de haute pente-hyperactif de l’intestin pour obstruction de l’intestin grêle.
Conclusions qui réduisent la probabilité de la maladie sont d’un Carnett positif signe et douleur négative avec toux générales péritonite ; absence du quadrant inférieur droit de l’appendicite ; en l’absence du quadrant supérieur droit pour cholécystite ; bruits intestinaux normaux et absence de distension abdominale pour obstruction de l’intestin grêle.
Le rendement de l’examen abdominal est beaucoup mieux si le clinicien suscite une histoire efficace, assure une surveillance attentive et estime pertinent de l’anatomie régionale quand liquidienne et palpation. Relation du médecin avec leurs avantages patients d’avoir une approche douce à celui qui est déjà dans la douleur et éviter les manœuvres inutiles qui peuvent augmenter l’inconfort pour le patient sans fournir de nouvelles informations, telles que le critère traditionnel pour rebondir de tendresse, où le médecin palpe profondément au-dessus de la zone de la douleur, puis supprime vigoureusement la main palpating, demandant si la tendresse était pire avec la palpation ou la libération. Une histoire efficace et l’examen physique permettant une utilisation rentable de l’imagerie diagnostique et d’améliorent l’interprétation clinique d’imagerie résultats, ainsi que permettre le triage des patients qui peuvent avoir besoin de chirurgie urgente.
Tags
Passer à...
Vidéos de cette collection:

Now Playing
Examen abdominal IV: Évaluation de la douleur abdominale aiguë
Physical Examinations II
67.3K Vues

Examen des yeux
Physical Examinations II
77.1K Vues

Examen ophtalmologique
Physical Examinations II
67.9K Vues

Examen des oreilles
Physical Examinations II
55.1K Vues

Examen du nez, des sinus, de la cavité orale et du pharynx
Physical Examinations II
65.7K Vues

Examen de la thyroïde
Physical Examinations II
105.0K Vues

Examen des ganglions lymphatiques
Physical Examinations II
387.3K Vues

Examen abdominal I: Inspection et auscultation
Physical Examinations II
202.6K Vues

Examen abdominal II: Percussion
Physical Examinations II
248.2K Vues

Examen abdominal III: Palpation
Physical Examinations II
138.5K Vues

Toucher rectal chez l'homme
Physical Examinations II
114.4K Vues

Examen général des seins
Physical Examinations II
87.6K Vues

Examen pelvien I: Évaluation des organes génitaux externes
Physical Examinations II
306.9K Vues

Examen pelvien: Examen au spéculum
Physical Examinations II
150.4K Vues

Examen pelvien III: Examen bi-manuel et toucher rectal
Physical Examinations II
147.7K Vues
À PROPOS DE JoVE
Copyright © 2025 MyJoVE Corporation. Tous droits réservés.