로그인
JoVE Science Education
Neuropsychology
JoVE 비디오를 활용하시려면 도서관을 통한 기관 구독이 필요합니다.
의사 결정 및 아이오와 도박 과제
Overview
출처: 조나스 T. 카플란과 사라 I. 짐벨의 연구소 - 서던 캘리포니아 대학
의사 결정은 행동이나 인식의 과정에 대한 선택이 많은 가능성에서 이루어지는 인간의 집행 기능의 중요한 구성 요소입니다. 전두엽의 열등한 부분에 손상은 좋은 결정을 내리는 사람의 능력에 영향을 미칠 수 있습니다. 그러나 의사 결정 적자는 자신의 삶에 큰 영향을 미칠 수 있지만, 이러한 적자는 실험실에서 정량화하기 어려울 수 있습니다. 1990년대 중반, 실험실에서 실제 의사 결정을 모방하기 위한 작업이 수행되었습니다. 아이오와 도박 작업 (IGT)로 알려진이 작업은 의사 결정 능력의 매우 민감한 척도로 연구 및 임상 연구에서 널리 사용되는 인지적으로 복잡한 작업입니다. 1-3
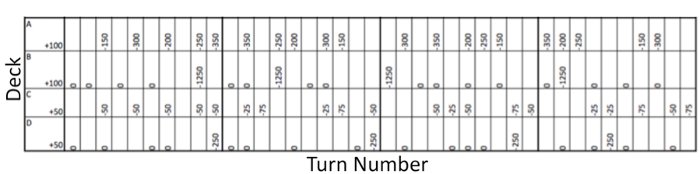
IGT에서 참가자는 4개의 카드 덱을 표시하고 각 턴마다 한 덱에서 카드를 공개하기로 결정합니다. 카드를 뒤집으면 참가자는 돈을 받을 수 있지만 때로는 벌금을 지불해야합니다. 두 덱은 더 높은 보수를 가지고 있지만, 또한 이러한 덱에서 선택하는 것은 장기적으로 순 손실로 이어질 수 있도록 높은 페널티가 있습니다. 다른 두 덱은 낮은 보수를 가지고 있지만, 또한 작은 처벌을 제시, 그래서 이러한 갑판에서 선택하는 것은 순이익으로 이어질. 따라서, 유리한 선택을하기 위해, 참가자는 시간이 지남에 따라 손실과 이익에 대한 정보를 통합해야합니다.
이 비디오는 IGT를 투여하여 심엽기 전두엽 피질에 손상을 입은 환자의 성능을 일치하는 대조군 과목 그룹에 비교하여 이 뇌 영역의 고유한 의사 결정에 기여하는 방법을 보여줍니다.
Procedure
1. 참가자 모집
- 환자 모집
- 전두엽 코르티제의 심혈관 구역에 손상을 입은 10명의 환자를 모집합니다.
- 이 지역에 손상은 MRI를 가진 신경 화상 진찰에 의해 확인됩니다. 벤트롬방 전두엽 피질은 복부 표면에 대뇌 피질의 가장 전방 내측 벽에 위치하고 있습니다. 손상은 일방적이거나 양자일 수 있지만, 환기 전두엽 피질을 넘어서서는 안 됩니다. 이러한 환자의 뇌의 예는 도 1에도시된다.
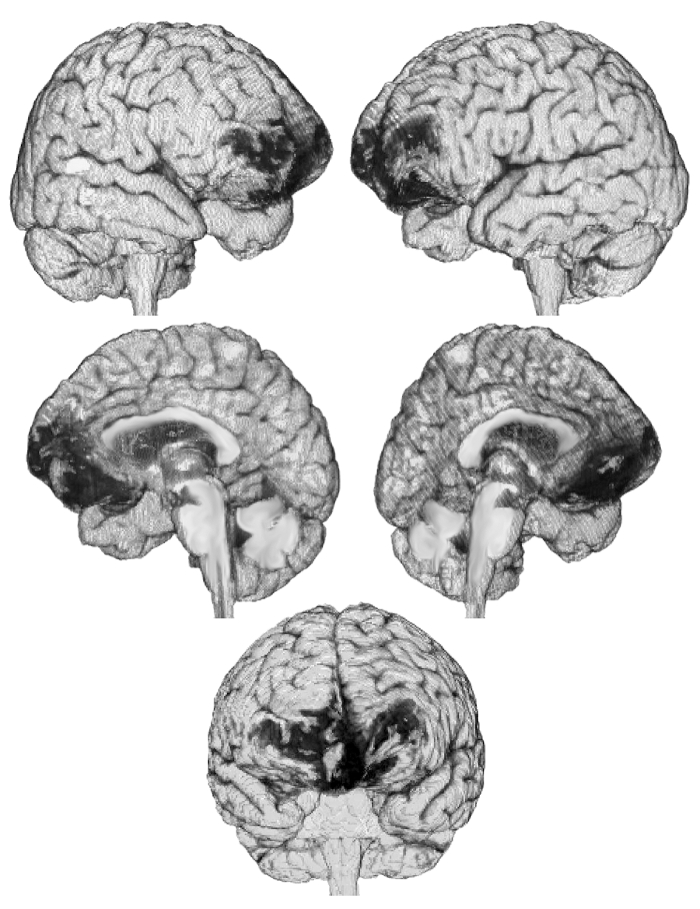
그림 1: VMPFC 손상을 입은 환자의 뇌의 컴퓨터 재구성. 이 환자는 MRI 이미지로 만든이 3D 재건에서 와 같이 내측 전두엽 피질에 양측 손상을 입힙니다. 이미지 제공: 한나 다마시오.
- 제어
Results
4개의 덱에서 100장의 카드를 뽑은 일반 컨트롤은 좋은 덱(C와 D)에서 더 많은 선택을 했고, 나쁜 덱(A와 B)을 피했습니다. 대조적으로, 심실 전두엽 피질 (VMPFC) 손상을 가진 환자는 나쁜 갑판 (A 및 B)에서 더 많은 선택을 하고, 좋은 갑판 (C와 D)를 피했습니다; 그림 3). 데크 A와 B의 컨트롤에 의해 선택된 카드의 수는 환자가 해당 덱에서 선택한 카드 수보다 훨씬 적?...
Application and Summary
이 작업은 다양한 인구의 의사 결정 적자를 평가하는 역할을 할 수 있습니다. 예를 들면, VMPFC에 손상을 가진 환자 이외에, 양측 편도체 손상을 가진 환자는 또한 IGT에 의해 측정될 수 있는 가혹한 의사 결정 손상을 보여줍니다. 또한, 불리한 의사 결정은 물질 중독, 병리학 적 도박, 정신 분열증, 강박 장애, 식욕 부진 nervosa, 주의력 결핍 /과잉 행동 장애, 정신 병증, 비만 및 많은 다른 사람을 포함하...
References
- Bechara, A., Damasio, A.R., Damasio, H. & Anderson, S.W. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 50, 7-15 (1994).
- Bechara, A., Damasio, H., Tranel, D. & Damasio, A.R. Deciding advantageously before knowing the advantageous strategy. Science 275, 1293-1295 (1997).
- Li, X., Lu, Z.L., D'Argembeau, A., Ng, M. & Bechara, A. The Iowa Gambling Task in fMRI images. Hum Brain Mapp 31, 410-423 (2010).
- Shurman, B., Horan, W.P. & Nuechterlein, K.H. Schizophrenia patients demonstrate a distinctive pattern of decision-making impairment on the Iowa Gambling Task. Schizophr Res 72, 215-224 (2005).
건너뛰기...
이 컬렉션의 비디오:

Now Playing
의사 결정 및 아이오와 도박 과제
Neuropsychology
32.4K Views

분할 뇌
Neuropsychology
68.2K Views

운동 지도
Neuropsychology
27.5K Views

신경 심리학에 대한 관점
Neuropsychology
12.0K Views

자폐 스펙트럼 장애의 실행 기능
Neuropsychology
17.7K Views

사건후기억상실
Neuropsychology
30.3K Views

감정 인식의 생리학적 상관 관계
Neuropsychology
16.2K Views

사건 관련 잠재력과 오드볼 과제
Neuropsychology
27.4K Views

언어: 의미 부조화의 N400
Neuropsychology
19.6K Views

학습과 기억: 기억-알기 과제
Neuropsychology
17.1K Views

화소 기반 형태법으로 회백질 차이 측정: 음악 두뇌
Neuropsychology
17.3K Views

다용적 패턴 분석으로 청각 이미지 디코딩
Neuropsychology
6.4K Views

시각 주의: 사물을 활용한 집중력 제어의 fMRI 조사
Neuropsychology
41.6K Views

외상성 뇌 손상에서의 확산 텐서 이미징 사용
Neuropsychology
16.7K Views

TMS를 사용한 동작 관찰 중 운동 흥분성 측정
Neuropsychology
10.1K Views
Copyright © 2025 MyJoVE Corporation. 판권 소유
당사 웹 사이트에서는 사용자의 경험을 향상시키기 위해 쿠키를 사용합니다.
당사 웹 사이트를 계속 사용하거나 '계속'을 클릭하는 것은 당사 쿠키 수락에 동의하는 것을 의미합니다.