
Esame obiettivo dell'addome IV: valutazione del dolore addominale acuto
Panoramica
Fonte: Joseph Donroe, MD, Medicina interna e pediatria, Yale School of Medicine, New Haven, CT
Il dolore addominale è una preoccupazione frequente sia nel pronto soccorso che nell'ufficio. Il dolore addominale acuto è definito come dolore che dura meno di sette giorni, mentre un addome acuto si riferisce all'insorgenza improvvisa di forti dolori addominali con caratteristiche che suggeriscono un processo chirurgicamente interveniente. La diagnosi differenziale del dolore addominale acuto è ampia; pertanto, i medici devono avere un metodo sistematico di esame guidato da un'attenta storia, ricordando che la patologia al di fuori dell'addome può anche causare dolore addominale, compresi disturbi polmonari, cardiaci, rettali e genitali.
La terminologia per descrivere la posizione della tenerezza addominale comprende i quadranti superiore e inferiore destro e sinistro e le regioni epigastrica, ombelicale e ipogastrica (Figure 1, 2). Un esame approfondito richiede un approccio organizzato che coinvolge l'ispezione, l'auscultazione, la percussione e la palpazione, con ogni manovra eseguita intenzionalmente e con una chiara rappresentazione mentale dell'anatomia. Piuttosto che palpare casualmente attraverso l'addome, inizia a palpare a distanza dal sito di tenerezza, muovendoti sistematicamente verso la regione tenera e pensando a cosa si trova sotto le dita in ogni posizione. Una tecnica utile è quella di immaginare un quadrante dell'orologio con il processo xifoide alle 12:00 e la sinfisi pubica alle 6:00 (Figura 3). Quando palpa alle 8:00, c'è pelle, muscoli, cieco, appendice e ureteri. Eseguire l'esame in questo modo aiuta nel ragionamento clinico e riduce al minimo la possibilità di patologia mancante.
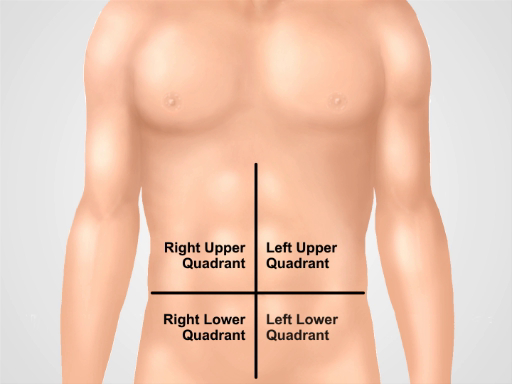
Figura 1. Quattro quadranti addominali. L'addome può essere diviso in quattro regioni da due linee immaginarie che si intersecano all'ombelico. Vengono mostrati il quadrante superiore destro (spesso designato come RUQ), il quadrante superiore sinistro (LUQ), il quadrante inferiore destro (RLQ) e il quadrante inferiore sinistro (LLQ).
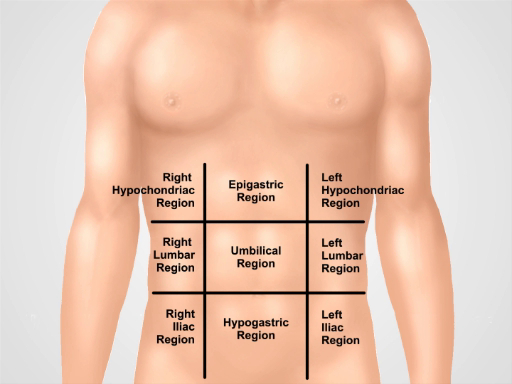
Figura 2. Nove regioni addominali. Le linee medioclavicolari e i piani subcostali e intertubercolari separano l'addome in nove regioni: regione epigastrica, regione ipocondriaca destra, regione ipocondriaca sinistra, regione ombelicale, regione lombare destra, regione lombare sinistra, regione ipogastrica, regione inguinale destra e regione inguinale sinistra.
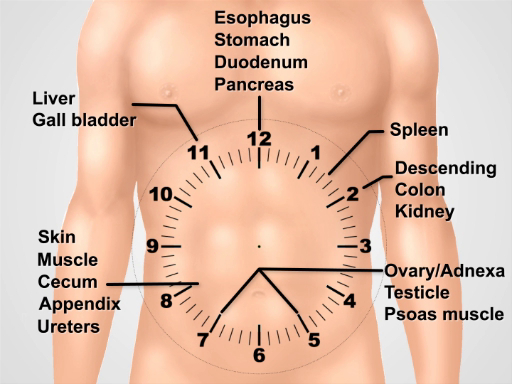
Figura 3. Visualizzare un quadrante dell'orologio sopra l'addome per pensare all'anatomia sottostante durante l'esecuzione dell'esame.
Procedura
1. Preparazione
- Lavarsi le mani e riscaldarle prima di esaminare il paziente.
- Fai indossare al paziente un camice. Un drappo extra è necessario per coprire la parte inferiore del corpo.
- Inizia con il paziente sdraiato supino sul tavolo o sul letto d'esame.
2. Approccio al dolore addominale acuto
- Inizia con una serie completa di test dei segni vitali.
- Dopo essere entrato nella stanza, iniziare immediatamente un'attenta ispezione. I pazienti con peritonite possono preferire stare fermi con fianchi e ginocchia flessi.
- Posizionare un drappo sulla parte inferiore del corpo del paziente fino alla sinfisi pubica e sollevare l'abito appena sotto il seno. Nota distensione addominale, colore della pelle, segni di scarsa perfusione, come chiazze, pulsazioni visibili o peristalsi, rigonfiamenti e cicatrici.
- Se il paziente è vigile, chiedere al paziente di usare un dito per indicare l'area dolorosa. Chiedere al paziente di tossire (test della tosse) o urtare delicatamente il letto, che può localizzare il dolore della peritonite.
- Auscultate il quadrante inferiore sinistro usando il diaframma con una leggera pressione. I suoni intestinali assenti possono indicare un ileo, mentre i suoni acuti suggeriscono un'imminente ostruzione meccanica. L'auscultazione ha la resa più bassa delle manovre diagnostiche per il dolore addominale.
- Auscultate su eventuali aree sporgenti per valutare l'ernia dell'intestino.
- Procedere ad utilizzare la testa dello stetoscopio per palpare i quattro quadranti con pressione graduata, pur continuando ad auscultare. Osservare il viso del paziente per i segni di angoscia e sentire la parete addominale per la rigidità.
- Percuss l'addome, iniziando con percussioni molto leggere (test di percussione leggera) sui quattro quadranti. Questo può localizzare il dolore peritoneale e distinguerlo dal dolore viscerale.
- Continuare con un colpo di percussione moderato nei quattro quadranti, valutando la ricerca di timosa anomalo, suggerendo aria (aria libera o intestino pieno di gas) o ottusità, suggerendo fluido o massa.
- Chiedi al paziente di flettere le gambe ai fianchi e alle ginocchia.
- Inizia la palpazione posizionando delicatamente la mano destra aperta sull'addome con le dita leggermente distese. Utilizzare un leggero movimento a dondolo mentre il paziente respira, sentendo la rigidità della parete addominale. Senti ogni quadrante in questo modo, iniziando più lontano dal sito del dolore. Distrarre il paziente con la conversazione può servire a ridurre al minimo la guardia volontaria.
- Palpare di nuovo usando una pressione moderata con i polpastrelli (non con la punta delle dita), in senso orario. Nel mezzo del quadrante dell'orologio, palpare l'aorta.
- Palpare rigonfiamenti che evocano il sospetto di ernie della parete addominale e tentano di ridurre se presenti.
- In pazienti selezionati, in particolare quelli con dolore al quadrante inferiore o sospetto di sanguinamento gastrointestinale, eseguire un esame rettale.
- Eseguire un esame testicolare su maschi con dolore addominale inferiore.
- Eseguire un esame pelvico su donne con dolore addominale.
3. Manovre speciali in pazienti selezionati con dolore addominale.
- Test per il segno di Murphy in pazienti con dolore al quadrante superiore destro. Palpato nella linea midclavicolare, appena sotto il bordo del fegato.
- Chiedi al paziente di fare un respiro profondo mentre palpi profondamente. Il dolore accompagnato dalla cessazione dell'ispirazione suggerisce colecistite acuta.
- Per il dolore del quadrante inferiore destro, le seguenti manovre possono essere diagnosticamente utili:
- Suscitare il segno di Rovsing con una profonda palpazione del quadrante inferiore sinistro. Il dolore riferito al quadrante inferiore destro suggerisce appendicite acuta.
- Eseguire il segno dell'otturatore flettendo l'anca destra e il ginocchio del paziente a 90 ° e ruotando internamente l'anca. Il dolore nel quadrante inferiore destro suggerisce appendicite acuta o ascesso pelvico.
- Eseguire il segno psoas facendo flettere al paziente la coscia destra contro la mano resistente dell'esaminatore. Il dolore addominale inferiore suggerisce un'appendicite retrocecale o ascesso psoas. Per eseguire un metodo alternativo del segno psoas, posizionare il paziente nella posizione del decubito laterale sinistro e, in piedi dietro il paziente, estendere la coscia del paziente.
- Eseguire il test di Carnett per valutare il dolore alla parete addominale, che può imitare la patologia intra-addominale e spesso non viene diagnosticato. Identificare il punto di dolore massimo nel paziente supino e palpare lì con una pressione moderata per suscitare tenerezza.
- Chiedi al paziente di sollevare le spalle dal letto come se stesse facendo un sit-up, contraendo così i muscoli della parete addominale. L'aumento del dolore suggerisce un dolore alla parete addominale, mentre il dolore migliorato suggerisce una patologia intraperitoneale (ora protetta dai muscoli retti contratti).
- Valutare la splenomegalia in pazienti con dolore al quadrante superiore sinistro o segni di ipertensione portale.
- Valutare l'ascite in pazienti con una storia suggestiva.
- Valutare per le ernie inguinali: le ernie inguinali sintomatiche possono essere presenti con dolore all'inguine, un rigonfiamento non riducibile o segni di ostruzione intestinale, come distensione addominale, dolore e vomito. La valutazione per le ernie inguini deve essere effettuata in pazienti selezionati con disturbi addominali o inguinale inferiori. Chiedi al paziente di stare in piedi, poiché questa è la posizione preferita da valutare per le ernie inguini. Passaggi 3.6.1. - 3.6.4. può anche essere eseguita in posizione supina se il paziente non è in grado di stare in piedi, anche se in questa posizione possono mancare ernie facilmente riducibili.
- Indossa i guanti e chiedi al paziente di sollevare il camice nella parte anteriore. Ispezionare l'area del canale inguinale, del canale femorale e dello scroto (maschi) per rigonfiamenti su entrambi i lati.
- Identificare il legamento inguinale che si estende dalla colonna iliaca superiore anteriore al tubercolo pubico. Il canale inguinale corre parallelo ad esso, tra gli anelli inguinali interni ed esterni. L'anello interno, e l'origine delle ernie indirette, è appena superiore al punto medio del legamento inguinale. L'anello inguinale esterno è leggermente superiore e laterale al tubercolo pubico. Il triangolo inguinale, e l'area di origine delle ernie dirette, è delimitato dall'arteria epigastrica inferiore lateralmente, dal legamento inguinale inferiormente e dalla linea semilunaris medialmente. Il canale femorale si trova sotto il legamento inguinale appena mediale alla vena e all'arteria femorale.
- Chiedi al paziente di girare la testa di lato, e tossire o semplicemente sopportare, e continuare a osservare per nuovo rigonfiamento o aumento delle dimensioni di un rigonfiamento esistente.
- Usando i cuscinetti delle dita della mano destra per esaminare il lato destro, palpare sul canale femorale e chiedere al paziente di tossire o sopportare di nuovo per valutare le ernie femorali. Le ernie femorali sono più comuni nelle donne e più probabilità rispetto alle ernie inguinali di incarcerare.
- Quindi, palpare sul canale inguinale destro. Chiedi al paziente di tossire o sopportare, quindi senti eventuali rigonfiamenti. Un rigonfiamento in espansione sentito verso il punto medio del legamento inguinale è probabilmente un'ernia indiretta. Un rigonfiamento sentito vicino al tubercolo pubico è più probabilmente un'ernia diretta.
- Auscultate su eventuali rigonfiamenti, notando la presenza o l'assenza di suoni intestinali.
- Nei maschi, se si osserva una massa scrotale, palparla e cercare di palparla sopra di essa per differenziarla dalla patologia testicolare.
- Se nessuna massa è ancora evidente, utilizzare l'indice della mano destra, con il polpaccino rivolto verso il paziente, per palpare l'anello inguinale esterno destro e il canale inguinale distale posizionando il dito sullo scroto, appena sopra il testicolo destro.
- Invaginare lo scroto, seguendo il cordone spermatico superiormente e in direzione del canale inguinale fino a quando la punta delle dita è appena oltre l'anello inguinale esterno. Il cordone spermatico (maschi) e il legamento rotondo (femmine) viaggiano attraverso il canale inguinale.
- Chiedi al paziente di tossire o sopportare. Un rigonfiamento sentito sulla punta delle dita può essere un'ernia indiretta, mentre uno sentito sul lato del dito può essere un'ernia diretta. Da notare, la capacità del medico di distinguere tra ernie dirette e indirette all'esame fisico è imprecisa.
- Ripeti sul lato sinistro usando la mano sinistra.
- Tentare di ridurre delicatamente eventuali ernie sospette, evitando una riduzione forzata. La riduzione è facilitata dal fatto che il paziente si sdrai nella posizione di Trendelenburg.
Applicazione e Riepilogo
Un approccio sistematico all'esame di un paziente con dolore addominale acuto include ispezione, auscultazione, percussione e palpazione. Manovre speciali per rilevare dolore alla parete addominale, appendicite, colecistite ed ernie dovrebbero essere eseguite se vi è sospetto per questi processi.
I risultati dell'esame che sono più utili per aumentare la probabilità di malattia includono rigidità e tenerezza delle percussioni per la peritonite generale; La tenerezza del punto di McBurney, il segno di Rovsing positivo e il segno di psoas positivo per l'appendicite; segno di Murphy positivo e tenerezza del quadrante superiore destro per colecistite; peristalsi visibile, distensione addominale e suoni intestinali iperattivi acuti per l'ostruzione dell'intestino tenue.
I risultati che diminuiscono la probabilità di malattia sono un segno di Carnett positivo e dolore negativo con tosse per peritonite generale; assenza di tenerezza del quadrante inferiore destro per appendicite; tenerezza del quadrante superiore destro assente per colecistite; suoni intestinali normali e assenza di distensione addominale per ostruzione dell'intestino tenue.
La resa dell'esame addominale è molto migliore se il clinico suscita una storia efficace, esegue un'attenta ispezione e considera l'anatomia regionale pertinente durante la percussione e la palpazione. La relazione del medico con il proprio paziente trae beneficio dall'avere un approccio gentile a chi è già nel dolore ed evitare manovre inutili che possono aumentare il disagio del paziente senza fornire nuove informazioni, come il tradizionale test per la tenerezza del rimbalzo, in cui il medico palpa profondamente sopra l'area del dolore e poi rimuove rapidamente la mano palpante, chiedendo se la tenerezza fosse peggiore con la palpazione o il rilascio. Un'efficace aurea e un esame fisico consentono un utilizzo economico dell'imaging diagnostico e migliorano l'interpretazione clinica dei risultati dell'imaging, oltre a consentire il triage dei pazienti che potrebbero aver bisogno di un intervento chirurgico urgente.
Tags
Vai a...
Video da questa raccolta:

Now Playing
Esame obiettivo dell'addome IV: valutazione del dolore addominale acuto
Physical Examinations II
67.3K Visualizzazioni

Esame obiettivo dell'occhio
Physical Examinations II
77.1K Visualizzazioni

Esame oftalmoscopico
Physical Examinations II
67.9K Visualizzazioni

Esame obiettivo dell'orecchio
Physical Examinations II
55.1K Visualizzazioni

Esame di naso, seni, cavità orale e faringe
Physical Examinations II
65.7K Visualizzazioni

Esame obiettivo della tiroide
Physical Examinations II
105.0K Visualizzazioni

Esame obiettivo dei linfonodi
Physical Examinations II
387.3K Visualizzazioni

Esame obiettivo dell'addome I: ispezione e auscultazione
Physical Examinations II
202.6K Visualizzazioni

Esame obiettivo dell'addome II: percussione
Physical Examinations II
248.2K Visualizzazioni

Esame obiettivo dell'addome III: palpazione
Physical Examinations II
138.5K Visualizzazioni

Esame rettale maschile
Physical Examinations II
114.4K Visualizzazioni

Esame completo del seno
Physical Examinations II
87.6K Visualizzazioni

Esame obiettivo ginecologico I: valutazione dei genitali esterni
Physical Examinations II
306.9K Visualizzazioni

Esame obiettivo ginecologico II: esame con lo speculum
Physical Examinations II
150.4K Visualizzazioni

Esame obiettivo ginecologico III: palpazione rettovaginale e bimanuale
Physical Examinations II
147.7K Visualizzazioni
Personale delle biblioteche
Copyright © 2025 MyJoVE Corporation. Tutti i diritti riservati