
Method Article
A Controlled Mouse Model for Neonatal Polymicrobial Sepsis
* These authors contributed equally
In This Article
Summary
This protocol provides the necessary steps to establish and evaluate neonatal sepsis in 7-day-old mice.
Abstract
Neonatal sepsis remains a global burden. A preclinical model to screen effective prophylactic or therapeutic interventions is needed. Neonatal mouse polymicrobial sepsis can be induced by injecting cecal slurry intraperitoneally into day of life 7 mice and monitoring them for the following week. Presented here are the detailed steps necessary for the implementation of this neonatal sepsis model. This includes making a homogeneous cecal slurry stock, diluting it to a weight- and litter-adjusted dose, an outline of the monitoring schedule, and a definition of observed health categories used to define humane endpoints. The generation of a homogeneous cecal slurry stock from pooled donors allows for the administration into many litters over time, reducing the variation between donors, and preventing the use of potentially toxic glycerol. The monitoring strategy used allows for the anticipation of survival outcome and the identification of mice that would later progress to death, allowing for an earlier identification of the humane endpoint. Two main behavioral features are used to define the health scores, namely, the ability of the neonatal mice to right themselves when placed on their back and their level of mobility. These criteria could potentially be applied to address humane endpoints in other studies of neonatal disease in mice, as long as a pilot study is performed to confirm accuracy. In conclusion, this approach provides a standardized method to model newborn sepsis in mice, while providing resources to assess animal welfare used to define early humane endpoints for challenged animals.
Introduction
Sepsis is a leading cause of human newborn infectious deaths1. Because newborn sepsis is poorly understood, little progress has been made in both the identification of at-risk newborns early during the disease and the development of efficacious treatments or prophylaxes. This necessitates the use of animal models of sepsis to better understand the process and test possible interventions. Furthermore, adult rodents respond differently to sepsis, with statistically significant differences in the number of bacteria to administer to obtain the same lethal dose (LD) and differences in the resulting host response as compared to newborns2. Thus, neonatal sepsis has to be studied in neonates. Several adult sepsis models have been used in sepsis research. These include an intravenous challenge with specific organisms implicated in adult human sepsis or cecal ligation and puncture (CLP). CLP is an endogenous challenge model where the cecum is surgically isolated, ligated, and punctured to allow leakage of intestinal contents into the peritoneum, eventually leading to the systemic dissemination of microbes and their products3. However, the surgical procedure required to establish CLP is lethal to newborn animals; therefore, an alternate method is necessary to mimic the polymicrobial challenge of CLP to induce neonatal sepsis. The cecal slurry model for neonatal polymicrobial sepsis was developed to address this need, whereby the cecal contents of animals are harvested, suspended in sterile dextrose 5% in water (D5W), and intraperitoneally injected into newborn mice2. This has, since, become an increasingly popular model to study sepsis in both newborn and adult animals and has substantially advanced mechanistic insights in the disease's process4,5,6,7,8,9,10,11,12,13,14,15.
Given the increasing use of this model and desire of researchers to directly compare results across publications, there is a need for the technical aspects to be well described and standardized across studies. Standardization applies to three aspects of the model, namely, i) the preparation of the cecal slurry stock, ii) the preparation of the challenge aliquots for injection into the experimental animals, and iii) the definition of the humane endpoint whereby animals are deemed nonsurvivors in challenge experiments. Specifically, methods to prepare the cecal slurry stock are often referenced to the original article introducing the model2. A brief summary of that model is that cecal contents from adult mice were harvested, suspended in sterile D5W to a concentration of 80 mg/mL, and used within 2 h to inject the experimental animals. This original model used mice of the same age, from the same vendor location, which were housed in their respective research facilities for less than 2 weeks prior to harvesting cecal contents. The use of in-house bred mice, although reducing the cost from regular vendor delivery and allowing for the use of excess mice of a broader range of sex and age, also substantially increased donor-to-donor variability. This motivated the development of an alternative technique, whereby cecal contents from multiple mice were pooled together to prepare a large stock, which was then aliquoted and stored at -80 °C13. This alternate method was adapted by multiple groups14,15. However, that adaptation resulted in some technical variations, both in the storage media used (10% or 15% glycerol, or D5W alone) and in the strategy of filtration to remove particulate (multistage filtration through a 860 µm and, then, a 190 µm filter, or individual filtrations through 100 µm or 70 µm filters)13,14,15. The injection of glycerol alone could potentially cause harm, given that 25%-50% glycerol injections have been used as a rodent model of renal injury16,17,18,19,20. To avoid unintended side effects of glycerol, the cecal slurry stock preparation for mice in this study is frozen in D5W without glycerol, and tests of bacterial viability from storage at -80 °C are performed. The filtration strategy used in this study is one pass through a 70 µm filter, which has not been directly compared to the other filtration strategies listed.
Lethal weight-adjusted doses of injected cecal slurry may vary from facility to facility and should be titered out to the desired lethality for individual groups. With different challenge doses, the accompanying challenge volumes change by necessity. However, this methodological detail has not been reported before. Furthermore, strategies for standard procedures, such as intraperitoneal injection, are rarely elaborated on within the literature, but individual techniques may affect whether newborn mice leak when injected and impact their final outcomes.
Animal welfare, including a definition of humane endpoint, is a central aspect of this model and in any model of infection and inflammation in rodents21. In 1998, the Canadian Council on Animal Care (CCAC) published extensive guidelines for humane endpoint selection, defining the humane endpoint as "any actual or potential pain, distress, or discomfort should be minimized or alleviated by choosing the earliest endpoint that is compatible with the scientific objectives of the research"22. Others also caution that humane endpoints must be established based on scientific justification rather than on a subjective interpretation of the animal's state alone21. While there is a wealth of resources for clinical, behavioral, and body-condition sign-based criteria for humane endpoint, even in the context of infection and inflammation specifically21,23,24, none of these, including the CCAC guidelines for humane endpoint22, mention newborn mice. Thus, objectively and scientifically justified humane endpoints are much more difficult to establish for newborn animals, given both their limited behavioral capabilities and the lack of evidence from criteria like weight loss, which is commonly used for adult mice. Currently, the criteria for the humane endpoint used for 5- to 12-day-old neonatal mice in the cecal slurry literature all reference back to the original manuscript that introduced the model2. In this original paper, the definition of humane endpoint for newborn animals was based on two criteria; namely, the location of a mouse outside of the nest (scattering) and the lack of milk spots had been seen to result in death within hours. A complicating matter in assigning a humane endpoint is that milk spots become difficult to see in mouse strains with dark fur, such as the commonly employed C57BL/6J strain, after the first week of life, while sick animals are monitored until the 14th day of life (DOL). Further, dead animals can be found postchallenge when applying these criteria (own observation; unpublished); thus, a more rigorous definition of humane endpoint is necessary to alleviate suffering to experimental animals and avoid mortality in situations where the outcome could be accurately discerned earlier.
All three methodological aspects of the cecal slurry model are presented in a standard operating procedure detailing the preparation of cecal slurry stock, a method for injecting experimental animals that keeps the injection volume constant between doses and reduces the risk of leaks, and a definition of humane endpoint for 7- to 12-day-old mice based on a system of behavioral modeling. Behavioral information of mouse health scores from over 240 experimental animals was collected and grouped by final survival outcome, demonstrating an evidence-driven definition of humane endpoint. The suffering of experimental animals is reduced by identifying moribund neonatal mice at the earliest possible time point, while biologically significant survival outcomes can be inferred by observing key variables. The visual representation of both cecal slurry preparation and neonatal mouse behaviors will serve as an excellent resource to any group studying sepsis or newborn challenge model animals.
Protocol
All experiments in this protocol have been approved by the University of British Columbia Animal Care Committee under protocol number A17-0110.
1. Tool sterilization
- In a biological safety cabinet (BSC), turn on and preheat the hot bead sterilizer to 250 °C, at least 30 min before use.
- Dip the tools in 70% ethanol.
- Submerge the tools into the preheated hot bead sterilizer for a minimum of 1 min.
NOTE: The handles of the tools will get hot and may burn if left in the hot bead sterilizer for over 1.5 min. - Spray a mat of paper towels with 70% ethanol to sterilize it.
- Remove the tools from the hot bead sterilizer without touching the sterilized part of the tool to the nonsterile handles of other submerged tools and place them on the ethanol-sprayed paper towels.
- Wait for 30 s to 2 min for the tools to cool down before using them for dissection.
2. Cecal slurry preparation
- Preweigh 15 mL centrifuge tubes (one tube for every five mice being euthanized).
- Euthanize cecal slurry donors according to local animal care guidelines or use the protocol below.
NOTE: Up to 40 C57BL/6J mice between 6 and 12 weeks old were used for cecal slurry preparation, with up to five mice being euthanized at a time.- Transfer the mice to the euthanasia chamber and set the isoflurane anesthesia machine to 5% with oxygen perfusion.
- Monitor the mice to observe the loss of the ability to move and to see them entering the surgical plane of anesthesia and finally, stop breathing.
- Remove a mouse from the euthanasia chamber, pinch its paw and observe any leg retraction or inhalation. If either is present, return the mouse to the euthanasia chamber; otherwise, continue.
- Terminally euthanize the mice by sharp cervical dislocation.
- Perform cecum dissection, using presterilized and cooled tools (see section 1) in a BSC.
- Pin the legs of the mouse to an extruded polystyrene foam board using 23 G needles so that the mouse has its abdomen up. Secure and then spray the abdomen with 70% ethanol.
- Using sterile forceps and scissors, cut through the skin, loosen the skin from the peritoneal lining with the scissors, and cut open a rectangular region from groin to sternum, and left side to right side. Remove any fur from the peritoneum.
- Switch to a new pair of sterile tools to cut through the peritoneum, making a rectangular opening as was done for the skin, switching tools if the ones used contact the skin.
- Identify the cecum, which should be running left to right across the body. Disrupt connective tissue to identify the cecum branches from the intestines and cut the cecum away from the intestines. Place the cecum on a sterilized sheet of weighing paper.
NOTE: Weighing paper can be sterilized either by spraying it with 70% ethanol on both sides and leaving it to dry, or by UV irradiation. Alternatively, the cecum can be dissected on a sterile Petri plate.
- Cecal content extrusion
- In a BSC, use sterile tools to cut through both ends of the cecum.
- Hold the middle of the cecum with sterile forceps and use a flat sterile metal spatula to gently push the cecal contents out of the cut ends, using a rolling motion and avoiding a scraping motion that could tear the epithelium. Collect the contents and place them into a preweighed 15 mL centrifuge tube.
- Pool the cecal contents from a maximum of five mice into the same tube. Weigh the tube again once all the contents have been added.
NOTE: Expect an average of 300 mg, and up to 390 mg of cecal slurry per mouse, requiring 1.8 to 2.4 mL of D5W for resuspension per mouse; therefore, using more than five mice during this step can result in overfilling the 15 mL centrifuge tube. - Wipe the tools clean with an ethanol-sprayed paper towel and resterilize them by repeating steps 1.2-1.6.
- Cecal slurry filtration
- Weigh the centrifuge tube filled with cecal contents and calculate the amount of D5W to add to the cecal contents by dividing the weight of the cecal contents by the desired stock concentration in milligrams per milliliter, as in the equation below.

- In a BSC, add the required amount of ice-cold D5W to the 15 mL centrifuge tube containing the cecal contents.
- Vortex the 15 mL centrifuge tube vertically and horizontally for 30 s. Check for particulate of more than 1-3 mm in diameter, and if present, continue vortexing until all large particulate has visibly disappeared.
- Place a sterile 70 µm cell strainer into a 50 mL centrifuge tube that is placed on ice. Pipette 4 mL of resuspended cecal slurry into the cell strainer and, then to the collection tube. Resuspend the particulate by pipetting up and down 2x-3x. Gently extrude bubbles to increase the filtering speed while stirring the contents with the pipette tip until there are no more droplets being filtered.
NOTE: When mixing, there may be particulate large enough to plug the 5 mL pipette. In this case, repeat the vortexing from step 2.5.3, and if the solution still does not break apart, use the pipette to press the particulate against the wall of the centrifuge tube. - Repeat step 2.5.4, changing cell strainers between each tube of cecal slurry, and pool all contents into the same 50 mL centrifuge collection tube kept on ice, or into a second 50 mL centrifuge tube if the volume of the filtrate exceeds the ice level in the ice box.
- Weigh the centrifuge tube filled with cecal contents and calculate the amount of D5W to add to the cecal contents by dividing the weight of the cecal contents by the desired stock concentration in milligrams per milliliter, as in the equation below.
- Aliquot the cecal slurry.
- If applicable, combine multiple 50 mL cecal slurry filtrate tubes from step 2.5.5 into a larger sterile container (e.g., a 1,000 mL storage bottle). Then, vortex for 15 s and place 20 mL into a new 50 mL centrifuge tube.
- Vortex the cecal slurry stock that is in the 50 mL centrifuge tube for 5-10 s, and aliquot 500 µL into three 2 mL cryogenic vials that have a rubber seal, to prevent evaporation over time. Immediately place the master stock and aliquoted cryogenic vial on ice.
- Repeat steps 2.6.1 and 2.6.2 until all of the cecal slurry has been aliquoted, vortexing the master stock after every three cryogenic vials to prevent the settling of any particulate and to maintain a homogeneous mixture.
- Freeze the cecal slurry aliquots at -80 °C.
NOTE: Expect between three to four stock vials at 500 µL from each adult mouse. Each stock vial should be roughly enough to challenge one litter of eight mice at DOL 7.
3. Sepsis challenge of 7-day-old neonatal mice
- Separate, identify, and weigh neonatal mice.
- In a BSC, transfer the neonatal mice to a new cage to keep the mice away from the dam and to reduce stress to the dam.
- Remove and rub part of the nesting material with gloves to transfer the cage's smell to the gloves. Then, mold the nesting material into a smaller nest and place it into a new cage without the dam.
- Transfer the neonatal mice to the nesting material in the new cage.
- Transfer more nesting material to make a second, empty nest in the new cage.
- Close and remove the dam's cage from the hood so that the dam is not stressed from hearing any of the neonatal mice's distress.
- To track individual neonatal mice within the litter over time, use an ethanol-proof marker to mark one to five dots on the front or reverse of the tail, reapplying every 12-24 h as needed.
- Weigh each mouse that will be challenged, placing each into the secondary nest after weighing, and repeat this for all the mice.
- Return the entire litter to the dam before preparing the cecal slurry challenge aliquot.
- Calculate the individual weight-adjusted doses of cecal slurry and required dilution with D5W by completing this step for each litter separately, using the calculations below or using the provided worksheet (see Supplemental File).
- Calculate the milligrams of cecal slurry (a) to be administered to each mouse by multiplying the weight of the mouse in grams (b) by the desired challenge dose in milligrams of cecal slurry per gram of mouse (c).

- Calculate the individual volume of undiluted cecal slurry stock required per mouse in microliters (d) by dividing the milligrams of cecal slurry needed per mouse from step 3.2.1 (a) by the stock cecal slurry concentration, 160 mg of cecal slurry per milliliter of D5W (e), and multiplying by 1,000 µL per milliliter to convert from milliliters to microliters.

- Average the stock volume of cecal slurry required per mouse (g) by summing the volume of cecal slurry stock (d) per mouse in a litter of n mice, divided by the number of mice (n).

- Calculate the average dilution factor for the cecal slurry stock (h) by dividing the average injection volume (100 µL) by the average stock volume of cecal slurry required per mouse (g).

- Calculate each mouse's specific injection volume in microliters (j) by multiplying each mouse's volume of stock cecal slurry required (d) by the average dilution factor (h), and then round it off to the nearest ten (to match the 10 µL increments of the injection syringe).

- Calculate the average required volume of D5W to dilute the cecal slurry stock (k) by subtracting the average cecal slurry stock (g) from the average injection volume (100 µL).

- Calculate the total amount of cecal slurry stock in microliters (l) by multiplying the average stock cecal slurry per mouse in microliters (g) by the number of mice in this litter (n) and multiplying by 1.4 to create extra.

- Calculate the total amount of D5W in microliters (m) required to dilute the cecal slurry stock by multiplying the average required volume of D5W (k) by the number of mice (n) and multiplying by 1.4 to create extra.

- Calculate the milligrams of cecal slurry (a) to be administered to each mouse by multiplying the weight of the mouse in grams (b) by the desired challenge dose in milligrams of cecal slurry per gram of mouse (c).
- Prepare the challenge aliquot after calculating the amount of stock cecal slurry required (l from step 3.2.7). In a BSC, thaw the required number of cecal slurry stock vials at room temperature, pipetting its contents to mix.
- When there are no more visible ice crystals present in the thawed cecal slurry, transfer the calculated amount of cecal slurry stock (l from step 3.2.7) to a sterile 1.8 mL microcentrifuge tube.
- Dilute to the required concentration by adding ice-cold D5W as calculated in step 3.2.8 (m). Store the challenge aliquot on ice.
- Before loading the syringe, mix the microcentrifuge tube by flicking it 20x, followed by 3x of drawing up and expelling 300-500 µL of cecal slurry with a 500 cc 28 G ½ inch insulin syringe.
- Draw up roughly 150 µL of diluted cecal slurry into the same syringe.
- Flick the syringe to dislodge bubbles from the plunger, draw back slightly on the syringe, and then expel the bubbles.
- Dispense the excess cecal slurry back into the microcentrifuge tube until the correct amount of cecal slurry for one mouse, as was calculated for individual mice in step 3.2.5 (j), is loaded in the syringe.
- Intraperitoneally inject cecal slurry, according to relevant local animal care institution guidelines, or use the steps outlined below.
- In a BSC, separate the neonatal mice from the dam as described in step 3.1.
- Scruff the mouse by the back of the neck, using the thumb and index finger.
- Secure the mouse's tail across the back of the middle and ring fingers, or on the front of the ring and pinky fingers.
- To minimize leaks, tilt the neonatal mouse so that it faces downward and insert the needle bevel of the needle facing up, between the leg and the genitalia, keeping the needle shallow and subcutaneous.
- When the needle is inserted for 1 cm, press downward and forward to feel the needle puncture the peritoneum. Slowly depress the plunger, keeping the tip of the needle as steady as possible, as lateral movements could damage the mouse's organs.
- Carefully withdraw the needle over 5-10 s, following the same route out as in, relaxing the middle finger during the removal to reduce tension in the mouse's body.
- To check for leaks, hold the mouse for a few seconds after the removal of the needle, to allow time for the injection site to close, and observe any leakage or bulging at the injection site, at which point the mouse should not be used in the analysis.
NOTE: Bulging of the skin at the injection site indicates a failed intraperitoneal injection, with the injectant being subcutaneous. - Place the mouse on a paper towel and allow the mouse to take a step. If the mouse is immobile for 5 s, then lightly press the tail.
- Pick up the mouse and check for any leakage of cecal slurry at the injection site. If there is a leak, exclude the mouse from the analysis and euthanize the mouse.
4. Mouse monitoring
- Monitor the mice regularly to check them for arriving at a humane endpoint.
- Observe the mice 2 h postchallenge for any injection-related complications.
- Monitor the mice 12 h postchallenge for sepsis-related morbidity and the identification of mice at a humane endpoint (see steps 4.2-4.3 for criteria).
- Subsequently monitor every 4-6 h for the first 2 days, except for 8 h overnight, when the neonatal mice are unattended.
- Beyond 2 days postchallenge, monitor 1x-2x per day. If sick mice or mice whose health score decreases are observed, then increase the monitoring frequency to every 4-6 h.
- Monitoring neonatal mice
- For any procedure involving neonatal mice, transfer the bedding material to a new cage as described in step 3.1 (for the same reasons as mentioned there). Carefully check for any neonates that are dragged from the nest while nursing. Any mice that are dragged out of the litter while nursing should not be considered to be scattered mice.
- When removing the top of the nest, identify any scattering of neonatal mice either away from the nest or stuck in the nesting material but away from their littermates, with the exception of mice dragged away from the litter while nursing. Refer to the humane endpoint criteria in step 4.5 if a mouse is found scattered.
- Measure the mice's righting reflexes and mobility.
- On a paper towel, place a mouse on its back and monitor for its ability to right itself within a maximum of 4 s. When placed on its back, the mouse will fall to either the left or right side, which is when the 4 s count begins.
NOTE: To be classified into the "Rights" group, the mouse must be able to get at least three of four paw pads on the paper towel for 1 s. It is still grouped as being able to right itself if it falls over.- If the mouse can right itself, then wait for 8 s to determine its level of mobility.
- Categorize the mouse as "Rights-Mobile" if it can right itself and explore its environment by taking multiple steps in a row.
- Categorize the mouse as "Rights-Lethargic" if it can right itself and take a few steps to explore its environment. The mice in this group may fall over while taking a step, look shaky on their feet, and pause between steps.
- Categorize the mouse as "Rights-Nonmobile" if it can right itself but does not move around a lot. It may still fall over, and if it does not take any steps within 8 s, it is grouped as Rights-Nonmobile.
- If the mouse could not right itself, then categorize its mobility based on the observed hip movement.
NOTE: Avoid repeating the monitoring or increasing the length of time the mouse spends on their back because this could affect the scoring system and humane endpoint, as a mouse that fails to right itself within 4 s can sometimes do so if given more time.- Categorize the mouse as "Fail to right (FTR)-Mobile" if it is unable to right itself and displays hip movement that exceeds 90° angle from horizontal. Some mice can right themselves if given more than 4 s but should still be categorized as FTR, with mobility scores based on hip movement.
- Categorize the mouse as "FTR-Lethargic" if it is unable to right itself and displays hip movement below 90° angle from horizontal.
- Categorize the mouse as "FTR-Nonmobile" if it is unable to right itself and has legs that shake or vibrate but no hip movement. Limbs may extend or retract but do not have lateral movement. The mouse is visibly ill and has reached the humane endpoint.
- On a paper towel, place a mouse on its back and monitor for its ability to right itself within a maximum of 4 s. When placed on its back, the mouse will fall to either the left or right side, which is when the 4 s count begins.
- Repeat step 4.3 on the other side of the mouse, recording both sides.
NOTE: See the Supplementary File for recording observations. - Determine whether the mouse is at a humane endpoint and requires euthanasia as outlined in Table 1, and below.
- Categorize mice into different righting and mobility levels based on the monitoring observations noted in steps 4.3 and 4.4. The mouse's mobility is measured for each side, and the mobile behavior is used to determine whether the mouse requires euthanasia.
- Assign any mice with a righting reflex of either (a) FTR-Nonmobile or (b) FTR-Lethargic and found separated from the nest to be at a humane endpoint.
- In monitoring time points beyond 20 h postchallenge, classify any mouse with a righting reflex of "fail to right" on both sides as being at a humane endpoint, because the presented data predict with high accuracy that these mice eventually succumb to disease, and do not recover.
- Separate mice that are to be euthanized, as determined in step 4.5. If the monitored mouse is not seen as at a humane endpoint, place it into the second empty nest in the new cage without the dam, and continue with the other neonatal mice.
- Once the entire litter has been monitored, move half of the nesting material into the cage with the dam, reforming a nest with room in the middle for the neonatal mice.
NOTE: An improperly formed nest could cause the mice to scatter and reduce the amount of available care that the dam can offer. - Transfer the neonatal mice back into the cage with the dam.
- Enclose the litter in the nest by putting the leftover nesting material over the litter and gently pinching it around the lid to secure the nesting material in place.
- Euthanize the neonatal mice separated in step 4.6 according to local institution requirements.
5. Titration of the cecal slurry
- Challenge the mice at the desired challenge dose (section 3) and monitor the outcomes (section 4).
- Observe whether the final outcome results in the desired LD, and if not, repeat sections 3 and 4 with a new litter at a higher or lower challenge dose, adjusting it by 5%-10%.
NOTE: Challenge doses may be similar to Figure 1B but need to be titered in each facility and strain of mice. - Also, observe whether the mice achieve a humane endpoint faster or slower than the expected kinetics in Figure 1B, and repeat sections 3 and 4 with a new litter at a higher or lower challenge dose, adjusting it by 5%-10%.
Results
Cecal slurry viability stored at -80 °C can be tested over time by serially diluting and plating aliquots of cecal slurry stock on 5% sheep's blood tryptic soy agar followed by 24 h of aerobic incubation at 37 °C. Subsequent counting of culturable colony-forming unit (CFU) content of a cecal slurry preparation was found not to change over a 6 month period, and the viability was not affected by prolonged storage at -80 °C (Figure 2). Each donor mouse resulted, on average, in enough cecal slurry to challenge three to four litters (data not shown).
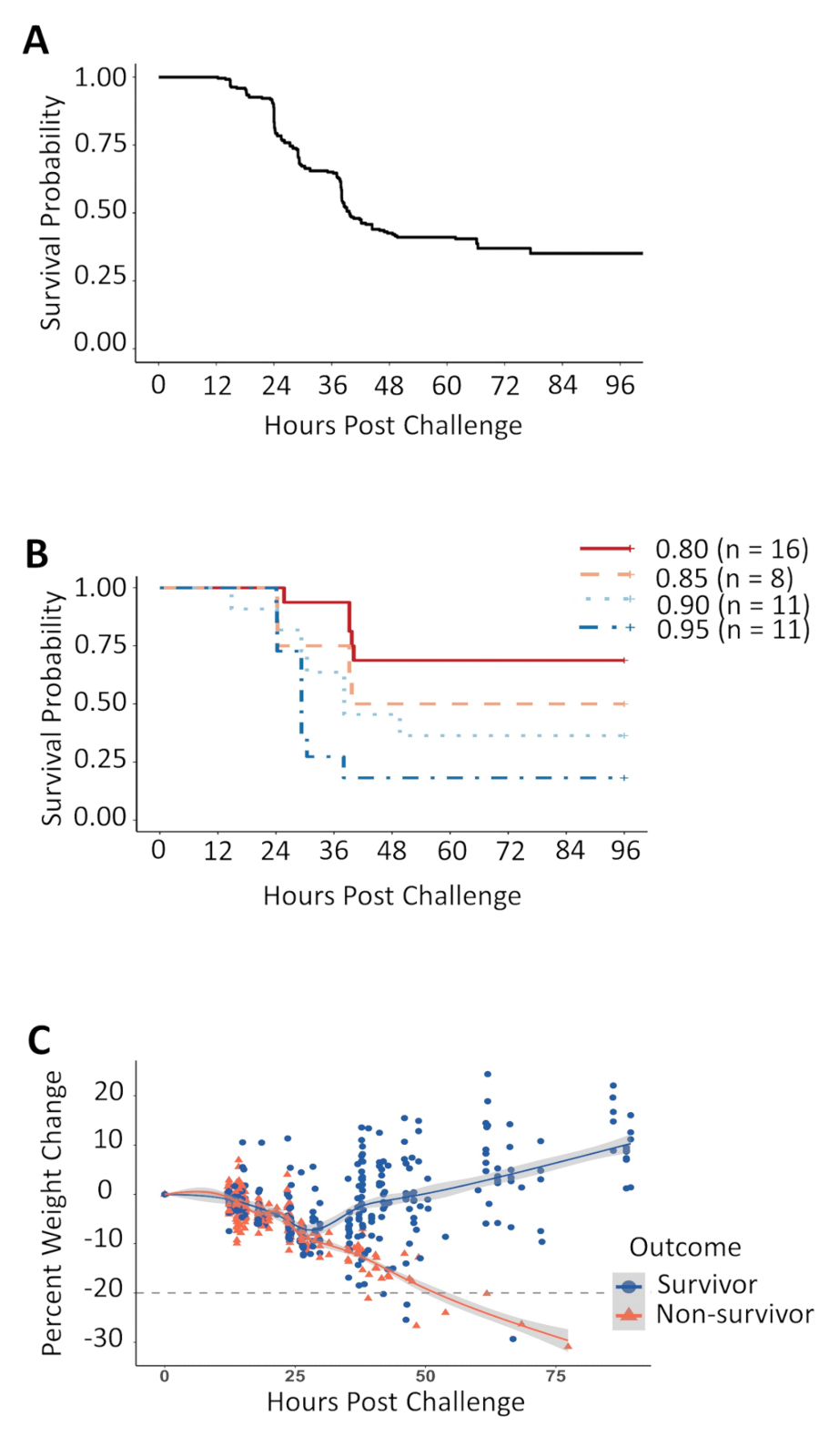
Mice challenged at DOL 7 with cecal slurry to induce polymicrobial sepsis began to reach the humane endpoint within 12 h of the challenge, and polymicrobial sepsis was mostly resolved by 48 h postchallenge, as observed in a Kaplan-Meier survival curve combined from data from over 200 challenged mice (Figure 1A). The lethality was dependent on the challenge dose administered, with a 5% change in challenge dose resulting in a roughly 15% difference in survival rate (Figure 1B). The mouse body weight was measured at each monitoring visit. Weight loss was seen in all challenged animals, being nondiscriminatory between mice that ended up surviving and those that did not during the initial 24 h postchallenge (Figure 1C). After 24 h, most surviving animals began to regain their weight, while all nonsurvivors continued to lose weight and moved to their humane endpoint. However, a small proportion of surviving animals that had retained their righting reflex also continued to lose weight or failed to gain weight, until the end of the experiment, even losing as much as 20% of their initial body weight within 40 h of the challenge. As there was an overlap of weight loss between mice that ended up surviving and those that did not, the change in weight or a threshold of weight loss could not be used as a criterion for humane endpoint while still maintaining the goal of accurately dividing survivors from nonsurvivors.
The behavior of mice was monitored as outlined in the protocol and in Table 2. Snapshots of the health categories are displayed (Figure 3A-C). These photos show the different health categories of mice who failed to right themselves after being placed on their back and outline the difference between FTR-Mobile and FTR-Lethargic, which is an important distinction. Unchallenged healthy mice of this age do not display FTR-Lethargic activity; therefore, this health category is a marker of disease and a response to challenge. Sick mice displayed FTR-Lethargic symptoms (Figure 3B) and could regress toward FTR-Nonmobile (Figure 3C), where the upper leg remains parallel with the bottom leg, with little to zero hip rocking movement, which is one of the criteria for humane endpoint. The mice might also recover, gaining increased hip movement and becoming FTR-Mobile (Figure 3A). The righting reflex and mobility scores were determined for both the left and right side of each mouse, and the highest score was utilized to determine whether the mouse had reached a humane endpoint. Behavioral information was collected from over 240 animals challenged with a lethal dose 60 (LD60) of cecal slurry, and 144 humane endpoints were observed (Figure 3D-F and Table 1). This evidence-driven approach was used to define and refine the humane endpoint across four disease stages, categorized by the experimenters based on both behavioral differences between survivors and nonsurvivors and by the fraction of humane endpoints reached during each time frame. During early experiments, FTR-Nonmobile mice that had no hip movement were consistently found dead within 4-6 h of this behavior being observed. In the collection of the presented information, an FTR-Nonmobile health score was used as criterion for a humane endpoint. From 12-21 h postchallenge, while FTR-Nonmobile mice were euthanized, both surviving and nonsurviving animals displayed very similar behavioral patterns and could not be distinguished in any other way (Figure 3D). From 21-48 h postchallenge, the majority of surviving mice regained their righting reflex, while fewer than 1% of the FTR behaviors observed were in animals that would go on to survive the experiment (Figure 3E). Thus, mice that failed to right themselves from both sides became an additional criterion for humane endpoint during this time. Between 12 and 20 h postchallenge, 12.5% of the total number of humane endpoints were observed, versus 80.5% between 20 and 48 h, and 7% after 48 h (Table 1). A distinguishing feature between mice that ended up surviving and that eventually worsened to a humane endpoint was the loss of the righting reflex, independent of hip mobility (Figure 3F). Indeed, between 20 and 48 h after the challenge, a total of 121 mice had failed to right themselves from both sides, with 116 of these mice eventually progressing to a humane endpoint (which represents a 96% accuracy in identifying mice that would not recover). Beyond 48 h after the challenge, 11 mice were observed to fail to right themselves from both sides, and 10 of these progressed to a humane endpoint (a 91% accuracy). Beyond 20 h after the challenge, the number of mice that lost the righting reflex for both sides predicts the final outcome with an accuracy of more than 90%; therefore, this has been added to the humane endpoint criteria, to identify nonrecovering mice earlier and reduce mouse suffering (Table 1).
The frequency that mice need monitoring changes over time, due to different rates of death postchallenge, and is outlined in Table 1. A mouse was considered to be at its humane endpoint at any point if it had failed to right itself and displayed nonmobile hip movement on both sides, or if the mouse was found scattered from the nest, was unable to right itself, and had lethargic hip movement. Mice with either of these conditions were not expected to be able to rejoin the litter and have been observed to be FTR-Nonmobile within 4-6 h. Starting 20 h after the challenge, a new humane endpoint was added because the presented information shows that the vast majority of mice that FTR from both sides ends up succumbing to disease.
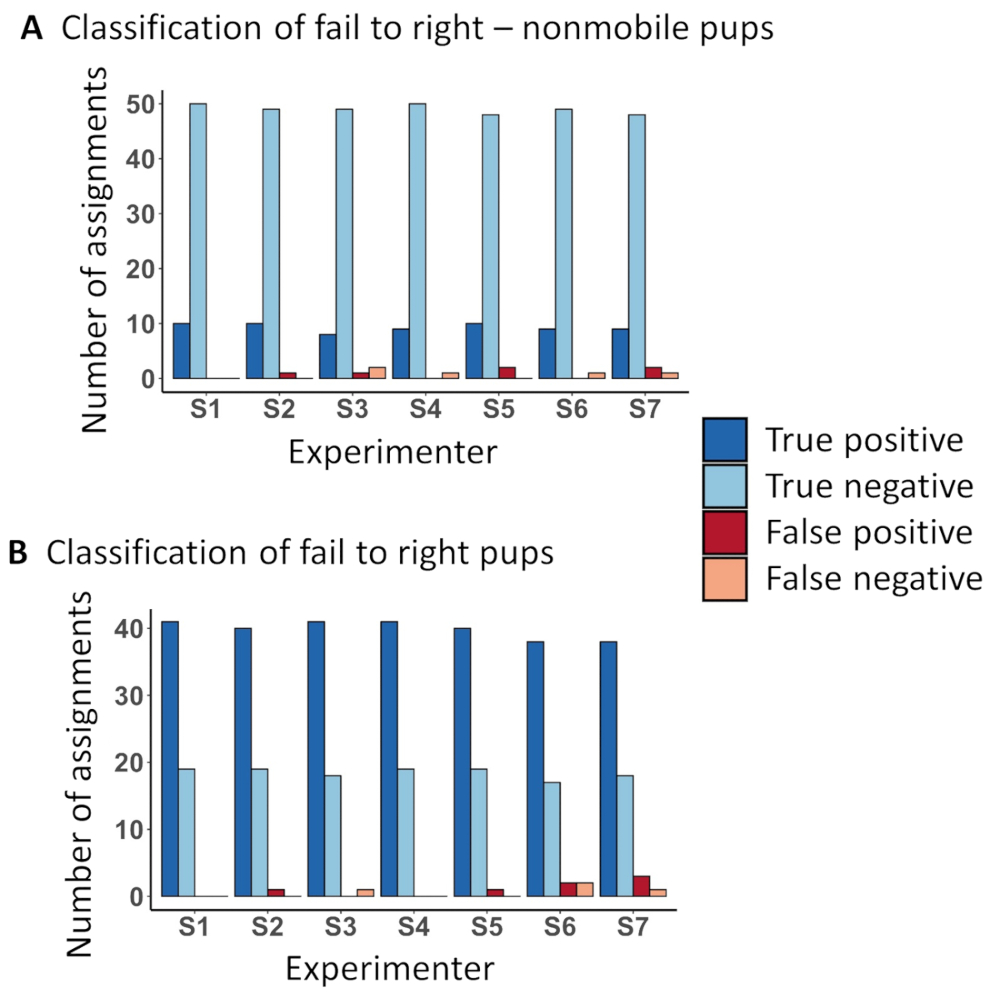
The videos, tables, and resources presented in this manuscript are an effective teaching resource for the correct behavioral assignment of challenged mice. Seven experimenters were asked to watch the training video and read both the protocol and the tables before assigning behaviors to 60 challenged animals. The identification of humane endpoint assignment was accurate both for distinguishing FTR-Nonmobile mice from mice that displayed the other behaviors (Figure 4A) and FTR mice from mice that were able to right themselves within the allowable time frame (Figure 4B).

Figure 1: Kaplan-Meier survival curve, cecal slurry dose titration, and weight change following the cecal slurry challenge. (A) Survival outcome of neonatal C57BL/6J mice challenged with an intraperitoneal cecal slurry injection at DOL 7. The data for this figure were combined from independent experiments using multiple challenge doses, ranging from 0.7 to 1.3 mg of cecal slurry per gram body weight was administered to these mice. (B) Neonatal mice challenged with 0.80 to 0.95 mg of cecal slurry per gram body weight from one cecal slurry preparation display a dose-dependent relationship between the amount of cecal slurry given and the percentage of survival.(C) The percentage of change in weight compared to the challenge weight, with the dotted line denoting a 20% loss of weight from the time of the challenge. Please click here to view a larger version of this figure.
{kind=link}

Figure 2: CFU concentration in cecal slurry stock stored at -80 °C does not change over a 6 month period. The effect of the cecal slurry age on CFU concentration was tested using linear regression. Each point represents one aliquot of the same cecal slurry preparation, serially diluted and plated over a 6 month period. Please click here to view a larger version of this figure.
{kind=link}

Figure 3: Hip mobility categories of mice that fail to right themselves and of animal behaviors at various times postchallenge. Mice that have been challenged with sepsis, when placed on their back, will display signs of morbidity that can be measured by the degree of hip movement. (A) A fail to right (FTR)-Mobile mouse shows hip rocking movement of their upper leg exceeding 90° angle from horizontal. (B) An FTR-Lethargic mouse shows hip rocking movement but does not exceed 90° angle from horizontal at any point during the 4 s of monitoring. (C) Some FTR-Nonmobile mice will extend their leg, bending at the knee, but will show very little (less than 10° angles) to zero hip rocking movement, and the legs will remain parallel to each other. (D) Animal behaviors 12-21 h postchallenge show that only FTR-Nonmobile behaviors separate survivors from nonsurvivors. (E) From 21 to 48 h postchallenge, only 4 out of the 592 observed FTR behaviors (0.67%) belong to survivors, allowing the righting reflex to predict the final outcome and be used as a new criterium for humane endpoint. (F) Beyond 48 h postinfection, 6 out of 131 mice (4.55%) that had a righting reflex went on to become part of the FTR group and were sacrificed by the end of the experiment, justifying sustained monitoring throughout the course of recovery. Please click here to view a larger version of this figure.
{kind=link}

Figure 4: Instructional resources result in accurate behavioral classification by independent experimenters. Experimenters trained by watching video accompanying this protocol categorized videos of 60 neonatal mice into different health groups. (A) The ability to distinguish a humane endpoint was determined and an average of 97% of behaviors was accurately categorized as FTR-Nonmobile or not, while only 1% of FTR-Nonmobile mice were misidentified. Two percent of the mice were falsely identified as FTR-Nonmobile. (B) The identification of the second humane endpoint criterium of correctly distinguishing between FTR mice or those having the ability to right themselves within 4 s of being placed on their back was assigned correctly in 97% of the scorings, while only 0.96% of the mice were incorrectly assigned as righting themselves and 2% of mice were incorrectly assigned as FTR. Please click here to view a larger version of this figure.
{kind=link}
| Disease Stage | A: High morbidity, no mortality | B: High morbidity, low mortality | C: High morbidity, high mortality | D: Low morbidity, low mortality |
| Hours post challenge | 0−12 | 12−20 | 20−48 | >48 |
| Monitoring frequency | 2 h post challenge | every 4−6 h | Every 4−6 h, 8 h, unattended overnight | 1−2 times daily, more if needed |
| Proportion of total humane endpoints observed | 0/144 | 18/144 | 116/144 | 10/144 |
| Percentage of humane endpoints observed | 0% | 12.5% | 80.5% | 7% |
| Humane endpoint criteria | 1. FTR−Nonmobile on both sides | 1. FTR−Nonmobile on both sides | ||
| 2. Scattered from nest and is FTR−Lethargic | 2. Scattered from nest and is FTR−Lethargic | |||
| 3. FTR on both left or right side (with any mobility score) | ||||
Table 1: Frequency of monitoring and humane endpoint criteria in the different stages of disease. Monitoring frequency, humane endpoints observed, the percentage of humane endpoints, and humane endpoint criteria during different stages of disease.
| Righting Reflex | Mobility | Time limit to right after being placed on back | Time limit to measure amount of movement (mobile / lethargic / nonmobile) | Mobility scoring Criteria |
| Rights | Mobile | 4 s | An additional 8 s | The mouse takes multiple steps in a row, maintaining forward momentum, and explores its environment. Pup will not fall over. |
| Lethargic | The mouse can take a step but will stop and pause before taking another. Pup may fall over. | |||
| Nonmobile | The mouse does not take any steps after righting itself. Pup may fall over. | |||
| Fail to right | Mobile hips | The same 4 s used to measure righting reflex | Has energetic hip movement with the upper leg rotating beyond 90° from horizontal at least once within 4 s. | |
| Lethargic hips | Hip movement up to but not beyond 90° from horizontal. | |||
| Nonmobile hips | Limbs may move by extending and retracting but the hips will not rotate. Pup looks very sickly. |
Table 2: Monitoring table and criteria in determining the health score of mice. The provided criteria were used to define health category groups to mice, and to reduce individual variance in assigning health scores.
Discussion
Postnatal neonatal mice have very limited mobility and fail to right themselves after being placed on their back, even when unchallenged. By DOL 7, the age of mice challenged in this model, a range of movement spanning from Rights-Mobile to FTR-Mobile was observed in unchallenged mice, with an important difference, namely that an unchallenged mouse at this age did not display FTR-Lethargic behavior. Only mice challenged with polymicrobial sepsis were observed to become FTR-Lethargic; therefore, this response can be a marker of disease severity. Being attentive to the cutoff of a 90° angle from horizontal for hip movement allows for the consistent and accurate assignment of lethargic or mobile hip movement in mice. The time frame of 4 s to see if a mouse can right itself was selected because unchallenged mice were able to consistently right themselves within this time frame. Repeated measurement of the same mouse was avoided, while the time to right themselves and the measurement of hip mobility was limited to 4 s, to avoid excessively tiring the mouse, which could otherwise affect its ability to obtain food and warmth and could affect its prognosis to get better. Righting itself from both the left and the right side were observed, and the higher of the scores was used to determine if the mouse was at a humane endpoint, because some mice were found to display FTR-Nonmobile on one side yet have a higher mobility on the other side and be able to recover eventually.
The scoring system used to evaluate mouse health relied on the application of categorical cutoffs to what is a spectrum of movement and, therefore, could be prone to individual bias. Staff was trained together to ensure each person scored the mice the same; however, there will likely remain a level of subjectivity leading to variation. The consistency of scoring was evaluated by having seven researchers who had not previously performed the neonatal mouse monitoring learn the requirements outlined in this protocol and video and, then, independently assign behaviors and determine humane endpoint. A 97% accuracy was observed with scoring performed on 60 challenged mice, suggesting that individual bias does not play a substantial role in the behavioral assignments of this model. The presented behavioral monitoring protocol is based on observations of animals challenged on DOL 7, yet mice younger than 6 days in an unchallenged healthy state cannot consistently right themselves. Thus, the described humane endpoint criteria could not be applied directly to younger mice. If younger mice are used in this experimental model or if a different challenge model with different disease kinetics is applied, then suitable humane endpoint criteria must be developed and piloted to avoid the euthanasia of mice that would otherwise, eventually, recover. The scoring system displays a robust method of improving humane endpoint classification that, with testing and confirmation, could potentially be applied to other models.
Each preparation of cecal slurry or the use of a new mouse strain required the retitration of the cecal slurry dose to administer to achieve a similar lethal dose. Each preparation was standardized by the readout of interest, namely survival, rather than giving the same bacterial count. Each cecal slurry preparation's viable bacterial concentration varied slightly, potentially due to differences in the donor's commensal bacteria or due to variances in the weight left in the cell strainer of the cecal slurry stock postfiltration. During the titration of the cecal slurry, the first two litters were divided into two groups and each half of the litter were challenged with one of the two doses so that each of the doses would be tested in two litters. If the resulting survival rate did not match the required level, then the challenge dose was either increased or decreased by 5%-10% and the experiment repeated. Multiple litters were used to account for litter-to-litter differences that could cause resistance or increased susceptibility to sepsis across a litter. It was important to accurately titer the cecal slurry stock with each new preparation to ensure that the new titration of cecal slurry was comparable to previous cecal slurry preparations. Periods of excess noise and vibration, specifically during the compacting of asphalt and the construction of a nearby building and road, were observed to increase stress in the dams. This correlated with increased rates of cannibalization, and affected the mortality of the survival experiments, even affecting unchallenged mice, indicating that there can be extraneous impacts on neonatal survival that also need to be controlled for.
Prior methods for cecal slurry stock preparation included either the use of fresh cecal slurry or the preparation of frozen cecal slurry, using a variety of methods, including the storage in glycerol that would inevitably be transferred during the challenge. While the use of fresh cecal slurry provides the advantage of having a bacterial composition closest to original cecal contents, there is the risk of variance between individual donor mice due to the variation of commensal bacteria. While this was minimized by using cecal donors from the same vendor with minimal time between arrival and progression of the experiment, this could become a cost-prohibitive option for some laboratories and presented another timing logistics challenge in having age-matched mice available when commencing a cecal slurry experiment in neonatal mice that were 7 days old. An alternative method to using fresh cecal slurry was utilized, where multiple adult donors' cecal contents were pooled, resuspended in D5W, frozen at -80 °C without glycerol, and thawed one aliquot at a time for experiments. The utilization of adult donor cecal slurry to study neonatal sepsis could potentially transfer species of bacteria present in the cecal slurry that the neonatal mouse has not been exposed to, but it is a strategy that allows for the study of sepsis in neonatal mice and has been used to study neonatal mouse biology in the past13,14,15. Cecal slurry was diluted in D5W to provide nutrition to the bacteria, which allowed the establishment of an active infection once the bacteria were injected, and was done to mimic the availability of nutrients in the peritoneal cavity during necrotizing enterocolitis. Glycerol was not included as a stabilizing agent in freezing bacteria because of the potential negative side effects that could arise from glycerol injection alone. If glycerol had been included in the cecal slurry preparation, then the potential damage that glycerol alone could induce would need to be tested for by including a glycerol-only (lacking cecal slurry) injection in mice, which would have increased mouse usage. The bacteria viability of the cecal slurry stocks was tested after freezing the cecal slurry stock without glycerol and was found to be constant, with no change in bacteria concentration in separate aliquots of the same cecal slurry preparation stored at -80 °C over a 6 month period. This suggests that the storage without glycerol is feasible in providing a consistent biological outcome. The use of a bulk-prepared frozen cecal slurry stock also allowed for the use of mice bred in-house, reducing cost and utilizing male mice that would otherwise be excess from breeding, therefore reducing mouse wastage.
The identification of failed challenges in mice was important to avoid adding extra noise to the system. After undergoing an intraperitoneal injection of cecal slurry, the mice were observed for the presence of a bulge underneath the skin, which indicated a failed injection that was actually subcutaneous. Mice were observed for leaks at the injection site, both immediately after needle removal and after allowing them to take a step after the injection, because mice would sometimes (rarely) leak only after moving the limb of the injection site by taking a step. The presence of a bulge or leak following the injection resulted in removing the mouse from the analysis. After all, either of these could result in a different outcome due to the incorrect amount of cecal slurry injected as a 5% difference in challenge dose has been observed to affect subsequent survival.
Cecal slurry challenge experiments often required varying target lethal doses with varying weight-adjusted doses. Due to this, injection volumes can range from as little as 20 µL and up to 100 µL. The proportionate experimental error associated with dead needle volume also changes along with the injection volume, increasing the difficulty to directly compare different doses. With the simple modification of standardizing the injection volume, this source of variance is removed from the experiment.
The neonatal mouse's behavioral monitoring system used in this protocol is the first of its kind. Researchers intent on conducting ethical research with newborn mice are often faced with the challenging lack of resources to assess the animal's well-being at this age. The presented intuitive and consistent monitoring system begins to address this knowledge gap. Importantly, this evidence-driven approach not only increases the quality of the experimental data obtained but, at the same time, also reduces the suffering of the experimental animals.
Disclosures
Dr. James Wynn receives support from the National Institutes of Health (NIH)/National Institute of General Medical Sciences (R01GM128452) and the NIH/Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) (R01HD089939).
Acknowledgements
Special thanks to Claire Harrison and the Animal Care Facility at British Columbia Children's Hospital Research Institute (BCCHR) for their support in the animal work, as well as to Dr. Po-Yan Cheng for their guidance and input on animal monitoring and well-being.
Materials
| Name | Company | Catalog Number | Comments |
| 0.1 - 20 μL pipette tips | VWR | 732-0799 | |
| 1.8 mL Microcentrifuge tube | Costar | 3621 | |
| 100 - 1000 μL pipette tips | VWR | 732-0801 | |
| 1 - 200 μL pipette tips | VWR | 732-0800 | |
| 15 mL Centrifuge tube | FroggaBio | TB15-25 | |
| 23G1 needles | Becton Dickinson | 305145 | only the needle, not the syringe, used for pinning mouse to styrofoam |
| 28G 0.5 mL Insulin syringe | BD | 329461 | |
| 2 mL Cryogenic vial | Corning | 430488 | |
| 50 mL Centrifuge tube | Fisher scientific | 14-432-22 | |
| 5 mL pipette | Costar | 4487 | |
| 6 - 10 week old C57BL/6J adult mice | Jackson Laboratories | 664 | |
| 7 + day old C57BL/6J neonatal mice | Bred in house | n.a | |
| 70 μm Cell strainer | Falcon | 352350 | |
| Defibrinated Sheep's Blood | Dalynn | HS30-500 | |
| Dextrose 5% Water (D5W) | Baxter | JB0080 | |
| Dissecting forceps | VWR | 82027-386 | |
| Dissecting Scissors, Sharp Tip | VWR | 82027-592 | |
| Dissecting Scissors, Sharp/Blunt Tip | VWR | 82027-594 | |
| Ethanol (HistoPrep 95% Denatured Ethyl Alcohol) | Fisherbrand | HC11001GL | diluted to 70% with double distilled water |
| Ethanol-proof marker; Lab marker | VWR | 52877-310 | |
| EZ Anesthesia Vaporizer | EZ Anesthesia | EZ-155 | |
| Germinator 500, Dry sterilize surgicial instrument (Hot bead sterilizer) | Braintree Scientific | GER 5287-120V | |
| Isoflurane | Fresenius Kabi | CP0406V2 | |
| Micro Spatula | Chemglass | CG-1983-12 | |
| Pipette-Aid | Drummond | 4-000-100 | |
| Rainin Classic Pipette PR-1000 | Rainin | 17008653 | |
| Rainin Classic Pipette PR-20 | Rainin | 17008650 | |
| Rainin Classic Pipette PR-200 | Rainin | 17008652 | |
| Scale | Sartorius | BL 150 S | |
| Specimen forceps | VWR | 82027-440 / 82027-442 | |
| Square 1000 mL Storage Bottle | Corning | 431433 | |
| Styrofoam board | Any | n.a | |
| Sure-Seal Mouse/Rat euthanasia chamber | Euthanex | EZ-178 | |
| Tryptic Soy Agar | Sigma-Aldrich | 22091-2.5KG | |
| VX-200 Lab Vortex Mixer | Labnet International | S0200 | |
| weigh paper | Fisherbrand | 09-898-12B |
References
- Liu, L., et al. Global, regional, and national causes of child mortality in 2000-13, with projections to inform post-2015 priorities: an updated systematic analysis. The Lancet. 385 (9966), 430-440 (2015).
- Wynn, J. L., et al. Increased mortality and altered immunity in neonatal sepsis produced by generalized peritonitis. Shock. 28 (6), 675-683 (2007).
- Fink, M. P. Animal models of sepsis. Virulence. 5 (1), 143-153 (2014).
- Wynn, J. L., et al. Defective innate immunity predisposes murine neonates to poor sepsis outcome but is reversed by TLR agonists. Blood. 112 (5), 1750-1758 (2008).
- Cuenca, A. G., et al. Critical role for CXC ligand 10/CXC receptor 3 signaling in the murine neonatal response to sepsis. Infection and Immunity. 79 (7), 2746-2754 (2011).
- Gentile, L. F., et al. Protective immunity and defects in the neonatal and elderly immune response to sepsis. Journal of Immunology. 192 (7), 3156-3165 (2014).
- Cuenca, A. G., et al. Delayed emergency myelopoiesis following polymicrobial sepsis in neonates. Innate Immunity. 21 (4), 386-391 (2015).
- Gentile, L. F., et al. Improved emergency myelopoiesis and survival in neonatal sepsis by caspase-1/11 ablation. Immunology. 145 (2), 300-311 (2015).
- Wynn, J. L., et al. Targeting IL-17A attenuates neonatal sepsis mortality induced by IL-18. Proceedings of the National Academy of Sciences of the United States of America. 113 (19), E2627-E2635 (2016).
- Fallon, E. A., et al. Program Cell Death Receptor-1-Mediated Invariant Natural Killer T-Cell Control of Peritoneal Macrophage Modulates Survival in Neonatal Sepsis. Frontiers in Immunology. 8, 1469(2017).
- Young, W. A., et al. Improved survival after induction of sepsis by cecal slurry in PD-1 knockout murine neonates. Surgery. 161 (5), 1387-1393 (2017).
- Rincon, J. C., et al. Adjuvant pretreatment with alum protects neonatal mice in sepsis through myeloid cell activation. Clinical & Experimental Immunology. 191 (3), 268-278 (2018).
- Starr, M. E., et al. A new cecal slurry preparation protocol with improved long-term reproducibility for animal models of sepsis. PLoS ONE. 9 (12), e115705(2014).
- Hansen, L. W., et al. Deficiency in milk fat globule-epidermal growth factor-factor 8 exacerbates organ injury and mortality in neonatal sepsis. Journal of Pediatric Surgery. 52 (9), 1520-1527 (2017).
- Fujioka, K., et al. Induction of heme oxygenase-1 attenuates the severity of sepsis in a non-surgical preterm mouse model. SHOCK. 47 (2), 242-250 (2017).
- Al Asmari, K. A., et al. Protective effect of quinacrine against glycerol-induced acute kidney injury in rats. BMC Nephrology. 18, PMC5273840(2017).
- Geng, X., et al. Differences in gene expression profiles and signaling pathways in rhabdomyolysis-induced acute kidney injury. International Journal of Clinical and Experimental Pathology. 8 (11), 14087-14098 (2015).
- Kim, J. H., et al. Macrophage depletion ameliorates glycerol-induced acute kidney injury in mice. Nephron Experimental Nephrology. 128 (1-2), 21-29 (2014).
- Nara, A., et al. Evaluations of lipid peroxidation and inflammation in short-term glycerol-induced acute kidney injury in rats. Clinical and Experimental Pharmacology and Physiology. 43 (11), 1080-1086 (2016).
- Zager, R. A., Johnson, A. C. M., Lund, S., Hanson, S. Acute renal failure: determinants and characteristics of the injury-induced hyperinflammatory response. American Journal of Physiology Renal Physiology. 291 (3), F546-F556 (2006).
- Olfert, E. D., Godson, D. L. Humane Endpoints for Infectious Disease Animal Models. Institute for Laboratory Animal Research Journal. 41 (2), 99-104 (2000).
- Canadian Council on Animal Care. Guidelines on: choosing an appropriate endpoint in experiments using animals for research, teaching and testing. , https://www.ccac.ca/Documents/Standards/Guidelines/Appropriate_endpoint.pdf (1998).
- Nemzek, J. A., Xiao, H. Y., Minard, A. E., Bolgos, G. L., Remick, D. G. Humane endpoints in shock research. SHOCK. 21 (1), 17-25 (2004).
- Morton, D. B. A systematic approach for establishing humane endpoints. Institute for Laboratory Animal Research Journal. 41 (2), 80-86 (2000).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved