
Abdominal Exam IV: Acute Abdominal Pain Assessment
Overview
Source: Joseph Donroe, MD, Internal Medicine and Pediatrics, Yale School of Medicine, New Haven, CT
Abdominal pain is a frequent presenting concern in both the emergency department and the office setting. Acute abdominal pain is defined as pain lasting less than seven days, while an acute abdomen refers to the abrupt onset of severe abdominal pain with features suggesting a surgically intervenable process. The differential diagnosis of acute abdominal pain is broad; thus, clinicians must have a systematic method of examination guided by a careful history, remembering that pathology outside of the abdomen can also cause abdominal pain, including pulmonary, cardiac, rectal, and genital disorders.
Terminology for describing the location of abdominal tenderness includes the right and left upper and lower quadrants, and the epigastric, umbilical, and hypogastric regions (Figures 1, 2). Thorough examination requires an organized approach involving inspection, auscultation, percussion, and palpation, with each maneuver performed purposefully and with a clear mental representation of the anatomy. Rather than palpating randomly across the abdomen, begin palpating remotely from the site of tenderness, moving systematically toward the tender region, and thinking about what lies below the fingers at each position. A helpful technique is to imagine a clock face with the xiphoid process at 12:00 and the pubic symphysis at 6:00 (Figure 3). When palpating at 8:00, there is skin, muscle, cecum, appendix, and ureters. Performing the exam in this fashion assists in clinical reasoning and minimizes the chance of missing pathology.
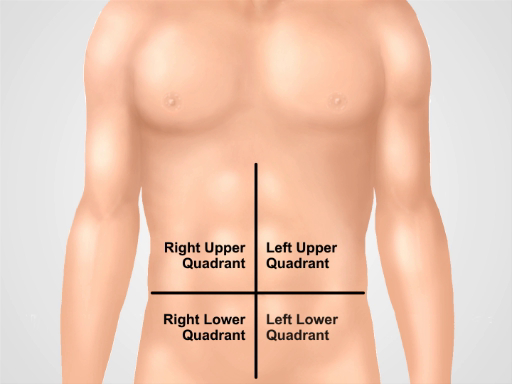
Figure 1. Four abdominal quadrants. Abdomen can be divided into four regions by two imaginary lines intersecting at umbilicus. Right upper quadrant (often designated as RUQ), left upper quadrant (LUQ), right lower quadrant (RLQ), and left lower quadrant (LLQ) are shown.
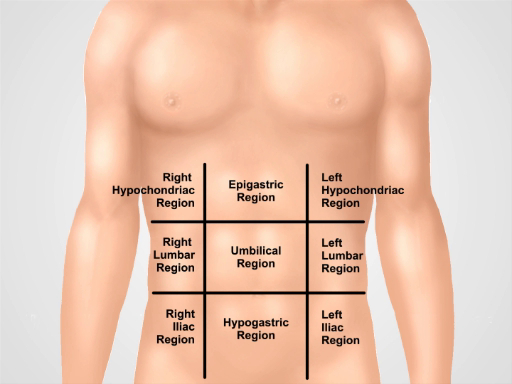
Figure 2. Nine abdominal regions. Midclavicular lines and subcostal and intertubercular planes separate abdomen into nine regions: epigastric region, right hypochondriac region, left hypochondriac region, umbilical region, right lumbar region, left lumbar region, hypogastric region, right inguinal region, and left inguinal region.
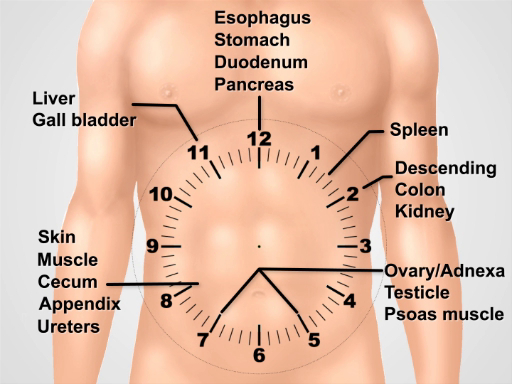
Figure 3. Visualizing a clock face over the abdomen for thinking about the underlying anatomy while performing the exam.
Procedure
1. Preparation
- Wash your hands and warm them prior to examining the patient.
- Have the patient put on a gown. An extra drape is necessary to cover the lower body.
- Begin with the patient lying supine on the exam table or bed.
2. Approach to acute abdominal pain
- Begin with a complete set of vital sign tests.
- After entering the room, immediately begin careful inspection. Patients with peritonitis may prefer to lie still with flexed hips
Application and Summary
A systematic approach to examining a patient with acute abdominal pain includes inspection, auscultation, percussion, and palpation. Special maneuvers to detect abdominal wall pain, appendicitis, cholecystitis, and hernias should be performed if there is suspicion for these processes.
The exam findings that are most useful for increasing the probability of disease include rigidity and percussion tenderness for general peritonitis; McBurney's point tenderness, positive Rovsing's sign, and posit
Tags
Skip to...
Videos from this collection:

Now Playing
Abdominal Exam IV: Acute Abdominal Pain Assessment
Physical Examinations II
67.3K Views

Eye Exam
Physical Examinations II
77.1K Views

Ophthalmoscopic Examination
Physical Examinations II
67.9K Views

Ear Exam
Physical Examinations II
55.1K Views

Nose, Sinuses, Oral Cavity and Pharynx Exam
Physical Examinations II
65.7K Views

Thyroid Exam
Physical Examinations II
105.0K Views

Lymph Node Exam
Physical Examinations II
387.2K Views

Abdominal Exam I: Inspection and Auscultation
Physical Examinations II
202.6K Views

Abdominal Exam II: Percussion
Physical Examinations II
248.1K Views

Abdominal Exam III: Palpation
Physical Examinations II
138.5K Views

Male Rectal Exam
Physical Examinations II
114.4K Views

Comprehensive Breast Exam
Physical Examinations II
87.6K Views

Pelvic Exam I: Assessment of the External Genitalia
Physical Examinations II
306.8K Views

Pelvic Exam II: Speculum Exam
Physical Examinations II
150.3K Views

Pelvic Exam III: Bimanual and Rectovaginal Exam
Physical Examinations II
147.7K Views
Copyright © 2025 MyJoVE Corporation. All rights reserved