
Method Article
ブタモデルにおける異自家腎移植:ステップバイステップのプロトコル
要約
Porcine models of organ transplantation provide an important platform to study mechanisms of organ preservation. This article describes a heterotopic porcine renal autotransplantation model, which allows investigating new approaches to improve the outcome of transplantation using marginal kidney grafts.
要約
Kidney transplantation is the treatment of choice for patients suffering from end-stage renal disease. It offers better life expectancy and higher quality of life when compared to dialysis. Although the last few decades have seen major improvements in patient outcomes following kidney transplantation, the increasing shortage of available organs represents a severe problem worldwide. To expand the donor pool, marginal kidney grafts recovered from extended criteria donors (ECD) or donated after circulatory death (DCD) are now accepted for transplantation. To further improve the postoperative outcome of these marginal grafts, research must focus on new therapeutic approaches such as alternative preservation techniques, immunomodulation, gene transfer, and stem cell administration.
Experimental studies in animal models are the final step before newly developed techniques can be translated into clinical practice. Porcine kidney transplantation is an excellent model of human transplantation and allows investigation of novel approaches. The major advantage of the porcine model is its anatomical and physiological similarity to the human body, which facilitates the rapid translation of new findings to clinical trials. This article offers a surgical step-by-step protocol for an autotransplantation model and highlights key factors to ensure experimental success. Adequate pre- and postoperative housing, attentive anesthesia, and consistent surgical techniques result in favorable postoperative outcomes. Resection of the contralateral native kidney provides the opportunity to assess post-transplant graft function. The placement of venous and urinary catheters and the use of metabolic cages allow further detailed evaluation. For long-term follow-up studies and investigation of alternative graft preservation techniques, autotransplantation models are superior to allotransplantation models, as they avoid the confounding bias posed by rejection and immunosuppressive medication.
概要
Kidney transplantation is the treatment of choice for patients with end-stage renal disease, due to associated lower rates of morbidity and mortality when compared to dialysis 1-3. Despite major improvements in patient outcomes following kidney transplantation, graft shortage still poses a severe challenge worldwide. The number of patients waiting for a kidney transplant by far exceeds the number of organs available 4-6. To increase the number of kidneys available for transplantation and to reduce patient waiting times, further sources of kidney grafts are needed.
Commonly, standard criteria donor (SCD) and extended criteria donor (ECD) kidney grafts from donation after brain death (DBD) as well as kidneys recovered from live donors (LDKT) are utilized. Since the 1990s, an increasing number of kidney grafts have been recovered in a donation after circulatory death (DCD) scenario, to further expand the donor pool 7,8. However, DCD and ECD kidney grafts demonstrate acceptable but decreased outcomes after transplantation, depending on different factors, such as donor age, warm and cold ischemia times, and the preservation technique used 9-11. Thus, additional research is required to improve the outcome of patients receiving marginal kidney grafts and to further increase the donor pool.
The porcine model of renal transplantation is well established and provides a clinical important scenario to investigate innovative approaches for the improvement of marginal kidney graft outcomes. In contrast to rodent and canine kidneys, which are unilobular, porcine and human kidneys are multilobular and are anatomically similar, particularly in regard to the arterial, venous, and urinary collecting systems 12,13. In addition, porcine and human kidneys demonstrate similarities in the pathophysiology of ischemia reperfusion injury (IRI), biochemistry, and immunological parameters 14. Thus, porcine renal transplantation is well-suited to investigate new organ preservation methods for marginal kidney grafts 15-17, model human IRI 18, study immunological pathways and allograft tolerance 19, provide surgical training 20-22, test new pharmacological therapies 23, implement new medical devices, and study new immunological mechanisms in xenotransplantation 24-26.
The renal porcine and human transplantation settings are not completely analogous. This article focuses on important technical details that will facilitate successful establishment of a renal autotransplantation model. Species-adapted pre- and postoperative housing, administration of anesthesia with close monitoring, and matched surgical techniques are described in the protocol and demonstrated in the video. Resection of the contralateral native kidney provides the opportunity to assess the function of the transplanted kidney. The placement of venous and urinary catheters and the use of metabolic cages allow more in-depth assessment. For studies aimed at investigating alternative graft preservation methods and mechanisms of IRI, autotransplantation models are superior to allotransplantation models, as they avoid the complications and confounding bias associated with rejection and use of immunosuppressive medications.
プロトコル
すべての動物は、人道的なケアを受け、すべての研究私たちは動物管理上のカナダの評議会の方針やガイドラインに従って行います。すべての手順は、大学健康ネットワーク施設内動物管理委員会によって承認された動物の使用プロトコル下で行いました。
注:試験プロトコールの概略を図1に示されています。

図1.研究プロトコル。 この図の拡大版をご覧になるにはこちらをクリックしてください。
{kind=link}
1.動物
- このプロトコルで男性のヨークシャーブタ(30キロ)を使用します。
2.腎移植検索
- 術前の手順
- ハウスオスYorkshirそれらを慣らすために、少なくとも1週間のための研究施設での電子豚。 ストレプトコッカス・スイス(Streptococcus suis)やサルモネラ菌による感染の潜在的なリスクを軽減するために3日間、このようなセフチオフルとして、第三世代セファロスポリンの筋肉内注射を使用してください。誤嚥を防ぐために麻酔の導入前に、6時間の最小値のための豚を速いです。
- ケタミン(20 mgの/ kg)を、アトロピン(0.04ミリグラム/キログラム)、及びミダゾラム(0.3ミリグラム/キログラム)の筋肉内注射により豚の麻酔を開始します。その後、手術室(OR)に収容施設から動物を輸送します。
- ORのテーブルの上に仰臥位で豚を置きます。豚が自発的にイソフルランの5%と酸素の2 Lを呼吸することを可能にします。喉頭鏡で声帯を公開し、挿管誘発性喉頭痙攣を防ぐために2%リドカイン局所用溶液でそれらをスプレー。 6.5ミリメートル管と挿管後、空気3〜5 mlのカフをブロックします。
注:カプノメトリが正しいpositioを確認します気管チューブのn個。 - 2.5パーセントにイソフルランガスを減少させます。 14-16呼吸/分、10〜15ミリリットル/ kg体重一回換気量に人工呼吸器を設定します。密接に豚を監視します。心拍数および酸素飽和度は、パルスオキシメトリによって記録されます。減少した(150拍/分以下)心拍数と血圧(100 mmHgの収縮期値以下)だけでなく、ブタの動きの欠如(筋弛緩剤の無使用)により、適切な麻酔を確認してください。
- 無菌条件下で、9.5神父を紹介セルジンガー法27を用いて、内頸静脈へのシングルルーメン永久カテーテル。簡単に言えば、静脈を穿刺するために針を使用しています。ガイドワイヤを導入した後、血管カテーテルとワイヤの交換が続くピールアウェイイントロデューサ針を交換してください。 3-0シルクまたは非吸収性モノフィラメント縫合糸を使用して皮膚にカテーテルを修正しました。
- メトロニダゾール500mgの、セファゾリンの1グラム、およびパントプラゾール20mgを投与します。広告大臣5%デキストロース(D5W)および静脈内手術を通して、毎時1ミリリットルのフェンタニルクエン酸と乳酸リンゲル液の200ミリリットル。麻酔下ながら乾燥を防ぐために、目に獣医の眼軟膏を適用します。
- 外科手術
- 滅菌消毒や手術野の報道に続いて、長さ25cmの正中切開を行います。開創器を挿入します。タオルで大小の腸を覆い、右の腎臓への最適なアクセスのために左側にそれらを配置します。
- 焼灼を使用して、任意の付着組織から尿管と右腎自身を解放します。
- 下大静脈と大動脈からその起源までメスを使用して、右腎静脈と動脈を解剖、それぞれ、自由です。動脈血管攣縮を回避するために、パパベリンの30〜65 mgの投与を考慮すべきです。
- 完全な腎解剖、ネクタイ(シルク、3-0)の後および遠位尿管を切りました。 Prepar氷のEAボウルと滅菌オルガンバッグ。
- まず、血管クランプを使用して、大静脈に近い腎静脈をクランプ、大動脈および第二の近くに腎動脈をクランプします。次に、腎臓移植片を切除し、直ちに腎動脈カニューレと腎動脈にカニューレを挿入。血液を洗い流すために氷のように冷たいヒスチジン - トリプトファン - ケトグルタル酸(HTK)溶液500mlを使用してください。移植まで氷上に腎臓を保管してください。
- その場では 、結紮糸(絹、2-0)と連続縫合(プロレン、6-0)で腎静脈と残りの腎動脈を閉じます。
- 出血のための解剖エリアを確認した後、実行している縫合糸(モノフィラメント、1)及び3-0絹または非吸収性モノフィラメント縫合糸で皮膚と腹壁を閉じます..
- 術後の手順
- それは、不要な操作を防止するために、豚の背中に静脈カテーテルの縫合糸(絹、3-0)を皮下トンネルを修正しました。発生しやすい豚を配置した後、Suture(シルク、3-0)皮膚にしっかりとカテーテル。
- 人工呼吸器から豚を離乳させると、それは抜管後の住宅地で回復しましょう。体積膨張のために静脈内に乳酸リンゲル液を投与し、鎮痛のために0.3 mgのブプレノルフィンを管理します。それは胸骨横臥位を維持するのに十分な意識を取り戻したまで無人の動物を放置しないでください。
3.腎移植移植
- 術前の手順
- 50-100ミリグラム/時間の速度でプロポフォールの連続注入に続いて、プロポフォールの静脈内注射(1-2 mg / kg体重)を使用して豚を麻酔。ステップ2.1.3と2.1.4で説明したように豚を再挿管と3から4パーセントにイソフルランガスを設定します。
- 2.1.4に記載したのと同じ麻酔プロトコルを使用し、手術の間、セファゾリン1g及びパントプラゾールIV 20mgを投与します。
- 滅菌消毒した後、気管の横4センチメートルのカットを行います。 TIを解剖頸動脈を露出させるssue。動脈の周りにオーバーホルト鉗子や絹のネクタイ(2-0)を渡します。継続的に手術全体の動脈圧を測定するためにプラスチック製のカテーテルを導入するためにセルジンガー法を使用してください。あるいは、非侵襲的な血圧測定技術を利用することができます。
- 外科手術
- 滅菌消毒した後、皮膚および筋膜縫合糸のステッチを切断することにより腹腔を再度開き、腹腔を露出させ、そして腎臓下の血管へのより良いアクセスを許可するように左側に腸を再配置する手術用開創を再導入。
- 腎臓下の大静脈と大動脈に保存腎移植端側を移植。したがって、5-8以上のcmのピックアップや焼灼を使用して、腸骨分岐の上大静脈と大動脈を解剖。可能な場合は、リンパ管を邪魔しません。可能でない場合は、5-0プロレン縫合糸でそれらを閉じます。
- 解剖を完了した後、foをチェック出血Rおよび血管から残りの組織を除去します。 Satinskyクランプと大静脈と大動脈の完全なクランプが実現可能であることを確認してください。
- 次に、対側(左)の腎臓を切除。これを行うには、右に腸を配置。尿管、腎臓自体、腎静脈、および付着組織から腎動脈を解剖。尿管や血管を結ぶと腎臓を切除。出血を確認してください。
- 腎臓下の大動脈と大静脈を露出するために左に腸を再配置します。ヘパリン(100 IU / kg体重)を注入し、少なくとも2分間待ちます。
- 静脈吻合:
- 完全に大静脈をクランプし、11ブレードを用いて、腎静脈の開口部の大きさに一致するスリット切開を作るためにSatinskyクランプを使用してください。ポットのはさみは、さらにスリットを拡張するために使用することができます。
- 無菌の氷を含ませた布に腎臓をラッピングした後、氷からそれを削除し、手術野にそれを配置します。 2重武装6-0を使用します頭蓋と尾コーナーステッチを実行するためのプロレン縫合糸。
- 腎臓を近似、上部コーナーを結ぶと6-0プロレンを使用して、実行中の縫合を行い、後壁から始まります。 2/3を終えた後、前方側に縫合糸を完了するために、タイのもう一方の端を使用します。頭蓋ステッチを結ぶ後、尾コーナーで縫い目を結びます。
- 腎静脈上のブルドッグクランプを置き、Satinskyクランプを開きます。出血のための吻合を確認してください。
- 動脈吻合:
- Satinskyが完全に大動脈をクランプするために、再度クランプを使用します。腎動脈の開口部に一致する、スリットの切開を作るために11ブレードを使用してください。きれいな開口部を確保するために4.0ミリメートルラウンドパンチを使用してください。
- 受信者側で開始する、動脈吻合を実行するために、1つ6-0プロレン縫合糸を使用してください。動脈内皮は解剖を防止するために、各縫合糸に含まれていることを確認してください。一方、norepinephr 10ミリリットルの持続点滴を開始INE(16ミリグラム/ 250ミリリットル)は乳酸リンゲル液500mlに希釈し、100 mmHgの上記の収縮期血圧を維持するために滴定します。
- 動脈吻合が完了する前に、ベラパミル動脈内に注入し、血管攣縮を防止するために、容器の外側に局所パパベリンを投与します。
- 腎動脈上のブルドッグクランプを置き、Satinksyクランプを開きます。出血のための吻合を確認してください。
- 布から腎臓のラップを解除し、氷を取り除きます。動脈ブルドッグクランプ続いて、最初の静脈ブルドッグクランプを開きます。再灌流後、尿産生はすぐに開始する必要があります。
- 移植移植のための有利な位置を確保し、均質な再灌流を維持するために布を使用してください。
- 尿管吻合:
- 移植片から尿管および0.5センチ縦の長さにわたって受信者を開くには、ポットのはさみを使用してください。
- 横方向のUREのための2つの6.0のポリエステル、ポリ(p-ジオキサノン)縫合糸を使用してくださいテラル吻合。前壁に続いて、最初に連続的に後ろの壁を実行し、各側のコーナーシュティッヒを実行します。
- 出血を確認した後、布を取り外し、位置に保持するために腎臓の周りに小腸の一部を包みます。 2モノフィラメント1縫合糸で腹壁を閉じます。 3-0シルクまたは非吸収性モノフィラメント縫合糸で皮膚を閉じます。
- 豚が発生しやすい位置に配置されたまで慎重にノルエピネフリンの注入を滴定することによって連続的に100 mmHgの上記の収縮期血圧を維持します。
- 術後の手順
- 前述したように腹部の閉鎖後、豚加熱パッドと熱循環毛布を使用して温めておきます。 、動脈ラインを取り外し6-0プロレンシュティッヒと動脈に穿刺孔を閉じ、切開部位を閉じます。
- 、腹臥位に豚を回しノルエピネフリン点滴を停止し、人工呼吸器から豚を離乳させます。アル手順からのスムーズな回復を確実にするために、その住宅地に回復し、密接にそれを監視する低豚。移植された頸静脈カテーテルを介して血液ガスサンプルを各時間を取ります。代替ボリュームに乳酸リンゲル液を提供し、鎮痛のために0.3 mgのブプレノルフィンを投与します。
- 自然に飲むことができるようになるまで抜管後、密接に豚を監視します。それは胸骨横臥位を維持するのに十分な意識を取り戻したまで無人の動物を放置しないでください。完全に回復するまで、他の動物の会社に手術を受けた動物を返さないでください。
4.術後フォローアップ
- 必要に応じて、少なくとも2日後に手術以上0.3ミリグラムのブプレノルフィン静脈ごとに8時間を管理します。日常的に手術中に抗生物質の単予防的用量を投与。感染の徴候が発生した場合、1日に1回、昼とメトロニダゾールIV二回までセファゾリン1グラムIVを管理します臨床症状の改善が発生します。豚は十分な水を飲むまで、乳酸リンゲルを管理します。千IUヘパリンは、凝固を防ぐために、カテーテルをロックするために使用することができます。
- 豚の臨床症状や腎機能を評価するために頸静脈カテーテルと尿のサンプルを介して、静脈血サンプルを採取します。
- 安楽死のために、プロポフォール静脈(5〜10 ml)で豚の麻酔を誘導し、イソフルラン5%でそれを維持します。上記のように豚を挿管。 relaparatomyおよび腎組織サンプル採取後、40 mvalのKClの静脈内注射により心停止を引き起こします。
結果
以下では、腎臓の自己移植実験の結果は、(N = 4)で示されます。初期グラフト検索した後、豚は彼らの住宅地で回収されました。また、腎臓移植片は7時間35分(±18分)の平均時間氷上で保存しました。麻酔と繰り返し開腹の再寛解導入後、反対側の腎臓を切除し、説明したように、冷間保存された移植片はheterotopically移植しました。 ( 図1参照)は 、人工呼吸器から離乳後、ブタを手術から回復させ、10日まで続きます。毎日の(1-4術後日; POD)または一日おきに(6-10ポッド)血液試料を血液ガス分析を行うために収集しました。腎機能を評価するために、血清クレアチニンおよび血中尿素窒素(BUN)の値を推定しました。比較のために、あるallotransplanted腎臓移植の結果を示します。免疫抑制のために、この豚はシクロスポリン100mgの経口および共同受信しましたrtisone 250 mgを使用する外科技術は、自家移植プロトコルと同じであったivbid。何の暖かい虚血時間が適用されませんでした。
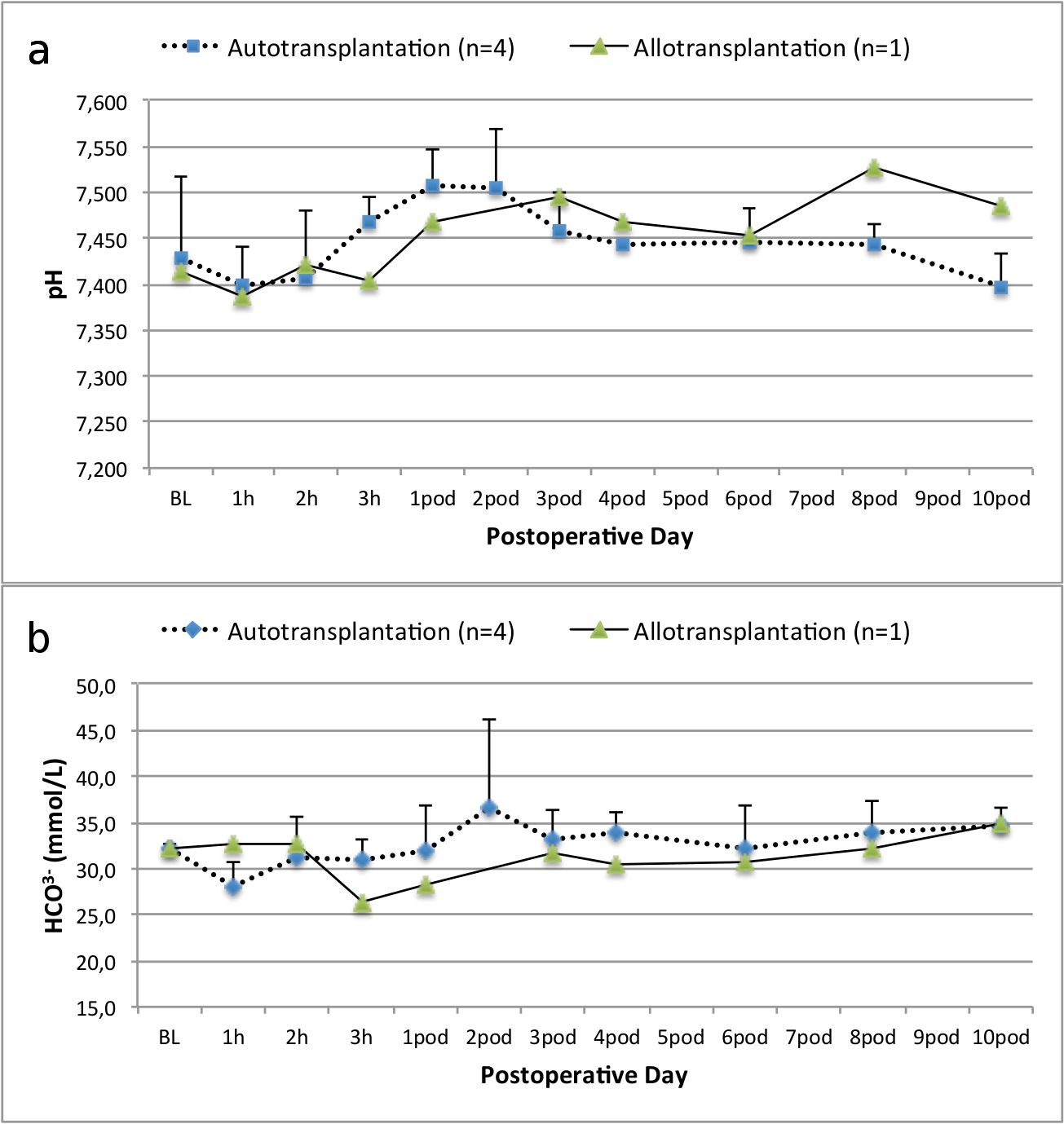
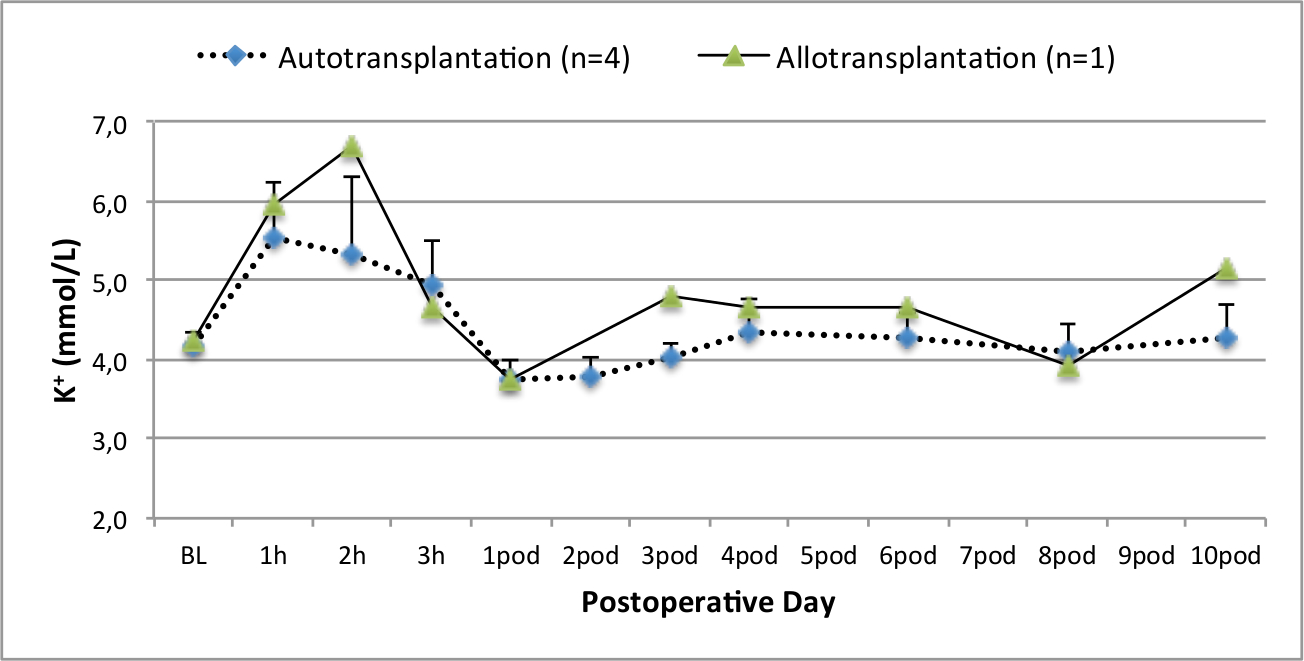
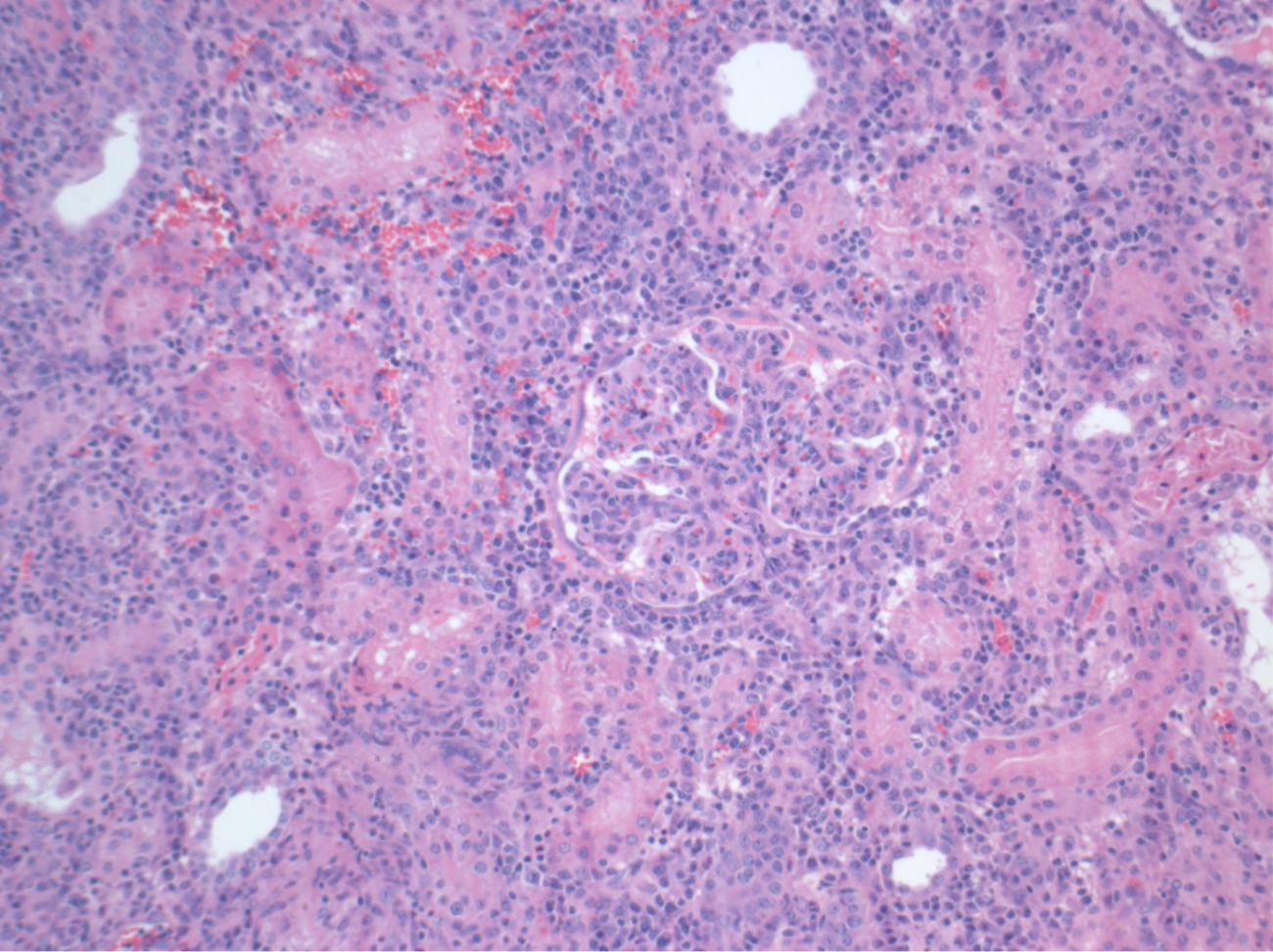
全てのブタは、フォローアップ期間の間に良好な臨床状態にありました。クレアチニンとBUN値は手術後一日目で最大の増加を明らかにした血清(クレア2.8±0.7ミリグラム/ dlで、BUN 25.3±7mgの/ DL)とポッド10(クレア1.7±0.4ミリグラム/ dlで、BUN 10.7±4まで減少しました初期ベースライン値に近いミリグラム/デシリットル)。拒絶反応の可能性が最も高い自家移植、( 図2および3)と比較した場合、allotransplanted腎臓移植片は、良好な初期移植片機能の後に、より高いクレアチニンとBUN値を示しました。酸塩基止血( 図4)及び電解質レベル( 図5)の介入なしに安定でした。組織学的検査は、自家移植、腎臓(Figurに保存尿細管間質を示しました。E 6)、およびallotransplanted腎臓で間質性炎症、尿細管炎、及び糸球体炎を拡散( 図7)。

ベースラインおよび術後10 図 2. 血清クレアチニン値を。血清クレアチニン値(平均値と標準偏差)。 この図の拡大版をご覧になるにはこちらをクリックしてください。
{kind=link}

図3.血清BUN値。ベースラインの血清BUN値(平均値と標準偏差)と10日手術後。 この図の拡大版をご覧になるにはこちらをクリックしてください。
{kind=link}
:FO "jove_content」 
図4.酸塩基止血。ベースラインの酸塩基止血(平均と標準偏差)と10日手術後。 この図の拡大版をご覧になるにはこちらをクリックしてください。
{kind=link}

図5.電解質レベル。電解質レベル(平均値と標準偏差)は、ベースラインおよび10日手術後。 この図の拡大版をご覧になるにはこちらをクリックしてください。
{kind=link}

図6.組織学(H& 10日手術後の自家移植腎臓におけるE)、100X倍率ノーマル尿細管間質。 この図の拡大版をご覧になるにはこちらをクリックしてください。
{kind=link}

図7.組織学(H&E)、100X倍率。豊富な間質性炎症、尿細管炎、及び糸球体炎、拒絶反応と一致して、10日手術後allotransplanted腎臓で。 この図の拡大版をご覧になるにはこちらをクリックしてください。
{kind=link}
ディスカッション
ブタ腎臓移植のモデルは、人間の外科の面で類似性に起因する移植、生理学、生化学、および免疫学14の分野を促進するユニークな機会を提供します。
実験的研究の目的に応じて、腎臓の自己移植のモデルは、同種移植モデルと比較していくつかの利点を有します。いくつかのグループは、同種移植28後に良好な腎移植片機能を報告しているが、ブタの免疫抑制は、特に腎移植では、困難です。術前の血液サンプルは、ブタ白血球抗原(SLA)との互換性を確保するために分析可能であるが、高価であり、実用的でない14。術後、このようなタクロリムスおよびシクロスポリン(カルシニューリン阻害剤、CNI)などの提案の免疫抑制剤は、経口投与または静脈28されています。豚は通常、経口MEDICAを飲み込むことを拒否するように経口投与は、非現実的でする。また、腸の障害物は、免疫抑制薬や治療薬のレベルの維持の十分な吸収を回避することがあります。アクティブな動物におけるCNIのIVの連続注入は、技術的に厳しいです。 IVボーラス投与が毒性を引き起こす高いピーク値をもたらします。したがって、新たな保存技術の調査のために、腎臓の自己移植のモデルはいくつかの利点を有します。上記の実証allotransplantated腎臓移植、クレアチニン及びBUNの遅延と増加したピークの代表的な結果では組織学的評価によって実証された拒絶反応を、示しています。
自家移植のブタモデルは、以前に新しい保存技術14,18,29を調査するために使用されてきました。しかし、心臓の拍動シナリオにおける自家移植豚の報告術後の血清クレアチニンとBUN値はかなり実験系22,30によって異なります。私たちはここに提示心臓鼓動ドナープロトコルは2.8ミリグラム/デシリットル(±0.7)及び(7.4±)25.3ミリグラム/ dlでのBUNピークの低術後の血清クレアチニンピークになります。これらの結果は、Hantoや同僚28とSnoeijsや同僚31によって提示された低ピーク値と同等です。
ブタの自家移植モデルにおける腎移植後の成功した結果を確実にするために、我々はある種の合併症の割合を最小限に抑えるいくつかの重要な技術的な要因を同定しました。ウィスコンシン大学(UW)ソリューションと比較すると、ヒスチジン - トリプトファン - ケトグルタル酸溶液(HTK)の使用は、カリウムのその下の内容に血管攣縮のリスクを低減します。さらに、再灌流の時点で血管痙攣のリスクを減少させるために、ベラパミルは、腎動脈に注入することができ、パパベリン、検索中および再灌流後に局所的に投与することができます。また、ノルエピネフリンの連続点滴を維持するために滴定100 mmHgの上記の収縮期血圧は、均質な再灌流を保証します。ブタの傾向に配置される少なくともまで、この血圧を維持するのに有用です。さらに、移植された移植片の位置決めは、新たに吻合血管のねじれを防止することが重要です。したがって、前に大規模な機械的操作を回避するために、グラフトの吻合を縫製に反対側の左腎臓を切除すると便利です。尿管吻合を終えた後、移植された移植片の周りに小腸をラッピングすることは腹壁の閉鎖後にその位置を確保しています。そのような腸のねじれによる腸閉塞などの合併症はほとんど観察されないが、腸閉塞、腸穿孔、および死亡を含む重篤な合併症につながることができます。良好な臨床転帰および移植片機能を確保フォローアップ中に全体的に、正確な手術手技、気配り麻酔と綿密なモニタリング。
動脈と静脈吻合をperfoすることができます異なる技術を使用してrmed。移植片の同所配置は、腎動脈と静脈のエンドツーエンドの吻合を可能にします。異移植の場合、移植片は、腸骨血管へのエンドツーエンドの吻合のための反対側の腎臓窩、直接遠位大動脈に配置することができます。吻合を有する異移植大動脈すると、それは血栓症および血管痙攣32のリスクを減らすことができるように静脈直接エンド・ツー・サイド手法でこのモデルにおいて好ましいです。非常に初期の静脈分岐部との解剖学的バリエーションは、2つの別々の静脈吻合を縫製の必要性につながる可能性があります。動脈または静脈が比較的短い場合、移植片は、血管の長さを得るために180°回転させることができます。尿管側側吻合は、狭窄または尿漏れを複雑にすることなく、良好な実験結果を得ることができます。
一般的には、腎移植のブタモデルは、他の動物モデルと比べて利点を提供しています。 dと上記の傍接した、特定の類似点は、ブタおよび臨床診療への新技術の比較的高速な翻訳を可能にする人間の設定、間に存在します。移植の技術は、げっ歯類モデルに比べて技術的に容易です。さらに、静脈カテーテルの配置によって、末梢血サンプルを容易に収集することができ、さらなる調査のために処理しました。尿の採取は、腎臓損傷および機能のさらなる評価を可能にします。尿サンプルを採取するために、経皮的カテーテルを膀胱に挿入することができます。豚による操作を回避するために、遠位端は、動物の背中の皮下にトンネルされるべきです。尿収集のための別のオプションは、長期の収集期間は、尿中のクレアチニンクリアランスおよびさらなるバイオマーカーの濃度を推定することを可能にする代謝ケージの使用です。超音波検査、CTスキャン、MRI画像が可能です。循環死のプロトコル後の寄付は暖かい適用することによって模倣することができます前の検索に虚血。また、豚は彼らの攻撃的な行動を制限する去勢場合は取り扱いが比較的容易です。
欠点は、動物の購入、住宅、外科手術などの医療機器、および労働力の高いコストが含まれます。これらの要因は、各試験群の動物の多数を含むことが不可能であることを意味します。また、げっ歯類モデルに比べて、参照の限られた数は、豚規範的、生物学的データについての文献で入手可能です。このような新規保存方法などの新開発技術の評価のための代替として、他のグループは、腎移植33,34の代替として正常体温ex vivoでの再灌流を記載しています。この技術は、実行するのが容易かつ安価です。しかし、標準化された腎臓移植片移植は臨床診療へのより多くの同様のモデルを提供し、長い期間をフォローアップできます。したがって、それは評価するより現実的な移植のために提供していますメント。
結論として、異自家腎移植のブタモデルは、腎臓移植の成果の改善のための革新的な新たなアプローチを調査する臨床の重要なシナリオを提供します。具体的には、このプロトコルは、自家腎移植モデルの成功確立を容易にする重要な技術的な詳細を提供していますし、臨床試験への新たな知見の迅速な翻訳を可能にします。
開示事項
The authors have nothing to disclose.
謝辞
We thank the Sorin Group (Milano, Italy), XVIVO Perfusion Inc. (Goteborg, Sweden), and Braun AG (Melsungen, Germany) for their support. We highly appreciate the support of the John David and Signy Eaton Foundation.
資料
| Name | Company | Catalog Number | Comments |
| Anesthesia Equipment | |||
| Anesthesia Machine, Optimax | Moduflex Anesthesia Equipment | SN5180 | |
| Infusion Pump 3,000 | SIMS Graseby LTD. | SN300050447 | |
| Infusion Pump Line | Smith Medical ASD Inc. | 21-0442-25 | |
| Intravenous permanent catheter (9.5 Fr) | Cook Medical Company | G01865 | |
| Isoflurane Vapor 19.1 | Draeger Medical Canada Inc. | N/A | |
| Mallinckrodt, Tracheal Tube, 6.5 mm | Covidien Canada | 86449 | |
| Temperature Therapy Pad | Gaymar Industries Inc | TP26E | |
| Ventilator, AV 800 | DRE Medical Equipment | 40800AVV | |
| Warm Touch, Patient Warming System | Nellcor/ Covidien Canada | 5015300A | |
| Name | Company | Catalog Number | Comments |
| Surgical Equipment | |||
| Abdominal Retractor | Medite GmbH | 07-0001-00 | |
| Aorta/vein punch 4.0 mm, round | Scanlan International Inc. | 1001-602 | |
| De Bakey, Atraumatic Peripheral, Clamp | Aesculap Inc. | FB463R | |
| De Bakey-Beck, Atraumatic Vena Cava, Clamp | Aesculap Inc. | FB519R | |
| De Bakey, Atraumatic Mini-Bulldog, Straight | Aesculap Inc. | FB422R | |
| De Bakey, Atraumatic Mini-Bulldog, Curved | Aesculap Inc. | FB423R | |
| De Bakey, Atraumatic Coarctation Clamp, Angled | Aesculap Inc. | FB453R | |
| Dissection Blade #11 | Feather Safety Razor Co. | 089165B | |
| Connector (1/4") with male luer lock | Sorin Group Inc. | AB1452 | |
| Liver Admin Set (flush line) | CardioMed Supplies Inc | 17175 | |
| Maxon, 1 | Covidien Canada | 606173 | |
| Med-Rx Suction Connecting Tube | Benlan Inc. | 70-8120 | |
| Organ Bag | CardioMed Supplies Inc | 2990 | |
| Potts – De Martel, Scissors | Aesculap Inc. | BC648R | |
| Renal artery cannula, 1.6" | Sorin Group Inc. | VC-11000 | |
| Sofsilk, 2-0 | Covidien Canada | S405 | |
| Sofsilk, 3-0 | Covidien Canada | S404 | |
| Satinsky, Suprahepatic Cava Clamp | Aesculap Inc. | FB605R | |
| Suction Tip | Tyco Healthcare Group LP | 8888501023 | |
| Surgipro II, 6-0 | Covidien Canada | VP733X | |
| Valleylab, Cautery Pencil | Covidien Canada | E2515H | |
| Valleylab, Force Tx | Valleylab Inc. | 216151480 | |
| Valleylab, Patient Return Electrode | Covidien Canada | E7507 | |
| Name | Company | Catalog Number | Comments |
| Medication | |||
| Atropine Sulfate 15 mg/30 ml | Rafter 8 Products | 238481 | |
| Buprenorphine 0.3 mg/ml | RB Pharmaceuticals LDT | N/A | |
| Ceftiofur 3 mg/ml | Pfizer Canada Inc. | 11103 | |
| Cefazolin 1 g | Pharmaceutical Partners of Canada Inc. | 2237138 | |
| Fentanyl Citrate 0.25 mg/5 ml | Sandoz Canada Inc. | 2240434 | |
| Heparin 10,000 iU/10 ml | Sandoz Canada Inc. | 10750 | |
| Histidine-tryptophan-ketoglutarate (HTK) solution | Methapharm | CU001LBG | |
| Isoflurane 99.9%, 250 ml | Pharmaceutical Partners of Canada Inc. | 2231929 | |
| Ketamine Hydrochloride 5,000 mg/50 ml | Bimeda-MTC Animal Health Inc. | 612316 | |
| Lactated Ringer’s + 5% Dextrose 1 L | Baxter Corporation | JB1064 | |
| Lactated Ringer’s 1 L | Baxter Corporation | JB2324 | |
| Metronidazole 500 mg/100 ml | Baxter Corporation | 870420 | |
| Midazolam 50 mg/10 ml | Pharmaceutical Partners of Canada Inc. | 2242905 | |
| Norepinephrine 16 mg/250 ml Dextrose 5% | Baxter Corporation | N/A | |
| Pantoprazole 40 mg | Sandoz Canada Inc. | 2306727 | |
| Papaverine 65 mg/2 ml | Sandoz Canada Inc. | 9881 | |
| Propofol 1,000 mg/100 ml | Pharmascience Inc. | 2244379 | |
| Saline 0.9%, 1 L | Baxter Corporation | 60208 | |
| Solu-Medrol 500 mg | Pfizer Canada Inc. | 2367963 | |
| Verapamil | Sandoz Canada Inc. | 2166739 | |
| Xylocaine Endotracheal 10 mg/50 ml | AstraZeneca | 2003767 |
参考文献
- Wolfe, R. A., Ashby, V. B., et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 341 (23), 1725-1730 (1999).
- Ingsathit, A., Kamanamool, N., Thakkinstian, A., Sumethkul, V. Survival advantage of kidney transplantation over dialysis in patients with hepatitis C: a systematic review and meta-analysis. Transplantation. 95 (7), 943-948 (2013).
- Tonelli, M., Wiebe, N., et al. Systematic review: kidney transplantation compared with dialysis in clinically relevant outcomes. Am J Transplant. 11 (10), 2093-2109 (2011).
- Matas, A. J., et al. OPTN/SRTR Annual Data Report 2012: Kidney. Am J Transplant. 14, (2014).
- . Annual Report 2013 - Eurotransplant International Foundation. Available from: https://www.eurotransplant.org/cms/mediaobject.php?file=AR20135.pdf (2013)
- Morrissey, P. E., Monaco, A. P. Donation after circulatory death: current practices, ongoing challenges, and potential improvements. Transplantation. 97 (3), 258-264 (2014).
- Maggiore, U., Oberbauer, R., et al. Strategies to increase the donor pool and access to kidney transplantation: an international perspective. Nephrol Dial Transplant. 30 (2), 217-222 (2014).
- Summers, D. M., Johnson, R. J., Hudson, A., Collett, D., Watson, C. J., Bradley, J. A. Effect of donor age and cold storage time on outcome in recipients of kidneys donated after circulatory death in the UK: a cohort study. Lancet. 381 (9868), 727-734 (2013).
- Wadei, H. M., Heckman, M. G., et al. Comparison of kidney function between donation after cardiac death and donation after brain death kidney transplantation. Transplantation. 96 (3), 274-281 (2013).
- Moers, C., Smits, J. M., et al. Machine perfusion or cold storage in deceased-donor kidney transplantation. N Engl J Med. 360 (1), 7-19 (2009).
- Pereira-Sampaio, M. A., Favorito, L. A., Sampaio, F. J. B. Pig kidney: anatomical relationships between the intrarenal arteries and the kidney collecting system. Applied study for urological research and surgical training. J Urol. 172 (5 Pt 1), 2077-2081 (2004).
- Bagetti Filho, H. J. S., Pereira-Sampaio, M. A., Favorito, L. A., Sampaio, F. J. B. Pig kidney: anatomical relationships between the renal venous arrangement and the kidney collecting system. J Urol. 179 (4), 1627-1630 (2008).
- Giraud, S., Favreau, F., Chatauret, N., Thuillier, R., Maiga, S., Hauet, T. Contribution of large pig for renal ischemia-reperfusion and transplantation studies: the preclinical model. J Biomed Biotechnol. 2011 (21), 532127 (2011).
- Gallinat, A., Paul, A., et al. Role of oxygenation in hypothermic machine perfusion of kidneys from heart beating donors. Transplantation. 94 (8), 809-813 (2012).
- Thuillier, R., Allain, G., et al. Benefits of active oxygenation during hypothermic machine perfusion of kidneys in a preclinical model of deceased after cardiac death donors. J Surg Res. 184 (2), 1174-1181 (2013).
- Hosgood, S. A., Barlow, A. D., Yates, P. J., Snoeijs, M. G. J., van Heurn, E. L. W., Nicholson, M. L. A pilot study assessing the feasibility of a short period of normothermic preservation in an experimental model of non heart beating donor kidneys. J Surg Res. 171 (1), 283-290 (2011).
- Delpech, P. O., Thuillier, R., et al. Effects of warm ischaemia combined with cold preservation on the hypoxia-inducible factor 1α pathway in an experimental renal autotransplantation model. Br J Surg. 101 (13), 1739-1750 (2014).
- Kirk, A. D. Crossing the bridge: large animal models in translational transplantation research. Immunol Rev. 196, 176-196 (2003).
- Golriz, M., Hafezi, M., et al. Do we need animal hands-on courses for transplantation surgery. Clin Transplant. 27, 6-15 (2013).
- He, B., Musk, G. C., Mou, L., Waneck, G. L., Delriviere, L. Laparoscopic surgery for kidney orthotopic transplant in the pig model. JSLS. 17 (1), 126-131 (2013).
- Faure, A., Maurin, C., et al. An experimental porcine model of heterotopic renal autotransplantation. Transplant Proc. 45 (2), 672-676 (2013).
- Hosgood, S. A., Yates, P. J., Nicholson, M. L. 1400W reduces ischemia reperfusion injury in an ex-vivo porcine model of the donation after circulatory death kidney donor. World J Transplant. 4 (4), 299-305 (2014).
- Ghanekar, A., Mendicino, M., et al. Endothelial induction of fgl2 contributes to thrombosis during acute vascular xenograft rejection. J Immunol. 172 (9), 5693-5701 (2004).
- Ghanekar, A., Lajoie, G., et al. Improvement in rejection of human decay accelerating factor transgenic pig-to-primate renal xenografts with administration of rabbit antithymocyte serum. Transplantation. 74 (1), 28-35 (2002).
- Cowan, P. J., Cooper, D. K. C., d'Apice, A. J. F. Kidney xenotransplantation. Kidney Int. 85 (2), 265-275 (2014).
- Seldinger, S. I. Catheter replacement of the needle in percutaneous arteriography; a new technique. Acta radiol. 39 (5), 368-376 (1953).
- Hanto, D. W., Maki, T., et al. Intraoperative administration of inhaled carbon monoxide reduces delayed graft function in kidney allografts in Swine. Am J Transplant. 10 (11), 2421-2430 (2010).
- Maathuis, M. -. H. J., Manekeller, S., et al. Improved kidney graft function after preservation using a novel hypothermic machine perfusion device. Ann Surg. 246 (6), 982-991 (2007).
- Gallinat, A., Paul, A., et al. Hypothermic reconditioning of porcine kidney grafts by short-term preimplantation machine perfusion. Transplantation. 93 (8), 787-793 (2012).
- Snoeijs, M. G., Matthijsen, R. A., et al. Autologous transplantation of ischemically injured kidneys in pigs. J Surg Res. 171 (2), 844-850 (2011).
- Golriz, M., Fonouni, H., Nickkholgh, A., Hafezi, M., Garoussi, C., Mehrabi, A. Pig kidney transplantation: an up-to-date guideline. Eur Surg Res. 49 (3-4), 121-129 (2012).
- Hosgood, S. A., Bagul, A., Yang, B., Nicholson, M. L. The relative effects of warm and cold ischemic injury in an experimental model of nonheartbeating donor kidneys. Transplantation. 85 (1), 88-92 (2008).
- Hoyer, D. P., Gallinat, A., et al. Influence of oxygen concentration during hypothermic machine perfusion on porcine kidneys from donation after circulatory death. Transplantation. 98 (9), 944-950 (2014).
転載および許可
このJoVE論文のテキスト又は図を再利用するための許可を申請します
許可を申請さらに記事を探す
This article has been published
Video Coming Soon
Copyright © 2023 MyJoVE Corporation. All rights reserved