
需要订阅 JoVE 才能查看此. 登录或开始免费试用。
Method Article
经口内窥镜甲状腺切除术甲状腺叶切除术前庭入路甲状腺叶切除术
摘要
在这里,我们提出了一个协议来详细描述经口内窥镜甲状腺切除术前庭入路的方法。
摘要
手稿描述了用于甲状腺叶切除术的经口内窥镜甲状腺切除术前庭入路 (TOETVA)。将患者置于仰卧位,伸展并固定颈部。在对皮肤和口腔进行消毒后,通过口腔前庭的粘膜做一个20毫米的横向切口和两个5毫米的切口,用于放置相机和仪器。工作区由皮肤悬浮装置建立和维护,该装置由不可吸收的绳子(3-0)和橡皮筋以及CO2 吹气压力制成。使用内侧到外侧技术和预防性同侧中央颈清扫术同时对甲状腺状癌 (PTC) 患者进行肺叶切除术。通过20毫米切口提取标本。立即在标本中寻找甲状旁腺并自动移植到左臂桡骨。引流管通过牵开器孔插入甲状腺床,并使用可吸收缝合线关闭口腔前庭和白线宫颈的粘膜切口。建议在术后前 24 小时内静脉注射预防性药物,术后 7 天使用口服抗生素。
引言
传统的开放性甲状腺切除术已经使用宫颈切口安全进行了 100 多年1。尽管大多数患者具有有效的疤痕愈合,并且美容效果通常可以接受,但颈部的永久性疤痕总是引起普通观察者的立即注意2。近20%的甲状腺切除术后患者有自我意识,超过10%的患者考虑进一步治疗以去除疤痕3。此外,据报道,宫颈切口对健康相关生活质量(HRQOL)也有负面影响4。已经开发了各种用于甲状腺手术的远程访问方法,例如腋窝乳房、经腋窝、耳后和锁骨下方法,通过将皮肤切口移动到不太显眼的位置来避免可见的颈部疤痕5,6,7,8。9然而,这些方法需要宽瓣解剖才能进入甲状腺,并且仍然在切口部位留下皮肤疤痕10。
自2008年以来,已经开发了用于经口甲状腺手术的自然孔腔内镜手术技术。这些可以通过口腔前庭入路或舌下入路 进行 。前者更受欢迎,因为它与较少的并发症相关。2016年,Anuwong发表了第一个病例系列,纳入了60名接受经口内窥镜甲状腺切除术前庭入路术(TOETVA)的患者,并确定了良好的预后11。与远程访问方法相比,TOETVA被认为是真正的微创,因为皮瓣夹层的区域类似于传统的开放性甲状腺切除术,并且不会在身体上留下任何疤痕10。
TOETVA是一种革命性的内窥镜方法,可满足女性的美容需求,并可轻松进入双侧甲状腺和中央间室12。它的特点是中央淋巴结完全暴露和解剖,有利于用cN1a10,13,14,15治疗分化型甲状腺癌。然而,由于手术空间有限,处理甲状腺上极的大肿瘤相对具有挑战性。目前的研究描述了TOETVA的分步程序。
研究方案
该研究经四川大学华西医院医学伦理委员会批准(2018[457]),并取得所有受试者的书面知情同意。
1.术前准备
- 患者资格
- 选择对美容有严格要求并符合以下标准的患者:(1)良性结节直径<4cm;(2)分化型甲状腺癌(DTC)直径<2cm,临床无侧淋巴结转移或远处转移;(3)无中央淋巴结转移或转移性淋巴结直径<2cm且无融合和固定的影像学指征。
- 排除符合以下标准的患者:(1)髓样癌或未分化甲状腺癌;(2)口腔或颈部感染;(3)对甲状腺功能有急性影响的严重甲状腺炎;(4)原发肿瘤或转移性淋巴结可疑侵犯邻近器官,如食道、气管或喉返神经(RLN);(5)原发肿瘤在上极的位置;(6)既往颈部手术、消融术或颈部放疗史;(7)未控制的甲状腺功能亢进的生化证据;(8)胸骨后甲状腺肿;(9)对手术不耐受。
- 患者准备
- 术前通过细针穿刺细胞学检查、甲状旁腺检查、甲状腺功能检查、喉镜检查和甲状腺超声检查评估患者16.
- 要求患者在 TOETVA 考试前至少 2 天饭前饭后使用漱口水(如替硝唑)准备口腔,每次将漱口水在口中保持至少 15 秒。
- 设备
- 确保口腔伤口的可吸收缝合线(5-0)的可用性。
- 确保协议所需的所有仪器和材料的可用性(见 材料表)。
2. 手术准备
- 术前准备
- 根据美国麻醉医师协会的分类评估手术的麻醉风险17.
- 使用术中神经监测 (IONM) 进行口腔插管诱导全身麻醉。
- 用胶带粘住眼睛和鼻子,并垫住头部以避免无意中的创伤。
- 进行导尿。
- 操作字段
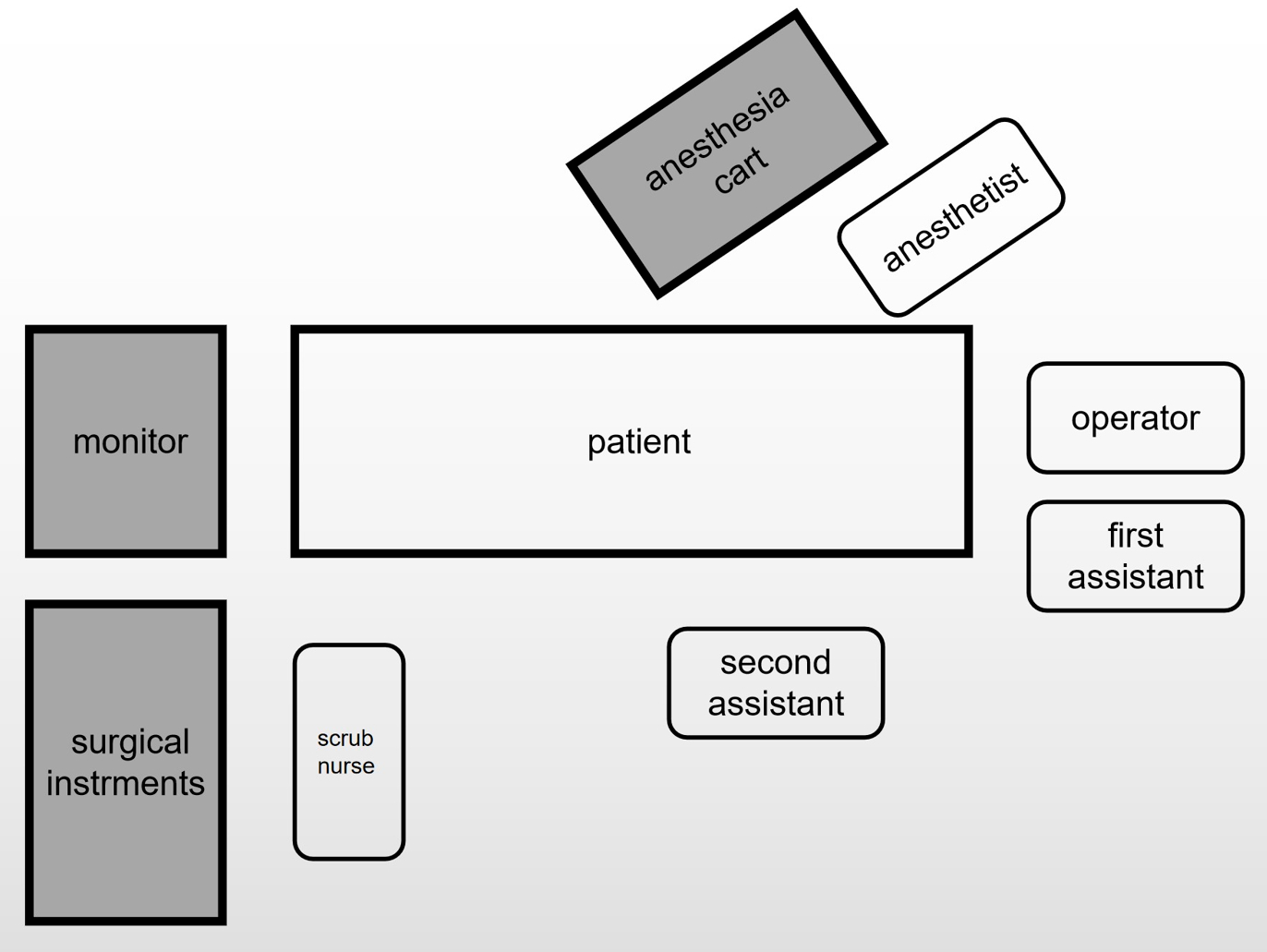
注意: 图1 显示了手术室布局的示意图。- 让操作员站在患者的头前。让第一助手站在患者头部的左侧。
注意:第一助手将负责握住内窥镜。 - 让第二助手根据病变的位置站在病人的身体旁边握住钩子。让擦洗护士站在病人的腿边。
- 将内窥镜设备并监测到患者脚外。
- 将患者置于仰卧位,颈部伸展。在手术过程中用顶部袖带固定患者的头部,以避免颈部旋转。
- 让操作员站在患者的头前。让第一助手站在患者头部的左侧。
- 消毒
- 皮肤消毒:根据自上而下和由外的原则,用碘溶液准备上胸部,颈部和下脸三次。
- 口腔消毒:将稀释后的碘纱布放入口中,用其消毒口腔三次,用生理盐水冲洗。

图 1:手术室布局示意图。 请点击此处查看此图的大图。
{kind=link}
3.设计切口并建立工作空间(图2)
- 用电切机切开相机端口切口;这应该是通过中央下唇前庭的肺泡粘膜在包皮系带上方 5 mm 处的 20 mm 横向切口。
- 用电切机将相机端口切口推进到下巴。注意避免进入薄膜皮肤。使用止血钳和皮下剥离杆在颈部中线开一条隧道,并进一步延伸到下颈部。
- 将 10 mm 摄像机穿过中央端口。用二氧化碳气体向工作空间注入压力,以建立 4 mmHg 的压力。
注意:二氧化碳气体的压力应为 <8 mmHg,以避免高压引起的并发症。 - 从第一前磨牙横向做两个 5 mm 垂直切口,用于放置器械。
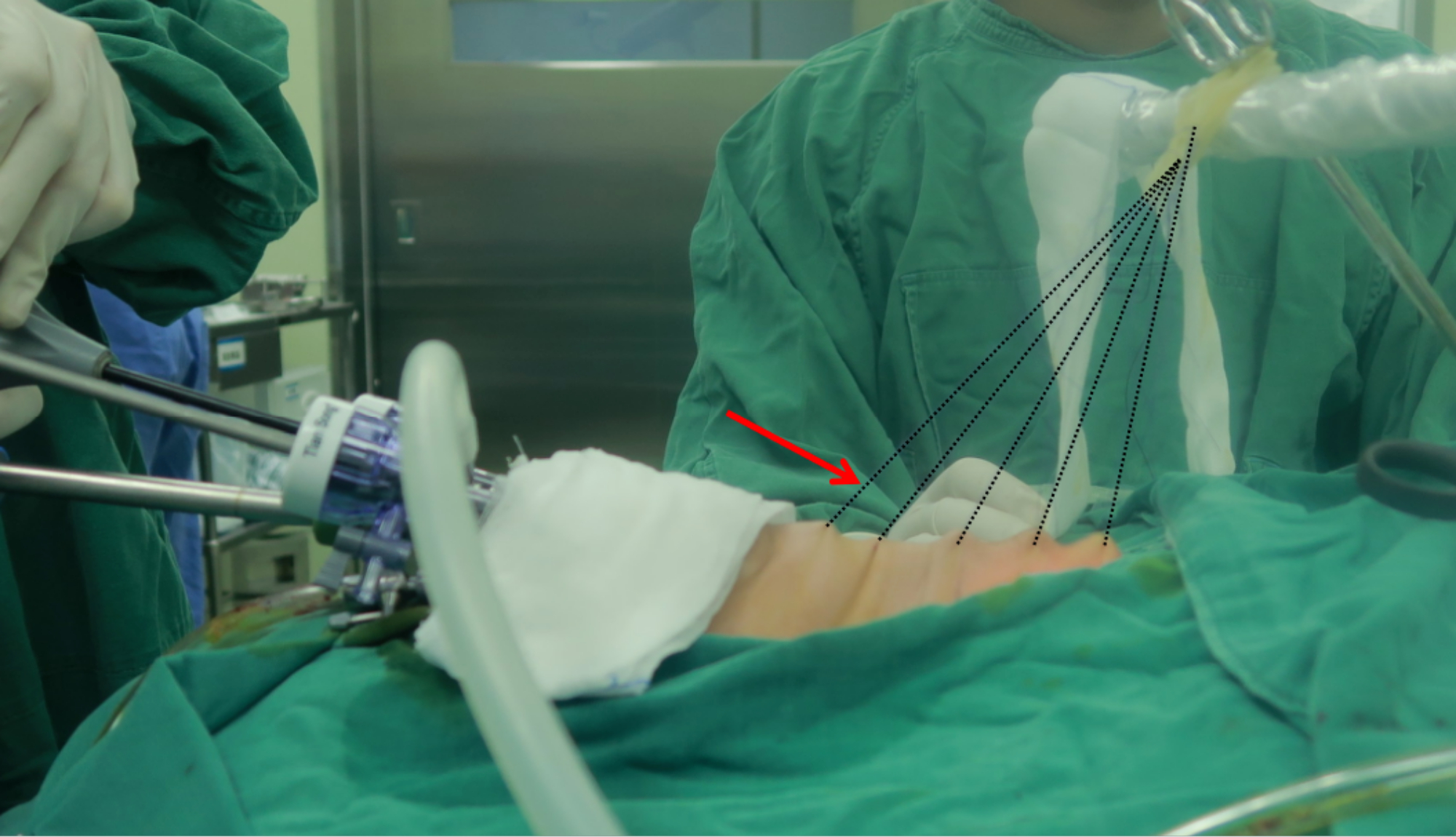
- 使用超声手术刀制造工作空间,并将其横向扩大到胸锁乳突肌两侧,并沿着板下平面扩大到胸骨下切口。使用由不可吸收缝合线(3-0)和橡皮筋制成的皮肤悬浮装置的牵引力来帮助扩大工作空间(图3)。

图2:患者和腹腔镜端口的位置。 中间一个是相机端口。臂I和臂II用于放置仪器。 请点击此处查看此图的大图。
{kind=link}

图 3:牵引悬架装置。 箭头指向牵引悬架装置。悬挂装置由不可吸收的绳子(3-0)和橡皮筋制成。 请点击此处查看此图的大图。
{kind=link}
4. 甲状腺叶切除术
- 用超声波手术刀分割大肠杆菌线。将部分带状肌与甲状腺分开。
- 使用 20 mL 针刺穿甲状腺软骨下角水平的皮肤,并将拉钩穿过孔。使用拉钩抓住带肌的分离部分。
- 使用超声手术刀分离带状肌肉的剩余部分并暴露颈总动脉。找到迷走神经,并使用IONM记录信号。
注意:IONM 技术有助于快速定位、识别和保护喉返神经 (RLN) 和喉上神经 (EBSLN) 的外支。鼓励使用IONM;它是一个很好的辅助工具,但不是强制性工具。 - 使用非创伤性镊子握住峡部下缘。使用超声手术刀从环状软骨的下部切开峡部并暴露气管。对于TOETVA的肺叶切除术,首先找到气管,并将其作为标志。
- 使用非创伤性镊子握住甲状腺的上极,并用超声手术刀分割环甲腔。横断部分胸骨肌。暴露甲状腺的上极。
- 切断甲状腺上动脉和静脉。从上到下释放侧腺。抬起腺体的上极,在直接可视化下找到RLN,并使用IONM记录信号。
- 使用超声手术刀将甲状腺囊与气管分开。分割甲状腺下血管,用超声波手术刀切断浆果韧带。
- 从气管中取出甲状腺的单侧叶。使用IONM再次记录迷走神经和RLN的信号。
5.中央淋巴结清扫术
- 首先找到下甲状旁腺,并尝试将其保留 在原位。
注意:应仔细识别和保护胸腺,以确保胸腺供应来源的甲状旁腺功能,并防止甲状旁腺意外切除。可以选择碳纳米颗粒来帮助识别甲状旁腺和清扫淋巴结。对于不能 原位保留的甲状旁腺,自体移植是可行的。 - 尽可能将带子肌肉向外拉伸,以充分暴露手术区域。
- 通过舌骨(上)、胸骨上窝(下窝)、颈动脉(外侧)、颈深筋膜浅层(前部)和食管(后部)识别中央淋巴结室。
- 使用超声手术刀解剖气管前和喉前淋巴结。切颈动脉前的结缔组织以确定中央淋巴结的侧边界,气管前的结缔组织以确定中央淋巴结的内侧边界。扫左RLN前侧或右RLN前侧和后侧,完成中央淋巴结清扫。
注意:侧缘不应扫得太深,以防止损伤迷走神经和交感神经干。清洁下缘时,应避免对无名血管和胸膜的伤害。
6. 取出试样并闭合
- 使用内窥镜袋取出标本。
注意:为避免异位植入,应通过内窥镜袋完全取出标本。 - 用大量温热的无菌蒸馏水反复清洗手术伤口。
- 通过颈部前部的小皮肤穿刺放置手术引流管(4#)。
- 重新近似带肌。用5-0可吸收缝合线关闭口腔伤口。
7.甲状旁腺自体移植
- 用生理盐水保留甲状旁腺,并通过冷冻切片活检进行检查。
- 用眼科剪刀将孤立的甲状旁腺切成 1 mm x 1 mm x 1 mm 的微小碎片。将碎片与生理盐水混合。将混合物注射到前臂的肱肌中。
结果
我们在中心为TOETVA患者建立了常规临床路径。手术前对每位患者进行喉镜检查和甲状腺超声检查。甲状旁腺激素(PTH)、甲状腺功能、25-二羟基维生素D(25-OH-VD)和血清钙在术前常规检测,除甲状腺功能外,所有甲状腺功能均在术后1天重新测定。在我们医院,Foley导管通常用于将进行TOETVA手术超过3小时的患者。Foley导管也在手术后1天移除。手术后,每位患者通过静脉滴注给予4g葡萄糖酸钙,并在?...
讨论
TOETVA的特征是中央淋巴结完全暴露和解剖,这在cN1a10,13,14,15治疗分化型甲状腺癌方面具有显着优势。但是,需要注意的是,由于手术空间有限,处理位于甲状腺上极的大肿瘤相对困难。应严格遵守手术适应症和禁忌症,确保手术安全开展。甲状腺上极完全脱位后,在手术过程中通过IONM监测直接可...
披露声明
作者声明没有竞争利益。
致谢
我们感谢所有参与这项研究的患者的合作。本研究得到了四川省科技厅项目基金的支持。(批准号:2021YFS0103)。
材料
| Name | Company | Catalog Number | Comments |
| Allis Grasping Forceps,310 mm x 5 mm | AESCULAP | PO111R | |
| Button Electrode Tip | AESCULAP | GK385R | |
| Ceramic Electrode | AESCULAP | GK384R | |
| Complete Trocar | AESCULAP | EJ751R | |
| Endoscope | Olympus | WA53005A | |
| IONM | Medtronic | NIM-3.0 | |
| Light Transmitting Bundle | Olympus | WA03310A | |
| Maryland Dissecting Forceps, 310 mm x 5 mm | AESCULAP | PO102R | |
| Monopolar Handle (5 mm diameter, 33 cm working length) | AESCULAP | GK372R | |
| Pneumoperitoneum tube,4 m | STRYKE | 620-240-223 | |
| Pyramidal Tip Obturator | AESCULAP | EJ755R | |
| Reusable Monopolar Cable | AESCULAP | GK245 | |
| Scissors | AESCULAP | P0004R | |
| Suction irrigation tube | AESCULAP | PG027R | |
| Super Righting Needle Holder, 5 mm | AESCULAP | PL414R | |
| Veress | TianSong | E2014.6 |
参考文献
- Latifi, R., et al. Outcomes of 1,327 patients operated on through twelve multispecialty surgical volunteerism missions: A retrospective cohort study. International Journal of Surgery. 60, 15-21 (2018).
- Liao, D., et al. Transoral neck surgery prevents attentional bias towards the neck compared to open neck surgery. Laryngoscope. 130 (6), 1603-1608 (2020).
- Best, A. R., Shipchandler, T. Z., Cordes, S. R. Midcervical scar satisfaction in thyroidectomy patients. Laryngoscope. 127 (5), 1247-1252 (2017).
- Choi, Y., et al. Impact of postthyroidectomy scar on the quality of life of thyroid cancer patients. Annals of Dermatology. 26 (6), 693-699 (2014).
- Kang, S. W., et al. Robotic thyroid surgery using a gasless, transaxillary approach and the da Vinci S system: The operative outcomes of 338 consecutive patients. Surgery. 146 (6), 1048-1055 (2009).
- Choe, J. H., et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World Journal of Surgery. 31 (3), 601-606 (2007).
- Inukai, M., Usui, Y. Clinical evaluation of gasless endoscopic thyroid surgery. Surgery Today. 35 (3), 199-204 (2005).
- Terris, D. J., Singer, M. C., Seybt, M. W. Robotic facelift thyroidectomy: II. Clinical feasibility and safety. Laryngoscope. 121 (8), 1636-1641 (2011).
- Russell, J. O., et al. Transoral thyroid and parathyroid surgery via the vestibular approach-a 2020 update. Gland Surgery. 9 (2), 409-416 (2020).
- Chai, Y. J., et al. Transoral endoscopic thyroidectomy for papillary thyroid microcarcinoma: Initial experience of a single surgeon. Annals of Surgical Treatment and Research. 93 (2), 70-75 (2017).
- Anuwong, A. Transoral endoscopic thyroidectomy vestibular approach: A series of the first 60 human cases. World Journal of Surgery. 40 (3), 491-497 (2016).
- Arora, A., et al. The perception of scar cosmesis following thyroid and parathyroid surgery: A prospective cohort study. International Journal of Surgery. 25, 38-43 (2016).
- Dionigi, G., Chai, Y. J., Tufano, R. P., Anuwong, A., Kim, H. Y. Transoral endoscopic thyroidectomy via a vestibular approach: Why and how. Endocrine. 59 (2), 275-279 (2018).
- Wang, Y., et al. Implementation of intraoperative neuromonitoring for transoral endoscopic thyroid surgery: A preliminary report. Journal of Laparoendoscopic and Advanced Surgical Techniques. Part A. 26 (12), 965-971 (2016).
- Wu, G. Y., et al. Endoscopic central lymph node dissection via breast combined with oral approach for papillary thyroid carcinoma: A preliminary study. World Journal of Surgery. 41 (9), 2280-2282 (2017).
- Yang, J., et al. Complete endoscopic thyroidectomy via oral vestibular approach versus areola approach for treatment of thyroid diseases. Journal of Laparoendoscopic and Advanced Surgical Techniques. Part A. 25 (6), 470-476 (2015).
- Su, A., et al. Does the number of parathyroid glands autotransplanted affect the incidence of hypoparathyroidism and recovery of parathyroid function. Surgery. 164 (1), 124-129 (2018).
- Doyle, D. J., Hendrix, J. M., Garmon, E. H. American Society of Anesthesiologists Classification. StatPearls. , (2022).
- Park, J. O., Kim, M. R., Kim, D. H., Lee, D. K. Transoral endoscopic thyroidectomy via the trivestibular route. Annals of Surgical Treatment and Research. 91 (5), 269-272 (2016).
- Dionigi, G., et al. Transoral endoscopic thyroidectomy: Preliminary experience in Italy. Updates in Surgery. 69 (2), 225-234 (2017).
- Udelsman, R., et al. Trans-oral vestibular endocrine surgery: A new technique in the United States. Annals of Surgery. 264 (6), 13-16 (2016).
- Choe, J. -. H., et al. Endoscopic thyroidectomy using a new bilateral axillo-breast approach. World Journal of Surgery. 31 (3), 601-606 (2007).
- Son, S. K., Kim, J. H., Bae, J. S., Lee, S. H. Surgical safety and oncologic effectiveness in robotic versus conventional open thyroidectomy in thyroid cancer: A systematic review and meta-analysis. Annals of Surgical Oncology. 22 (9), 3022-3032 (2015).
- Lee, K. E., et al. Robotic thyroidectomy by bilateral axillo-breast approach: Review of 1,026 cases and surgical completeness. Surgical Endoscopy. 27 (8), 2955-2962 (2013).
- Kim, M. J., et al. Yonsei experience of 5000 gasless transaxillary robotic thyroidectomies. World Journal of Surgery. 42 (2), 393-401 (2018).
- Jitpratoom, P., Ketwong, K., Sasanakietkul, T., Anuwong, A. Transoral endoscopic thyroidectomy vestibular approach (TOETVA) for Graves' disease: A comparison of surgical results with open thyroidectomy. Gland Surgery. 5 (6), 546-552 (2016).
- Yi, J. W., et al. Transoral endoscopic surgery for papillary thyroid carcinoma: Initial experiences of a single surgeon in South Korea. Annals of Surgical Treatment and Research. 95 (2), 73-79 (2018).
- Wang, D., et al. Transoral thyroidectomy vestibular approach versus non-transoral endoscopic thyroidectomy: A comprehensive systematic review and meta-analysis. Surgical Endoscopy. 36 (3), 1739-1749 (2022).
- Wang, T., et al. Safety of central compartment neck dissection for transoral endoscopic thyroid surgery in papillary thyroid carcinoma. Japanese journal of clinical oncology. 50 (4), 387-391 (2020).
- Sun, H., et al. Comparison of transoral endoscopic thyroidectomy vestibular approach, total endoscopic thyroidectomy via areola approach, and conventional open thyroidectomy: A retrospective analysis of safety, trauma, and feasibility of central neck dissection in the treatment of papillary thyroid carcinoma. Surgical Endoscopy. 34 (1), 268-274 (2020).
- Tanaka, K. Comparative study on bacterial flora of oral cavity and upper pharynx in healthy elderly. The Japanese Journal of Antibiotics. 54, 19-21 (2001).
- Guo, F., Wang, W., Zhu, X., Xiang, C., Wang, Y. Comparative study between endoscopic thyroid surgery via the oral vestibular approach and the areola approach. Journal of Laparoendoscopic and Advanced Surgical Techniques. 30 (2), 170-174 (2019).
- Chae, S., Min, S. Y., Park, W. S. Comparison study of robotic thyroidectomies through a bilateral axillo-breast approach and a transoral approach. Journal of Laparoendoscopic and Advanced Surgical Techniques. 30 (2), 175-182 (2020).
- Kim, W. W., et al. A comparison study of the transoral and bilateral axillo-breast approaches in robotic thyroidectomy. Journal of Surgical Oncology. 118 (3), 381-387 (2018).
- Nguyen, H. X., Long, T. N., Nguyen, H. V., Nguyen, H. X., Le, Q. V. Comparison of transoral thyroidectomy vestibular approach and unilateral axillobreast approach for endoscopic thyroidectomy: A prospective cohort study. Journal of Laparoendoscopic and Advanced Surgical Techniques. 31 (1), 11-17 (2020).
- Bhattacharyya, N. Surgical treatment of cervical nodal metastases in patients with papillary thyroid carcinoma. Archives of Otolaryngology - Head and Neck Surgery. 129 (10), 1101-1104 (2003).
- Lundgren, C. I., Hall, P., Dickman, P. W., Zedenius, J. Clinically significant prognostic factors for differentiated thyroid carcinoma: A population-based, nested case-control study. Cancer. 106 (3), 524-531 (2006).
转载和许可
请求许可使用此 JoVE 文章的文本或图形
请求许可探索更多文章
This article has been published
Video Coming Soon
版权所属 © 2025 MyJoVE 公司版权所有,本公司不涉及任何医疗业务和医疗服务。