Examen Respiratoire II: Percussion et auscultation
Source : Suneel Dhand, MD, médecin, médecine interne, Beth Israel Deaconess Medical Center de fréquentant
Apprendre la bonne technique pour percussion et l’auscultation de l’appareil respiratoire est indispensable et est livré avec pratique sur vrais patients. La percussion est une compétence utile qui est souvent ignorée lors de la pratique clinique quotidienne, mais si effectuée correctement, il peut aider le médecin à identifier la pathologie pulmonaire sous-jacente. L’auscultation peut fournir un diagnostic quasi immédiat pour un certain nombre de conditions pulmonaires aiguës, y compris la maladie pulmonaire obstructive chronique (MPOC), asthme, pneumonie et un pneumothorax.
Les domaines d’auscultating les poumons correspondent aux zones du poumon. Chaque lobe pulmonaire peut être photographié sous la paroi thoracique, au cours de percussion et l’auscultation ()Figure 1). Le poumon droit a trois lobes : le lobe supérieur, moyen et inférieur. Le poumon gauche a deux lobes : le lobe supérieur et inférieur. Le lobe supérieur du poumon gauche a également une projection séparée appelée le lingual.
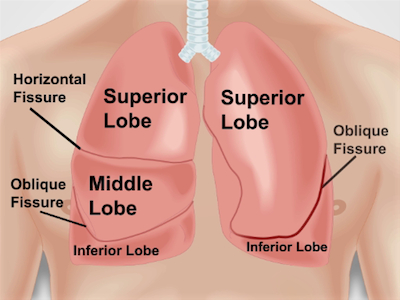
Figure 1. Anatomie des poumons à l’égard de la paroi thoracique. Une projection approximative des poumons et leurs fissures et lobes à la poitrine vers l’avant sur le mur. RUL - lobe supérieur droit ; RML - lobe moyen droit ; RLL - lobe inférieur droit ; LUL - lobe supérieur gauche ; LLL - lobe inférieur à gauche.
1. positionnement
- S’assurer que le patient est déshabillé jusqu'à la taille.
- Positionner le patient sur la table d’examen à un angle de 30 à 45 degrés et une approche du côté droit. Examen de la partie postérieure du poumon nécessite le patient à être penché vers l’avant ou s’asseoir sur le bord du lit.
2. percussion
- Percuss deux paramètre vers l’arrière et vers l’avant, commencer à l’arrière.
- Placer le main non-dominante avec milieu doigt (pl
Percussion et l’auscultation doivent toujours se faire dans l’ordre chaque fois qu’un examen respiratoire complet. Apprendre à percuss correctement prend du temps et pratique (pratique peut se faire sur vous-même ou d’autres surfaces, telles qu’une table). Notez comment la note de percussion change naturellement sur les poumons remplis d’air, côtes et des organes pleins, tels que le cœur.
L’auscultation doit être effectuée sur chaque zone de poumon pour donner au médecin l...
Passer à...
Vidéos de cette collection:

Now Playing
Examen Respiratoire II: Percussion et auscultation
Physical Examinations I
211.2K Vues

Approche générale à l’examen physique
Physical Examinations I
115.2K Vues

Observation et contrôle
Physical Examinations I
92.9K Vues

Palpation
Physical Examinations I
82.4K Vues

Percussions
Physical Examinations I
99.2K Vues

Auscultation
Physical Examinations I
60.0K Vues

Ajustement approprié de la tenue du patient pendant l'examen physique
Physical Examinations I
82.9K Vues

Mesure de la tension artérielle
Physical Examinations I
106.8K Vues

Mesure des signes vitaux
Physical Examinations I
113.5K Vues

Examen Respiratoire I: Inspection et palpation
Physical Examinations I
155.6K Vues

Examen cardiaque I : Inspection et palpation
Physical Examinations I
175.0K Vues

Examen cardiaque II: Auscultation
Physical Examinations I
139.0K Vues

Examen cardiaque III: Bruits cardiaques anormaux
Physical Examinations I
91.1K Vues

Examen vasculaire périphérique
Physical Examinations I
67.6K Vues

Examens vasculaires périphériques à l’aide d’un Doppler à onde continue
Physical Examinations I
38.3K Vues
À PROPOS DE JoVE
Copyright © 2025 MyJoVE Corporation. Tous droits réservés.