
需要订阅 JoVE 才能查看此. 登录或开始免费试用。
Method Article
皮下三瓣阀修复期间回声导的简化步进方法
摘要
本协议详细介绍了如何在转导器膜瓣膜修复过程中执行实时超声心动图指导。对程序的每个阶段都描述了基本观点和必要的测量结果。
摘要
皮质转导器边缘到边缘重建的三叶虫瓣膜是一种安全和成熟的治疗严重症状性皮质回流的患者与手术风险高。除了氟镜检查外,心电图指导是黄金标准,应采用标准化技术进行。
本文介绍了我们可重复的逐步声心电图指南,包括视图、测量以及突出过程中可能出现的困难。
本文为程序的每一步提供详细和按时间顺序排列的声心电图视图,尤其是 2D 和 3D 成像之间的首选项。如果需要,将描述脉冲波、连续波和彩色多普勒测量。此外,由于没有关于在皮边到边缘修复过程中量化线粒体回流的官方建议,因此在掌握线粒体传单和设备部署后,还包括了对超声心动图量化的建议。此外,本文还处理重要的回声心电图视图,以防止和处理手术过程中可能出现的并发症。
转导器三阀修复期间的回声心动图指导是强制性的。结构化方法可改善干预者和成像师之间的协作,对于安全有效的程序至关重要。
引言
三位一体性复发(MR)是欧洲第二频繁的瓣膜手术。未经治疗,它可能导致严重的心力衰竭和生活质量下降2,3,4。皮下皮瓣膜修复 (PMVR) 是一种基于导管的技术,它模仿阿尔菲耶里缝合手术方法,通过连接 A2 和 P2 扇贝5进行皮质修复。对于手术风险高的患者,该技术为治疗严重MRI提供了一种微创方法。 来自多个登记处和试验的数据表明,MitraClip程序,一种转导器三瓣修复疗法,是一种有效和安全的方法6,7,8,9。2019年,一种类似的设备PASCAL导管阀维修系统被引入市场。在治疗严重M10病人时,已显示出可行性及可接受的安全性。PMVR 的持续时间和成功取决于单个操作员的技能和经验11。与其他皮下技术相比,如皮外转体置换(TAVR),它只能用荧光镜检查,PMVR需要回声心电图指导12,13。
本文逐步描述了 PMVR 期间的回声心动图方法,包括测量、MR 的校内量化建议以及防止近视并发症的重要观点。
Access restricted. Please log in or start a trial to view this content.
研究方案
该协议遵循我们机构的人类研究伦理委员会的指导方针。
1. 干预前的评估
- 在转射穿刺前排除腹产。如果存在小腹腔溢出,则测量四室 (4Ch) 视图中的最大端舒张回声发光空间,重点是右心室 (RV)、中食管右心室流入流出视图和长轴 (LAX) 视图。
- 评估左上肺静脉脉冲波多普勒 (PW) 的肺静脉流动模式,并排除左心房附属物 (LAA) 中的血栓形成。以 LAA 为重点显示短轴 (SAX) 视图,然后以 40-60° 的速度扫过,然后逆时针旋转探头以显示 LUPV。通过以 90-110° (图 1 和补充图 1)清扫来评估右上肺静脉 (RUPV) 的流量。

图1:修改后的SAX视图:左上肺静脉的PW流量 请点击这里查看此图的较大版本。
{kind=link}
- 在程序前和程序后评估期间,确保血液状态相同。
注:由于MM是一种动态瓣膜疾病,在全身麻醉下,反流可能看起来不那么严重。在这种情况下,请咨询操作员并增加后加载和/或预加载。 - 查找最佳对讲视图(50-70°)。在有色多普勒和无彩色多普勒的三个部分中拍摄垂直视图 (X 平面),并测量后部三叶虫传单 (PML) 的长度。然后,再次检查传单形态(图2和补充图2)。

图2:2D双平面视图的MV与彩色多普勒:中等不足喷气机 请点击这里查看这个数字的较大版本。
{kind=link}
- 在长轴视图 (120-140°) 中,使用连续波多普勒 (CW) 评估传输压力梯度。
注:平均压力梯度 (MPG) > 5 mmHg 是 PMVR 的相对禁忌。 - 以带彩色多普勒的 3D 数据集或带颜色的宽段缩放图像为例,测量 3D-vena 合约 (3D-VCA) (图 3)。

图3:带彩色多普勒的3D数据集的多平面重建:3D-Vena合约 请点击这里查看此图的较大版本。
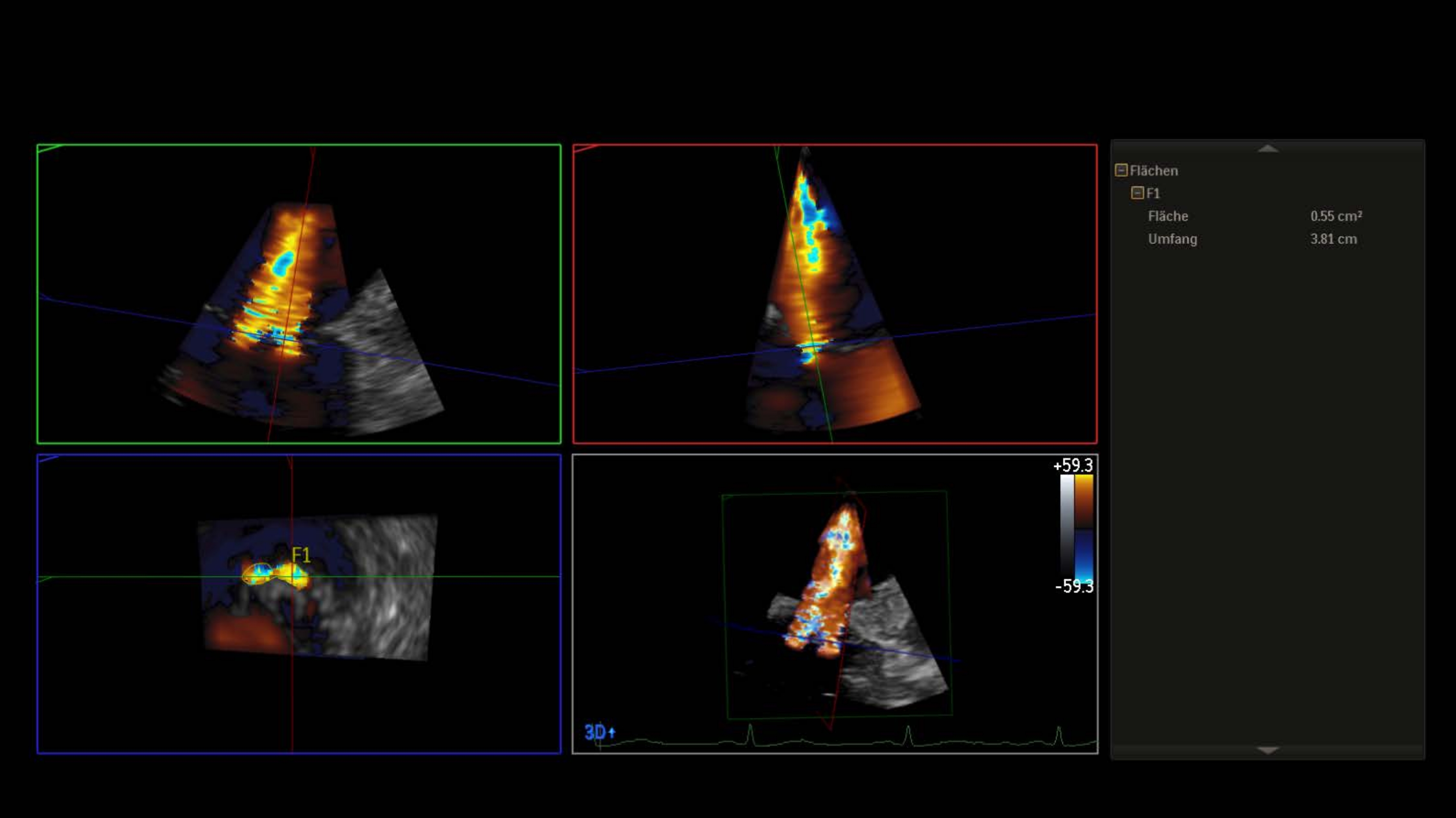{kind=link}
- 无颜色,使用 3D 音量测量三元阀区 (MVA) (补充图 3)。
注:4厘米2< 区域是相对禁忌症,面积<3厘米2 为绝对禁忌症来执行手术。否则,在跨胃基底 SAX 视图中评估 MVA。 - 显示子宫瓣膜的 3D 面部手术中庭视图(12 点的主动脉瓣)。
注:阀门段被命名为"横向",用于段 1,将命名为段 3 的"介质"。面部手术视图中段的序列与小卖部视图中的序列相反。顺时针旋转 180° 进入 3D en 面手术视图(6 点钟主动脉瓣),这将导致两个视图中的段数相等(图 4和图 5)。

图4:宽段缩放图像:3D内脸手术主审视图(主动脉瓣在12点) 请点击这里查看此图的较大版本。
{kind=link}

图5:宽段缩放图像:3D内脸审美视图(主动脉瓣在6点) 请点击这里查看此图的较大版本。
{kind=link}
- 最后,用 X 平面查看双壳视图 (90-110°),以显示主动脉瓣 (AV),用于转世穿刺。
2. 战略
- 在将可引导导管 (SGC) 和夹子递送系统 (CDS) 插入左中庭之前,与操作员讨论策略。
- 评估一个设备策略,如果孔<1厘米宽,并放置夹子正上方的回流喷射,如果孔是圆形的。
- 评估在大型椭圆形或多个喷射的情况下植入≥ 2 个夹子的情况。植入设备开始介质的回流孔,因为第二个设备的定位往往更容易,当第一个已经以这种方式植入,而不是横向启动后(补充图4)。
3. 转位穿刺
- 显示双壳视图与 SAX 视图相结合。确保 AV 可见,避免主动脉损伤。
- 确保穿刺部位稍优,后部(图6)。

图6: 2D双平面视图:转产穿刺 请点击这里查看此图的较大版本。
{kind=link}
- 选择4-5厘米的穿刺高度,以防退行性MM(如脱垂)和功能MRI的>3.5厘米。避免专利前椭圆形,因为条目太前。
- 一旦转世针导致午间隔膜的帐篷,测量在半鼻孔的4Ch视图穿刺高度(补充图5)。
注:在大阿提里亚的患者中,如果穿刺地点太后,帐篷在4Ch视图中无法可视化。在这种情况下,反光和插入深探针到食道。 - 转世穿刺后,始终排除4Ch视图中的腹膜扩散。
- 显示以 LAA 和肺静脉为重点的 SAX 视图,以可视化硬导线进入 LUPV。
4. 将 SGC 引入洛杉矶
- 通过连续的 2D 回声心电图和荧光引导,在 SAX 视图中与减速器一起可视化 SGC 的帐篷和推进,以避免左心房壁受伤。
注:SGC的尖端由无线电和回波明亮的双环(补充图6)定义。 - 向操作员显示 SAX 视图和双腔视图 (90-120°),以便将 SGC 定位在左心室 (LV) 的方向。
5. 将 CDS 推进到洛杉矶
- 采取3D卷,包括间歇隔膜,左侧脊和MV,并确保左侧脊是可见的,因为CDS的突出是常见的(图7)。

图7: 宽段缩放图像: SGC 在洛杉矶包括间歇隔膜, 左侧脊和 MV 请点击这里查看此图的较大版本.
{kind=link}
- 否则选择 SAX 视图和 LAX 视图 (X 平面) 以确保 CDS 不会与山脊和 LA 墙接触。
注:操作员可能会要求成像仪显示机际隔膜,并拉回 SGC 几毫米绕过山脊。如果无法可视化 3D 中的双环,则切换到 2D 并在 SAX 视图中显示 SGC。
- 检查 CDS 是否垂直于协调线的位置,以保证正确的轨迹。
- 在 ca. 60° 以 2D 显示对讲视图,以显示介质 - 横向平面和 LAX 视图(120-140°),以识别 MV 的前 - 后平面(补充图 7)。
- 或者优化 CDS 在 3D en-face 视图中的介质、横向、前部和后置位置(补充图 8)。
6. MV 上方和下方设备的方向
- 以 3D enface 视图显示手臂与套接线的垂直定位。
- 如果图像质量差,将显示对讲视图与 LAX 视图(图 8 和图 9)相结合。

图8: MV的双平面视图:设备在三元阀上的定位 请点击这里查看此图的较大版本。
{kind=link}

图9:宽段缩放图像:设备在三元阀上的定位 请点击这里查看此图的较大版本。
{kind=link}
注:夹臂仅在 LAX 视图中可见。
- 调整中间和横向定位设备的对讲视角,以可视化两臂的完整长度。在介质定位设备的 ca. 30-45° 下扫荡,对横向定位的设备扫荡 70-90°。
- 选择对讲视图与 LAX 视图相结合,可视化 CDS 向 LV 的推进。
- 确保 CDS 仅位于 MV 下方几毫米处。
- 在 3D en-face 视图中验证剪辑臂仍处于计划位置,因为夹子在穿过阀门时频繁旋转。
注:如果夹臂的位置发生变化,将顺时针或逆时针旋转以获得对称的抓握。在此操作中要小心,以尽量减少和弦和子弦纠缠。 - 如果设备需要进行粗放重新定位,则使用 X 平面显示对讲视图,以可视化将检索到 LA 的剪辑的反转。
7. 掌握夹子部署前后的三叶板传单和 MR 评估
- 将传单的抓地力记录在与 LAX 视图 (X 平面) 或仅在 LAX 视图(补充图 9)中相结合的对讲视图中。
- 请麻醉师进行呼吸控制,以减少通风过程中的移位,并便于掌握传单。
- 确保传单插入的连续可视化,以避免传单或和弦滚动。
注:抓握卷传单或和弦可能导致部分传单分离和/或 MR 的恶化。 - 在剪辑部署之前仔细评估回流减少。确保操作员和成像师同时分析这一关键步骤。
- 将 TEE 探头中间和横向旋转到剪辑中,或使用带有彩色多普勒的 X 平面来查找靠近剪辑的偏心喷射器(补充图 10)。
注:由于CDS低估MM造成的阴影伪影可能会发生。将探针插入食道深处,或显示横向视图,可视化残余不足喷射器,而不会遮盖文物。 - 评估肺静脉中的 PW 流量。
注意:如果以前的收缩流反转更改为收缩管主导模式,则可能已发生相关减少。 - 测量整个膜瓣膜的MPG。
注:梯度>5 mmHg是剪辑部署的相对禁忌症(补充图11和补充图12)。 - 使用MV的3Den面视图或MV的跨胃SAX视图来显示双孔(图10)。
- 将 TEE 探头中间和横向旋转到剪辑中,或使用带有彩色多普勒的 X 平面来查找靠近剪辑的偏心喷射器(补充图 10)。

图10:宽段缩放图像:设备部署后MV的双孔 请点击这里查看此图的较大版本。
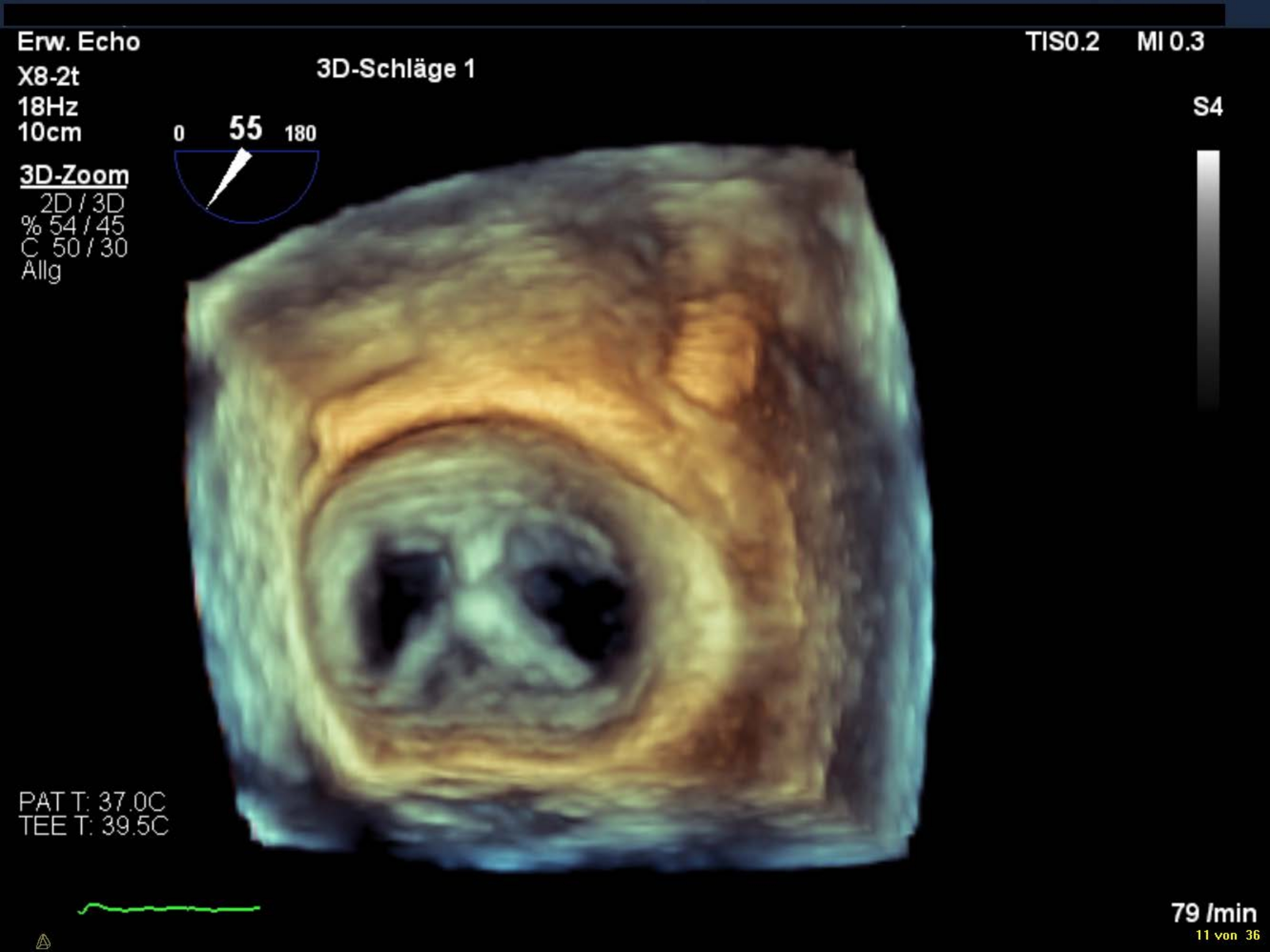{kind=link}
- 最后,如果结果令人满意,请检查 2D 中的传单插入。
- 从 CDS 中释放剪辑后,重复最后五个步骤。
注意:由于 MV 上的系统紧张,释放设备后的残余不足喷射器可能会加重。 - 显示何时用 X 平面从 LAX 视图中的 SGC 检索送货导管尖端,并确保峰值避免与 LA 接触(补充图 13)。
8. 最终 MR 评估
- 显示带彩色多普勒的对讲视图,如果存在,则与残余不足喷射器中的垂直 X 平面相结合。
- 在 3D 卷中计算 3D-VCA。注意:通常孔不在同一平面上。在这种情况下,测量在适当的平面上每个孔的分离平面(补充图14)。
- 再次评估肺静脉流动和整个内膜瓣膜的平均梯度。
注:连续 LA 压力监测可能是转导器膜瓣修复过程中的有用工具。 - 最后,显示三维内阀的 3D 面视图。
9. 植入其他设备
- 确保 MR 减少足够。
注意:如果结果不尽如人意,请评估其他设备的植入情况。 - 确保附加设备不会接触潜入左心室的植入设备。
注意:荧镜检查对于显示剪辑之间的真实距离至关重要。 - 显示 3D en-face 视图以可视化导体线,因为植入第一个剪辑后可能会推迟。
- 重复第 7.4 点中解释的五个步骤,在用附加剪辑抓握传单后评估 MR。
Access restricted. Please log in or start a trial to view this content.
结果
皮质边缘到边缘瓣膜修复是手术瓣膜修复或替代患者不符合有症状的严重MRI手术的替代方案。在血管内瓣边缘到边缘修复研究I(EVERESTI)14试验中,对MitraClip的首次临床应用进行了调查。许多其他试验已经证明了程序的有效性,症状的改善,以及低率的医院死亡率和不良事件(ACCESS EU,TRAMI,EVEREST II)15,16,17。<...
Access restricted. Please log in or start a trial to view this content.
讨论
PMVR 的回声引导是一种安全的方法。由于声心动图引起的并发症可能发生,但很少导致重大损害。然而,食管病变是可能的后,执行食管超声心动图。这种发生率在干预34的较短时间内减少。相反,与转导器边缘到边缘三边瓣膜修复相关的几个并发症被描述为35,36。大出血是输血后最常见的主要并发症,输血过程一直与死亡率
Access restricted. Please log in or start a trial to view this content.
披露声明
作者没有什么可透露的。
致谢
我们感谢多萝西娅·舍伦女士的技术视频支持。
Access restricted. Please log in or start a trial to view this content.
材料
| Name | Company | Catalog Number | Comments |
| EPIQ 7 Ultrasound System | Philips | US218B0542 | Cardiac Ultrasound Machine |
| X8-2t xMATRIX 3D-TEE probe | Philips | B34YYK | TEE-probe |
| Sheath 6F 25 cm | Merit Medical | B60N25AQ | Sheath |
| Dilator 16 F | Abbott | 405544 | Dilator |
| BRK-1 transseptal needle 71 cm | St. Jude Medical | ABVA407201 | Transseptal Needle |
| Swartz Lamp 90° | St. Jude Medical | 407356 | Transseptal Guiding Introducer Sheath |
| Amplatz super stiff | Kook Medical | 46509 | Wire |
| Steerable Guide Catheter | Abbott | SGC0302 | Steerable Guide Catheter |
| MitraClip NTR Delivery System | Abbott | CDS0602-NTR | Clip Delivery System |
| MitraClip NTR Bundle | Abbott | MSK0602-NTR | Device |
参考文献
- Iung, B., et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. European Heart Journal. 24 (13), 1231-1243 (2003).
- Hauptman, P. J., Rector, T. S., Wentworth, D., Kubo, S. Quality of life in advanced heart failure: role of mitral regurgitation. American Heart Journal. 151 (1), 213-218 (2006).
- Lewis, E. F. Assessing the impact of heart failure therapeutics on quality of life and functional capacity. Current Treatment Options in Cardiovascular Medicine. 15 (4), 425-436 (2013).
- Vaishnava, P., Lewis, E. F. Assessment of quality of life in severe heart failure. Current Heart Failure Reports. 4 (3), 170-177 (2007).
- Feldman, T., et al. Percutaneous repair or surgery for mitral regurgitation. New England Journal of Medicine. 364 (15), 1395-1406 (2011).
- Feldman, T., et al. Percutaneous mitral repair with the MitraClip system: safety and midterm durability in the initial EVEREST (Endovascular Valve Edge-to-Edge REpair Study) cohort. Journal of the American College of Cardiology. 54 (8), 686-694 (2009).
- Whitlow, P. L., et al. Acute and 12-month results with catheter-based mitral valve leaflet repair: the EVEREST II (Endovascular Valve Edge-to-Edge Repair) High Risk Study. Journal of the American College of Cardiology. 59 (2), 130-139 (2012).
- Baldus, S., et al. MitraClip therapy in daily clinical practice: initial results from the German transcatheter mitral valve interventions (TRAMI) registry. European Journal of Heart Failure. 14 (9), 1050-1055 (2012).
- Stone, G. W., et al. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. New England Journal of Medicine. 379 (24), 2307-2318 (2018).
- Lim, D. S., et al. Transcatheter Valve Repair for Patients With Mitral Regurgitation: 30-Day Results of the CLASP Study. JACC: Cardiovascular Interventions. 12 (14), 1369-1378 (2019).
- Schillinger, W., et al. Impact of the learning curve on outcomes after percutaneous mitral valve repair with MitraClip and lessons learned after the first 75 consecutive patients. European Journal of Heart Failure. 13 (12), 1331-1339 (2011).
- Katz, W. E., Conrad Smith, A. J., Crock, F. W., Cavalcante, J. L. Echocardiographic evaluation and guidance for MitraClip procedure. Cardiovascular Diagnosis and Therapy. 7 (6), 616-632 (2017).
- Altiok, E., et al. Optimized guidance of percutaneous edge-to edge repair of the mitral valve using real-time 3-D transesophageal echocardiography. Clinical Research in Cardiology. 100 (8), 675-681 (2011).
- Feldman, T., et al. Percutaneous mitral valve repair using the edge-to-edge technique: six-month results of the EVEREST Phase I Clinical Trial. Journal of the American College of Cardiology. 46 (11), 2134-2140 (2005).
- Maisano, F., et al. Percutaneous mitral valve interventions in the real world: early and 1-year results from the ACCESS-EU, a prospective, multicenter, nonrandomized post-approval study of the MitraClip therapy in Europe. Journal of the American College of Cardiology. 62 (12), 1052-1061 (2013).
- Kalbacher, D., et al. Long-term outcome, survival and predictors of mortality after MitraClip therapy: Results from the German Transcatheter Mitral Valve Interventions (TRAMI) registry. International Journal of Cardiology. 277, 35-41 (2019).
- Glower, D. D., et al. Percutaneous mitral valve repair for mitral regurgitation in high-risk patients: results of the EVEREST II study. Journal of the American College of Cardiology. 64 (2), 172-181 (2014).
- Baumgartner, H., et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. European Heart Journal. 38 (36), 2739-2791 (2017).
- Obadia, J. F., et al. MITRA-FR Investigators. Percutaneous Repair or Medical Treatment for Secondary Mitral Regurgitation. New England Journal of Medicine. 379 (24), 2297-2306 (2018).
- Stone, G. W., et al. COAPT Investigators. Transcatheter Mitral-Valve Repair in Patients with Heart Failure. New England Journal of Medicine. 379 (24), 2307-2318 (2018).
- Vahanian, A., et al. Joint Task Force on the Management of Valvular Heart Disease of the European Society of Cardiology (ESC); European Association for Cardio-Thoracic Surgery (EACTS), Guidelines on the management of valvular heart disease (version 2012). European Heart Journal. 33 (19), 2451-2496 (2012).
- American College of Cardiology/American Heart Association Task Force on Practice Guidelines; Society of Cardiovascular Anesthesiologists; Society for Cardiovascular Angiography and Interventions. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 114 (5), 84(2006).
- Praz, F., et al. Compassionate use of the PASCAL transcatheter mitral valve repair system for patients with severe mitral regurgitation: a multicentre, prospective, observational, first-in-man study. Lancet. 390 (10096), 773-780 (2017).
- McCarthy, K. P., Ring, L., Rana, B. S. Anatomy of the mitral valve: understanding the mitral valve complex in mitral regurgitation. European Journal of Echocardiography. 11 (10), 3-9 (2010).
- Zoghbi, W. A., et al. Recommendations for Noninvasive Evaluation of Native Valvular Regurgitation: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Magnetic Resonance. Journal of the American Society of Echocardiography. 30 (4), 303-371 (2017).
- Zoghbi, W. A., et al. Guidelines for the Evaluation of Valvular Regurgitation Percutaneous Valve Repair or Replacement: A Report from the American Society of Echocardiography Developed in Collaboration with the Society for Cardiovascular Angiography and Interventions, Japanese Society of Echocardiography, and Society for Cardiovascular Magnetic Resonance. Journal of the American Society of Echocardiography. 32 (4), 431-475 (2019).
- Abudiab, M. M., Chao, C. J., Liu, S., Naqvi, T. Z. Quantitation of valve regurgitation severity by three-dimensional vena contracta area is superior to flow convergence method of quantitation on transesophageal echocardiography. Echocardiography. 34 (7), 992-1001 (2017).
- Dietl, A., et al. 3D vena contracta area after MitraClip procedure: precise quantification of residual mitral regurgitation and identification of prognostic information. Cardiovasc Ultrasound. 16 (1), 1(2018).
- Ikenaga, H., et al. Usefulness of Intraprocedural Pulmonary Venous Flow for Predicting Recurrent Mitral Regurgitation and Clinical Outcomes After Percutaneous Mitral Valve Repair With the MitraClip. JACC: Cardiovascular Interventions. 12 (2), 140-150 (2019).
- Tang, G. H. L., et al. Continuous invasive hemodynamic monitoring using steerable guide catheter to optimize mitraclip transcatheter mitral valve repair: A multicenter, proof-of-concept study. Journal of Interventional Cardiology. 31 (6), 907-915 (2018).
- Maor, E., et al. Acute Changes in Left Atrial Pressure After MitraClip Are Associated With Improvement in 6-Minute Walk Distance. Circulation: Cardiovascular Interventions. 10 (4), 004856(2017).
- Kuwata, S., et al. Continuous Direct Left Atrial Pressure: Intraprocedural Measurement Predicts Clinical Response Following MitraClip Therapy. JACC: Cardiovascular Interventions. 12 (2), 127-136 (2019).
- Corrigan, F. E., et al. Pulmonary Venous Waveforms Predict Rehospitalization and Mortality After Percutaneous Mitral Valve Repair. JACC Cardiovasc Imaging. 12 (10), 1905-1913 (2019).
- Ruf, T. F., et al. ELMSTREET (Esophageal Lesions during MitraClip uSing TRansEsophageal Echocardiography Trial. EuroIntervention. 13 (12), 1444-1451 (2017).
- Eggebrecht, H., et al. Risk and outcomes of complications during and after MitraClip implantation: Experience in 828 patients from the German TRAnscatheter mitral valve interventions (TRAMI) registry. Catheterization and Cardiovascular Interventions. 86 (4), 728-735 (2015).
- von Bardeleben, R. S., et al. Incidence and in-hospital safety outcomes of patients undergoing percutaneous mitral valve edge-to-edge repair using MitraClip: five-year German national patient sample including 13,575 implants. EuroIntervention. 14 (17), 1725-1732 (2019).
- Généreux, P., et al. Incidence, predictors, and prognostic impact of late bleeding complications after transcatheter aortic valve replacement. Journal of the American College of Cardiology. 64 (24), 2605-2615 (2014).
- Benito-González, T., Estévez-Loureiro, R., Gualis, J. Chordal Rupture Following MitraClip Implantation Resulting in Massive Mitral Regurgitation. Journal of Invasive Cardiology. 27 (10), 224-225 (2015).
- Kaneko, H., Neuss, M., Weissenborn, J., Butter, C. Impact of residual mitral regurgitation after MitraClip implantation. International Journal of Cardiology. 227, 813-819 (2017).
- Buzzatti, N., et al. What is a "good" result after transcatheter mitral repair? Impact of 2+ residual mitral regurgitation. Journal of Thoracic and Cardiovascular Surgery. 151 (1), 88-96 (2016).
- Feldman, T., Guerrero, M. Assessing the Balance Between Less Mitral Regurgitation and More Residual Transmitral Pressure Gradient After MitraClip. JACC: Cardiovascular Interventions. 10 (9), 940-941 (2017).
- Neuss, M., et al. Elevated Mitral Valve Pressure Gradient After MitraClip Implantation Deteriorates Long-Term Outcome in Patients With Severe Mitral Regurgitation and Severe Failure. JACC: Cardiovascular Interventions. 10 (9), 931-939 (2017).
- Katz, W. E., Conrad Smith, A. J., Crock, F. W., Cavalcante, J. L. Echocardiographic evaluation and guidance for MitraClip procedure. Cardiovascular Diagnosis and Therapy. 7 (6), 616-632 (2017).
- Labrousse, L., et al. Guidance of the MitraClip procedure by 2D and 3D imaging. Archives of Cardiovascular Diseases. 111 (6-7), 432-440 (2018).
- Khalique, O. K., Hahn, R. T. Percutaneous Mitral Valve Repair: Multi-Modality Cardiac Imaging for Patient Selection and Intra-Procedural Guidance. Frontiers in Cardiovascular Medicine. 6, 142(2019).
- Bushari, L. I., et al. Percutaneous Transcatheter Edge-to-Edge MitraClip Technique: A Practical "Step-by-Step" 3-Dimensional Transesophageal Echocardiography Guide. Mayo Clinic Proceedings. 94 (1), 89-102 (2019).
- Sherif, M. A., et al. MitraClip step by step; how to simplify the procedure. Netherlands Heart Journal. 25 (2), 125(2017).
- Guarracino, F., et al. Transesophageal echocardiography during MitraClip procedure. Anesthesia & Analgesia. 118 (6), 1188-1196 (2014).
- Avenatti, E., et al. Diagnostic Value of 3-Dimensional Vena Contracta Area for the Quantification of Residual Mitral Regurgitation After MitraClip Procedure. JACC: Cardiovascular Interventions. 12 (6), 582-591 (2019).
- Altiok, E., et al. Analysis of procedural effects of percutaneous edge-to-edge mitral valve repair by 2D and 3D echocardiography. Circulation: Cardiovascular Imaging. 5 (6), 748-755 (2012).
Access restricted. Please log in or start a trial to view this content.
转载和许可
请求许可使用此 JoVE 文章的文本或图形
请求许可探索更多文章
This article has been published
Video Coming Soon
版权所属 © 2025 MyJoVE 公司版权所有,本公司不涉及任何医疗业务和医疗服务。