
Auscultazione
Panoramica
Fonte: Jaideep S. Talwalkar,MD, Medicina interna e pediatria, Yale School of Medicine, New Haven, CT
Attraverso l'auscultazione, il clinico è in grado di "intercettare il funzionamento del corpo" per ottenere importanti informazioni diagnostiche. 1 Storicamente, il termine "auscultazione" era sinonimo di "auscultazione immediata", in cui l'orecchio dell'esaminatore veniva posto direttamente contro la pelle del paziente. Sebbene questa sia stata una pratica standard per secoli, il metodo si è rivelato inadeguato nella Francia del diciannovesimo secolo, a causa delle norme sociali e della resa diagnostica non ottimale. Ciò ha portato René Laënnec a inventare il primo stetoscopio nel 1816 (Figura 1), uno strumento che da allora è diventato inseparabile dall'auscultazione nella pratica clinica moderna, e i pazienti lo considerano un simbolo di onore e affidabilità tra coloro che li portano. 2
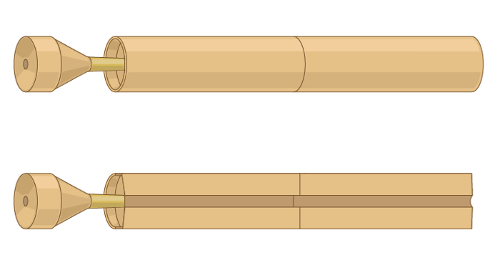
Figura 1. Un'illustrazione rappresentativa del primo stetoscopio inventato da René Laënnec.
Lo stetoscopio ha subito molti progressi tecnologici dall'iniziale tubo di legno cavo di Laënnec. In pratica, il fornitore deve capire la differenza tra i due lati del petto dello stetoscopio moderno: il diaframma e la campana (Figura 2).
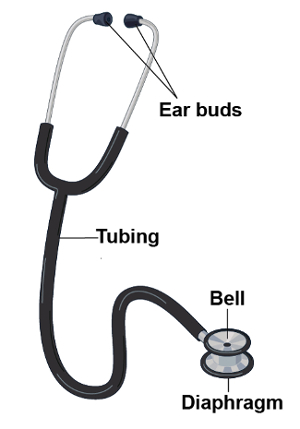
Figura 2. Parti di uno stetoscopio moderno.
Se applicato saldamente sulla pelle del paziente, il diaframma trasmette suoni ad alta frequenza. I suoni dall'interno del paziente vibrano la membrana del diaframma. Queste vibrazioni provocano la propagazione del suono attraverso la colonna d'aria all'interno dello stetoscopio e nelle orecchie dell'esaminatore. Al contrario, se applicata leggermente, la campana trasmette suoni a bassa frequenza. La campana agisce come una tazza che trasmette direttamente i suoni dall'interno del paziente attraverso il tubo dello stetoscopio. Premendo più saldamente con la campana può allungare la pelle sottostante, trasformandola essenzialmente in un diaframma. L'auscultazione è utilizzata in un'ampia varietà di contesti clinici. Più comunemente svolge un ruolo nell'esame del torace, del cuore, dell'addome e della vascolarizzazione.
Procedura
- Durante l'intero incontro con il paziente, utilizzare il senso dell'udito non assistito per identificare i risultati che possono essere diagnosticamente utili(ad esempio,voce rauca o grugnito con la scadenza).
- Prima del contatto con il paziente, decontaminare lo stetoscopio pulendolo con un pegno alcolico al 70%, un risciacquo antisettico standard utilizzato per l'igiene delle mani o un disinfettante per superfici ospedaliere. 3
- Posizionamento dello stetoscopio
- Posiziona gli auricolari de
Applicazione e Riepilogo
Questo video ha coperto le considerazioni generali relative all'auscultazione durante l'esame fisico. L'auscultazione viene in genere eseguita con l'aiuto di uno stetoscopio, anche se alcuni risultati, specialmente sull'esame respiratorio, possono essere evidenti all'orecchio non aiutato. Mentre le tecniche specifiche dello stetoscopio variano in base a ogni singola porzione dell'esame, in tutte le circostanze, il clinico deve tenere correttamente lo stetoscopio e riconoscere la differenza tra la campana e il diaframma a
Riferimenti
- Markel, H. The Stethoscope and the Art of Listening. New England Journal of Medicine. 354: 551-553 (2006)
- Jiwa, M., Millett, S., Meng, X., and Hewitt, V.M. Impact of the Presence of Medical Equipment in Images on Viewers' Perceptions of the Trustworthiness of an Individual On-Screen. Journal of medical Internet research. 14 (4), e100 (2012).
- Makim, D.G. Stethoscopes and Health Care-Associated Infection. Mayo Clinic Proceedings. 89: 277-280 (2014).
Vai a...
Video da questa raccolta:

Now Playing
Auscultazione
Physical Examinations I
62.3K Visualizzazioni

Approccio generale all'esame obiettivo
Physical Examinations I
117.6K Visualizzazioni

Osservazione e ispezione
Physical Examinations I
95.2K Visualizzazioni

Palpazione
Physical Examinations I
84.6K Visualizzazioni

Percussione
Physical Examinations I
101.8K Visualizzazioni

Adeguamento corretto dell'abbigliamento del paziente durante l'esame obiettivo
Physical Examinations I
83.5K Visualizzazioni

Misurazione della pressione sanguigna
Physical Examinations I
108.9K Visualizzazioni

Misurazione dei segni vitali
Physical Examinations I
115.1K Visualizzazioni

Esame obiettivo dell'apparato respiratorio I: ispezione e palpazione
Physical Examinations I
157.5K Visualizzazioni

Esame obiettivo dell'apparato respiratorio I: percussione e auscultazione
Physical Examinations I
213.2K Visualizzazioni

Esame obiettivo del cuore I: ispezione e palpazione
Physical Examinations I
176.8K Visualizzazioni

Esame obiettivo del cuore II: auscultazione
Physical Examinations I
140.1K Visualizzazioni

Esame obiettivo del cuore III: suoni cardiaci anormali
Physical Examinations I
91.9K Visualizzazioni

Esame obiettivo della vascolatura periferica
Physical Examinations I
68.9K Visualizzazioni

Esame vascolare periferico utilizzando un Doppler a onda continua
Physical Examinations I
38.6K Visualizzazioni
Personale delle biblioteche
Copyright © 2025 MyJoVE Corporation. Tutti i diritti riservati