
A subscription to JoVE is required to view this content. Sign in or start your free trial.
Method Article
Intravitreal Injections in the Ovine Eye
In This Article
Summary
Intravitreal injections were performed in the sheep eye with the aim of delivering viral-mediated gene therapy to the retina.
Abstract
There are several methods for the delivery of therapeutic agents to the retina, including intravitreal (IVT), subretinal, suprachoroidal, periocular, or topical administration. IVT drug delivery involves an injection into the vitreous humor of the eye, a gelatinous substance that fills the posterior chamber of the eye and maintains the shape of the eye globe. Although the IVT route is less specifically targeted than subretinal delivery, it is much less invasive and is widely used in clinical settings for a range of ocular diseases.
We previously demonstrated the efficacy of intravitreal delivery of an adeno-associated virus (AAV)-mediated gene therapy product (AAV9.CLN5) in sheep with a naturally occurring CLN5 form of neuronal ceroid lipofuscinosis (NCL). Affected sheep received IVT gene therapy in one eye, with the other untreated eye serving as an internal control. Retinal structure and function were maintained in the treated eye up to 15 months after treatment, while the untreated eye displayed progressively declining function and severe atrophy during postmortem examination. Based on the sheep studies, the CLN5 gene therapy product was cleared as a candidate investigational new drug (IND) by the United States Food and Drug Administration in September 2021. This paper details the surgical protocol for IVT delivery of a therapeutic viral vector to the ovine eye.
Introduction
Several methods can be used to deliver therapeutic agents to the retina, including intravitreal (IVT), subretinal, suprachoroidal, periocular, or topical administration. Each route of administration involves overcoming barriers such as the blood-retina barrier or the inner and outer limiting membranes and has varying rates of efficacy depending on the drug being delivered and the specific retinal target1,2.
IVT drug delivery involves an injection into the vitreous humor of the eye, a gelatinous substance that occupies the posterior chamber of the eye. The primary function of the vitreous humor is to maintain the shape of the eye globe and keep ocular tissues, such as the lens and retina, in place. The vitreous humor is composed largely of water, with small amounts of collagen, hyaluronic acid, and other noncollagenous proteins3. IVT injection is a simple and common procedure used routinely to treat a wide range of ocular conditions, including age-related macular degeneration, diabetic macular edema, diabetic retinopathy, retinal vein occlusion, and several inherited retinal dystrophies4,5.
Neuronal ceroid lipofuscinoses (NCL; Batten disease) are a group of fatal lysosomal storage diseases that cause severe degeneration of the brain and retina. There are currently 13 known variants of NCL resulting from mutations in different genes (CLN1-8, CLN10-14) that predominantly affect children but have varying ages of onset and disease severity6. The NCLs share common progressive symptoms, including cognitive and motor decline, seizures, and loss of vision. There is no cure for NCL; however, brain-directed enzyme-replacement therapy is currently in clinical trials for CLN2 disease7,8, and AAV-mediated gene therapy has shown great promise in preclinical studies, with a clinical trial for CLN5 gene therapy expected to begin in 20229,10.
Many other species develop naturally occurring forms of NCL, including cats, dogs, sheep, and cows. Two ovine models of NCL are currently under active study in New Zealand: a CLN5 disease model in Borderdale sheep and a CLN6 disease model in South Hampshire sheep. Affected sheep exhibit many of the clinical and pathological features of the human disease, including retinal atrophy and loss of vision10,11. Although brain-directed CLN5 gene therapy in sheep with CLN5 disease can prevent or halt brain atrophy and clinical decline, the treated sheep do still lose their vision9. This highlighted the need to treat the retina to preserve vision and maintain a better quality of life, leading to the establishment of a protocol for ocular gene therapy in sheep.
The sheep eye represents a good model of the human eye due to its similarity in eye globe dimensions, vitreous volume, and retinal structure10,12,13. This paper details the surgical protocol for IVT delivery of a small volume (≤100 µL) of therapeutic viral vector to the ovine eye.
Protocol
All experimental protocols were approved by the Lincoln University Animal Ethics committee and are in line with the US National Institutes of Health guidelines for the care and use of animals in research and the New Zealand Animal Welfare Act (1999). Borderdale sheep were diagnosed at birth14 and maintained at Lincoln University research farms. Three 3-month-old homozygous (CLN5-/-) ewes received a single IVT injection to the left eye, with the untreated right eye acting as an internal control. Electroretinography and pathology data were compared to historical healthy and affected control data. The viral vector used in this study was a self-complementary adeno-associated virus serotype 9, containing the chicken beta action (CBh) promoter and codon-optimized ovine CLN5 (scAAV9/CBh-oCLN5opt). The viral vector was provided by the University of North Carolina Vector Core, NC, USA.
1. Presurgery
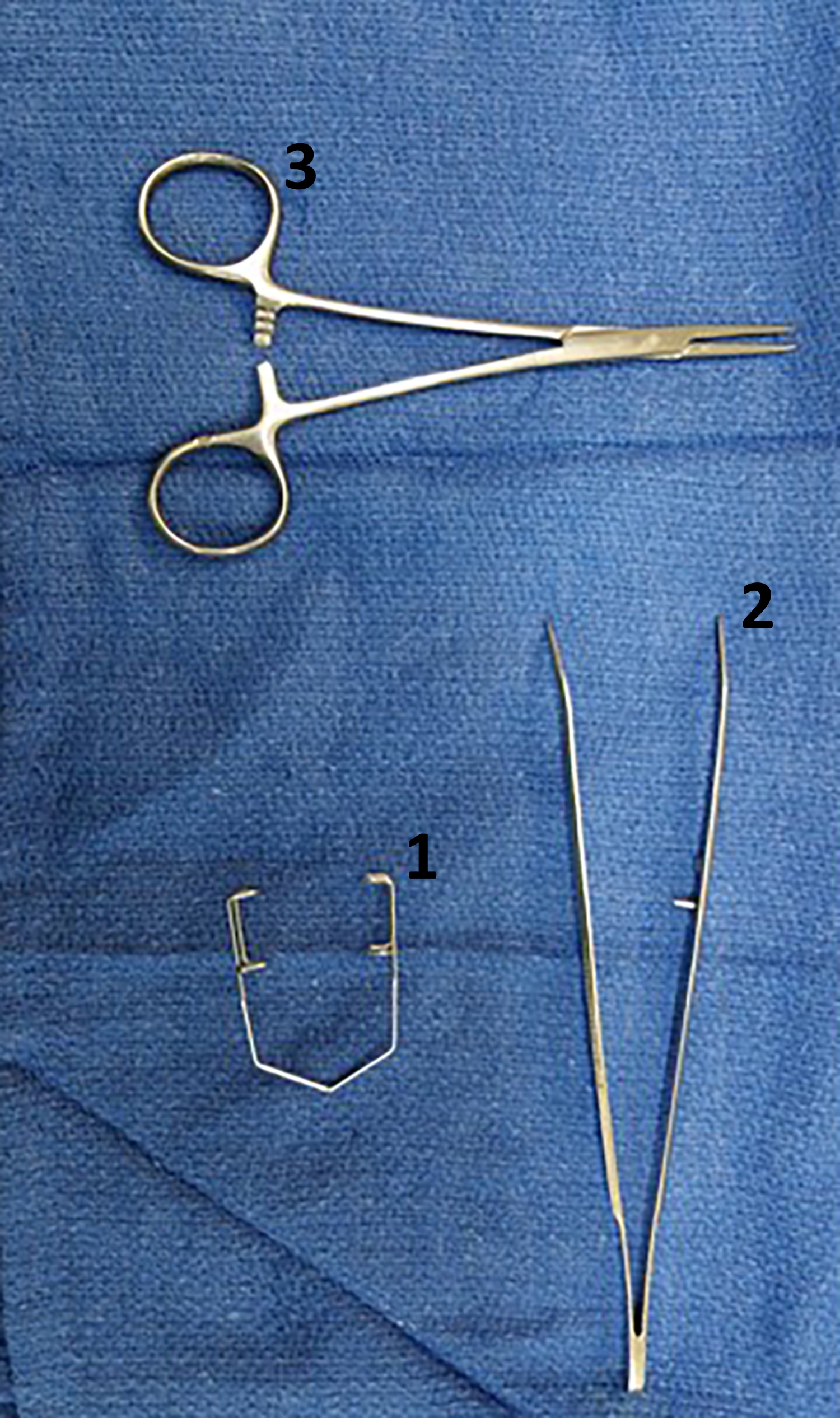
- Autoclave the surgical kit (Figure 1).
- Fast the sheep for 24 h before the surgery.
- Record live weights prior to surgery.

Figure 1: Intravitreal surgery kit. Instruments required for IVT surgery include (1) a speculum to hold the eyelids open and (2) a pair of curved-nose forceps to grasp the bulbar conjunctiva and rotate the eye. (3) A straight nose hemostat is also included as an alternative instrument to grip the bulbar conjunctiva and hold the eye in place if it has rolled back into the eye orbit. This kit is autoclaved prior to surgery. Please click here to view a larger version of this figure.
{kind=link}
2. Surgical procedure
- Restrain the animal and, using electronic clippers, shave the wool from one side of the neck over the jugular vein.
- Occlude the jugular vein by applying pressure at the base of the jugular groove and visualize the raised vein.
- Draw up the appropriate amount of diazepam (0.3 mg/kg) and ketamine (7.5 mg/kg) into a sterile syringe and attach a sterile 20 G needle. Insert the needle into the jugular vein and gently draw back on the plunger to ensure blood enters the hub and the needle is inside the vein. Once confirmed, induce through intravenous (jugular) administration.
- Immediately after induction, place the animal in dorsal recumbency, extend the neck, and hold the tongue up and forward, using a laryngoscope to visualize the larynx. Perform endotracheal intubation by gently inserting an endotracheal tube (size 6.0-9.0 depending on the size of the sheep) between the vocal cords when the animal exhales. Inflate the endotracheal cuff immediately and secure the tube with a tie around the lower jaw. Confirm air flow through the tube.
- Transfer the sheep to the surgical table and place it in lateral recumbency.
- Immediately connect the endotracheal tube to the hoses of the anesthetic machine for delivery of isoflurane in 100% oxygen. Initially commence with 3%-4% isoflurane and then reduce to 2%-3% for maintenance. Observe the spontaneous ventilation of the sheep.
- Monitor heart (pulse) rate, respiratory rate, oxygen saturation, end-tidal CO2 levels, and rectal body temperature throughout the procedure. See Table 1 for physiological values for these parameters in anesthetized sheep (variable, but use as guidance).
- Place a large, sterile, square drape on a surgical operating cart, followed by the sterile instruments.
- Position a sterile, fenestrated surgical drape over the eye to be injected.
- Aseptically disinfect the eye using a sterile 20 mL syringe to irrigate the eye with 1-5% povidone-iodine solution.
- Apply 1-2 drops Alcaine 0.5% W/V ophthalmic solution, as a local anesthetic, to the eye.
- Fit a Nopa Barraquer-Colibri eye speculum (10 mm) to the eyelids to hold the eye open.
- Grasp the bulbar conjunctiva on the dorsolateral aspect of the eye with forceps, and rotate the eye globe ventromedially.
| Conscious | Anesthetized | Recommended critical intervention point | |
| Heart rate (beats/min) | 50-80 (rest) to 280 (active) | 50-80 | <50, >100 |
| Respiratory rate (breaths/min) | 15-40 (rest) to 350 (overheated) | 10-30 | <8, >40 |
| Oxygen saturation (mm Hg) | 95-100 | 98-100 | <90 |
| End-tidal CO2 (mm Hg) | 35-45 | 35-45 | >55 |
| Body temperature (˚C) | 38.5-39.5 | 38.5-39.5 | <36, >40 |
Table 1: Physiological values of parameters to be monitored in anesthetized sheep.
3. Viral preparation
- Store AAV vector aliquots at −80 ˚C until use.
- On the day of surgery, thaw the required number of vials for IVT delivery on ice.
- Immediately prior to administration, vortex the viral vector aliquot and centrifuge at 400 × g for 10 s to collect the contents.
- Dilute each viral vector aliquot in sterile-filtered 1x phosphate-buffered saline (PBS) to the desired dose in a final volume of 100 µL. Prepare vector dilutions in a sterile 1.5 mL low-protein-binding microcentrifuge tube using sterile filter pipette tips. Dispose of all consumables that have been in contact with the viral vector in disinfectant solution (see the Table of Materials).
NOTE: In the original publication15 the dose of the therapeutic agent (AAV9.CLN5) was 1.9 x 1010 viral genomes. The recommended dosage will vary depending on the therapeutic agent being administered; therefore, a dosage has not been included in the standard protocol presented here. - Draw the full 100 µL of the AAV vector preparation into a sterile, low-dead space 1 mL syringe with a permanently attached 28 G x 1/2 in needle for immediate injection. Ensure the length of time from preparation to injection is less than 2 min.
4. Viral administration
- Insert the needle approximately 7 mm posterior to the sclera on the lateral aspect of the eye and angled posteriorly to avoid the lens (Figure 2 and Figure 3). Administer the single injection of 100 µL as a bolus as close to the retina as possible without disturbing the retinal surface.
- Rinse the eye with approximately 10-15 mL of 1-5% povidone-iodine solution followed by 10 mL of saline before removal of the speculum and drape.
- Turn the sheep over and repeat with the other eye if required.

Figure 2: Ventromedial rotation of the eye globe. (A) Grasp the bulbar conjunctiva with nontoothed forceps and (B) rotate ventromedially (i.e., down and towards the snout) to expose the dorsolateral surface of the eye for injection. Abbreviations: V = ventral, D = dorsal, M = medial, L = lateral. Please click here to view a larger version of this figure.
{kind=link}

Figure 3: Injection location and depth. The needle is injected on the dorsolateral aspect of the eye globe, and the full length of the needle shaft (0.5 in/12.7 mm) is inserted into the eye. Note the angle of the needle toward the posterior of the eye to avoid the lens and inject as close to the retina as possible. Please click here to view a larger version of this figure.
{kind=link}
5. Postoperative management
- On completion of the procedure, stop isoflurane gas inhalation anesthesia, flush the line with 100% oxygen, disconnect the hose from the endotracheal tube, and transfer the sheep to the recovery room.
- Place the sheep in sternal recumbency, with legs tucked underneath, and monitor until full recovery. Ensure the animal's mouth is clear of any obstructions.
- When the swallowing reflex is observed, partially deflate the cuff of the endotracheal tube and gently remove the tube from the mouth.
- Administer an intramuscular nonsteroidal anti-inflammatory into the biceps femoris muscle of the hind limb, subcutaneous antibiotics on the side of the neck or behind the shoulder, and 0.5% chloramphenicol eye drops to the surface of the eye globe.
- Provide water and food (lucerne pellets and chaff) once the sheep can stand unassisted.
- Administer 0.5% chloramphenicol eye drops 2-3 per day for 7 days post surgery.
- Keep the sheep indoors overnight before returning to the outdoor paddock approximately 24 h post surgery.
- Record rectal temperatures daily for 3 weeks. Monitor for any changes in pulse or respiratory rate, food consumption, neurobehavior, body temperature, weight, posture, eye health, and clinical signs of ill-health. Seek appropriate veterinary treatment if there are any indications of adverse events.
6. Assessing efficacy in vivo
- If the goal of the IVT injection is to preserve vision, monitor efficacy in vivo by methods such as maze testing or electroretinography (ERG) to assess retinal cell function or optical coherence tomography (OCT) to assess retinal structure.
NOTE: These efficacy measures have been well described following IVT gene therapy11,15,16.
7. Postmortem tissue analysis
- Perform sheep euthanasia by an approved method at an appropriate endpoint following intravitreal injection surgery.
NOTE: Suggested euthanasia methods, such as intravenous veterinary euthanasia drugs or a penetrating captive bolt to the cervical spine followed by rapid exsanguination, are detailed elsewhere15,16. - Harvest sheep eye globes using surgical sharp/blunt curved scissors. Cut the lateral and medial canthus to increase the eye socket opening and then systematically cut through the conjunctival folds, connective tissue, muscles, and optic nerve to free the eye globe from the socket.
- Immersion-fix intact, enucleated eye globes in 10% formalin for 2 h, followed by postfixation in Bouin's solution for 4 h, making a small (0.5 cm) cut in the sclera to allow sufficient perfusion. Alternatively, immersion-fix the eye globes in Davidson's solution for 48 h.
- Process sections of eye tissue via routine paraffin wax embedding and sectioning at 3-5 µm.
NOTE: Staining procedures for hematoxylin and eosin (H&E) staining and immunohistochemical analysis have been described previously15,16. - Assess the efficacy in postmortem tissue by measures such as total retinal thickness, retinal layer thickness, counts of outer nuclear layer cellular rows, and immunohistochemical staining for retinal cell types, retinal glia, or proteins of interest.
NOTE: For protocols for these analyses, see previous publications15,16.
Results
The efficacy of IVT delivery of a CLN5 gene therapy vector in attenuating retinal dysfunction and degeneration in sheep with CLN5 NCL has previously been demonstrated by this research group15. Affected sheep received a single 100 µL IVT injection of CLN5 packaged in an AAV serotype 9 (AAV9) vector (AAV9.CLN5) into one eye, with the contralateral eye serving as an untreated internal control. Vision was assessed monthly from the age at injection (3 months) to end-stage disease (18 months). Post...
Discussion
Intravitreal injections are one of the most common surgical procedures in human ophthalmology and have proven effective in delivering AAV-mediated gene therapies to the retina of sheep. We had previously demonstrated the efficacy of AAV9.CLN5 gene therapy delivered intravitreally in attenuating retinal dysfunction and degeneration in sheep with CLN5 NCL15. It is hoped that the translation of this route of administration to human NCL patients will also prove beneficial.
...
Disclosures
The authors have no conflicts of interest to disclose.
Acknowledgements
The authors would like to acknowledge Dr. Steve Heap (BVSc, CertVOphthal) for his assistance in establishing this protocol and performing the injections described by Murray et al.15. The authors also acknowledge funding from CureKids New Zealand, the Canterbury Medical Research Foundation, Neurogene Inc, and the Batten Disease Support and Research Association.
Materials
| Name | Company | Catalog Number | Comments |
| 1 mL low dead-space safety syringe with permanently attached 0.5 inch needle | Fisher Scientific, Auckland, New Zealand | 05-561-28 | Covidien Monoject Tuberculin Safety syringe or similar |
| 1.5 mL microcentrifuge tube | Sigma Aldrich | HS4323 | Autoclave tubes to sterilise prior to use |
| Anesthesia machine with gas bench and monitor | Hyvet Anesthesia, Christchurch, New Zealand | ||
| Antibiotic eye drops | Teva Pharma Ltd, Auckland, New Zealand | Commercial name: Chlorafast (0.5% chloramphenicol) | |
| BrightMount plus anti-fade mounting medium | Abcam, Cambridge, United Kingdom | ab103748 | |
| DAPI (4′ ,6-diamidino-2-phenylindole dihydrochloride) | Sigma Aldrich, St. Louis, Missouri, United States | 10236276001 | |
| Diazepam sedative | Ilium, Troy Laboratories Pty Ltd, Tauranga, New Zealand | 5 mg/mL | |
| Endotracheal tubes | Flexicare Medical Ltd, Mountain Ash, United Kingdom | Standard, cuffed. Sizes 7, 7.5, or 8 depending on sheep size | |
| Eye speculum | Capes Medical Ltd, Tauranga, New Zealand | KP151/14 | Nopa Barraquer-Colibri (10 mm) |
| Fenestrated surgical drape | Amtech Medical Ltd, Whanganui, New Zealand | DI583 | Or similar |
| Filter Tips | Interlab, Auckland, New Zealand | 10, 200, and 1,000 µL | |
| Formaldehyde solution (37%) | Fisher Scientific, Auckland, New Zealand | AJA809-2.5PL | Make up to 10% in distilled water with 0.9% NaCl |
| Goat anti-rabbit Alexa Fluor 594 | Invitrogen Carlsbad, CA, USA | A-11012 | Use at a dilution of 1:500 |
| Isoflurane anesthetic | Attane, Bayer Animal Health, Auckland, New Zealand | ||
| Ketamine HCl anesthetic/analgesic | PhoenixPharm Distributors Ltd, Auckland, New Zealand | 100 mg/mL | |
| Laryngoscope (veterinary) | KaWe Medical, Denmark | Miller C blade, size 2 | |
| Needles | Capes Medical Ltd, Tauranga, New Zealand | 302025 | BD Hypodermic Needles, or similar |
| Non-steroidal anti-inflammatory | Boehringer Ingelheim (NZ) Ltd, Auckland, New Zealand | 49402/008 | Commercial name: Metacam 20 (20 mg/mL meloxicam) |
| Non-toothed forceps | Capes Medical Ltd, Tauranga, New Zealand | AB864/16 | Or similar |
| Non-toothed hemostat | Capes Medical Ltd, Tauranga, New Zealand | AA150/12 | Or similar |
| Normal goat serum | Thermo Fisher Scientific, Christchurch, New Zealand | 16210072 | |
| Oxygen (medical) | BOC Gas, Christchurch, New Zealand | D2 cylinder, gas code 180 | |
| Phosphate buffered saline | Thermo Fisher Scientific, Christchurch, New Zealand | 10010023 | Sterile, filtered |
| Povidone-Iodine solution | Capes Medical Ltd, Tauranga, New Zealand | 005835 | Commercial name: Betadine (10% povidone-iodine) |
| Rabbit anti-cow glial fibrillary acidic protein (GFAP) | Dako, Glostrup, Denmark | Z0334 | Use at a dilution of 1:2,500 |
| Self-complementary adeno-associated virus serotype 9, containing the chicken beta action (CBh) promoter and codon-optimized ovine CLN5 | University of North Carolina Vector Core, NC, USA. | scAAV9/CBh-oCLN5opt | |
| Sodium Chloride 0.9% IV Solution | Capes Medical Ltd, Tauranga, New Zealand | AHB1322 | Commercial name: Saline solution |
| Subcutaneous antibiotics | Intervet Schering Plough Animal Health Ltd, Wellington, New Zealand | Commercial name: Duplocillin LA (150,000 IU/mL procaine penicillin and 115,000 IU/mL benzathine penicillin) | |
| Surgical sharp blunt curved scissors | Capes Medical Ltd, Tauranga, New Zealand | SSSHBLC130 | |
| Terumo Syringe Luer Lock | Amtech Medical Ltd, Whanganui, New Zealand | SH159/SH160 | Sterile syringes; 10 mL for drawing up induction drugs, 20 mL for drawing up saline |
| Virkon Disinfectant Powder | EBOS Group Ltd, Christchurch, NZ | 28461115 |
References
- Himawan, E., et al. Drug delivery to retinal photoreceptors. Drug Discovery Today. 24 (8), 1637-1643 (2019).
- Murray, S. J., Mitchell, N. L. Ocular therapies for neuronal ceroid lipofuscinoses: More than meets the eye. Neural Regeneration Research. 17 (8), 1755-1756 (2022).
- Bishop, P. N. Structural macromolecules and supramolecular organisation of the vitreous gel. Progress in Retinal and Eye Research. 19 (3), 323-344 (2000).
- Grzybowski, A., et al. update on intravitreal injections: Euretina expert consensus recommendations. Ophthalmologica. 239 (4), 181-193 (2018).
- Pavlou, M., et al. Novel AAV capsids for intravitreal gene therapy of photoreceptor disorders. EMBO Molecular Medicine. 13 (4), 13392 (2021).
- Kousi, M., Lehesjoki, A. -. E., Mole, S. E. Update of the mutation spectrum and clinical correlations of over 360 mutations in eight genes that underlie the neuronal ceroid lipofuscinoses. Human Mutation. 33 (1), 42-63 (2012).
- Wibbeler, E., et al. Cerliponase alfa for the treatment of atypical phenotypes of CLN2 disease: A retrospective case series. Journal of Child Neurology. 36 (6), 468-474 (2021).
- Schulz, A., et al. Study of intraventricular cerliponase alfa for CLN2 disease. The New England Journal of Medicine. 378 (20), 1898-1907 (2018).
- Mitchell, N. L., et al. Longitudinal in vivo monitoring of the CNS demonstrates the efficacy of gene therapy in a sheep model of CLN5 Batten disease. Molecular Therapy. 26 (10), 2366-2378 (2018).
- Murray, S. J., Mitchell, N. L. Natural history of retinal degeneration in ovine models of CLN5 and CLN6 neuronal ceroid lipofuscinoses. Scientific Reports. 12 (1), 3670 (2022).
- Russell, K. N., Mitchell, N. L., Wellby, M. P., Barrell, G. K., Palmer, D. N. Electroretinography data from ovine models of CLN5 and CLN6 neuronal ceroid lipofuscinoses. Data in Brief. 37, 107188 (2021).
- Shafiee, A., McIntire, G. L., Sidebotham, L. C., Ward, K. W. Experimental determination and allometric prediction of vitreous volume, and retina and lens weights in Göttingen minipigs. Veterinary Ophthalmology. 11 (3), 193-196 (2008).
- Shinozaki, A., Hosaka, Y., Imagawa, T., Uehara, M. Topography of ganglion cells and photoreceptors in the sheep retina. The Journal of Comparative Neurology. 518 (12), 2305-2315 (2010).
- Frugier, T., et al. A new large animal model of CLN5 neuronal ceroid lipofuscinosis in Borderdale sheep is caused by a nucleotide substitution at a consensus splice site (c.571+1G>A) leading to excision of exon 3. Neurobiology of Disease. 29 (2), 306-315 (2008).
- Murray, S. J., et al. Intravitreal gene therapy protects against retinal dysfunction and degeneration in sheep with CLN5 Batten disease. Experimental Eye Research. 207, 108600 (2021).
- Ross, M., et al. Outer retinal transduction by AAV2-7m8 following intravitreal injection in a sheep model of CNGA3 achromatopsia. Gene Therapy. , (2021).
- Boyd, R. F., et al. Photoreceptor-targeted gene delivery using intravitreally administered AAV vectors in dogs. Gene Therapy. 23 (2), 223-230 (2016).
- Dalkara, D., et al. In vivo-directed evolution of a new adeno-associated virus for therapeutic outer retinal gene delivery from the vitreous. Science Translational Medicine. 5 (189), (2013).
- Gearhart, P. M., Gearhart, C., Thompson, D. A., Petersen-Jones, S. M. Improvement of visual performance with intravitreal administration of 9-cis-retinal in Rpe65-mutant dogs. Archives of Ophthalmology. 128 (11), 1442-1448 (2010).
- Ross, M., et al. Evaluation of photoreceptor transduction efficacy of capsid-modified adeno-associated viral vectors following intravitreal and subretinal delivery in sheep. Human Gene Therapy. 31 (13-14), 719-729 (2020).
- Kotterman, M. A., et al. Antibody neutralization poses a barrier to intravitreal adeno-associated viral vector gene delivery to non-human primates. Gene Therapy. 22 (2), 116-126 (2015).
- Whitehead, M., Osborne, A., Yu-Wai-Man, P., Martin, K. Humoral immune responses to AAV gene therapy in the ocular compartment. Biological Reviews. 96 (4), 1616-1644 (2021).
- Yun, C., Oh, J., Hwang, S. -. Y., Kim, S. -. W., Huh, K. Subconjunctival hemorrhage after intravitreal injection of anti-vascular endothelial growth factor. Graefe's Archive for Clinical and Experimental Ophthalmology. 253 (9), 1465-1470 (2015).
- Christensen, L., Cerda, A., Olson, J. L. Real-time measurement of needle forces and acute pressure changes during intravitreal injections. Clinical & Experimental Ophthalmology. 45 (8), 820-827 (2017).
- Allmendinger, A., Butt, Y. L., Mueller, C. Intraocular pressure and injection forces during intravitreal injection into enucleated porcine eyes. European Journal of Pharmaceutics and Biopharmaceutics. 166, 87-93 (2021).
- Ross, M., Ofri, R. The future of retinal gene therapy: Evolving from subretinal to intravitreal vector delivery. Neural Regeneration Research. 16 (9), 1751-1759 (2021).
- Henein, C., et al. Hydrodynamics of intravitreal injections into liquid vitreous substitutes. Pharmaceutics. 11 (8), 371 (2019).
- Park, I., Park, H. S., Kim, H. K., Chung, W. K., Kim, K. Real-time measurement of intraocular pressure variation during automatic intravitreal injections: An ex-vivo experimental study using porcine eyes. PloS One. 16 (8), 0256344 (2021).
- Willekens, K., et al. Intravitreally injected fluid dispersion: Importance of injection technique. Investigative Ophthalmology & Visual Science. 58 (3), 1434-1441 (2017).
- Peynshaert, K., Devoldere, J., De Smedt, S. C., Remaut, K. In vitro and ex vivo models to study drug delivery barriers in the posterior segment of the eye. Advanced Drug Delivery Reviews. 126, 44-57 (2018).
- Kiss, S. Vector Considerations for Ocular Gene Therapy. Adeno-associated virus vectors offer a safe and effective tool for gene delivery. Retinal Physician. 17, 40-45 (2020).
- Kleine Holthaus, S. -. M., et al. Gene therapy targeting the inner retina rescues the retinal phenotype in a mouse model of CLN3 Batten disease. Human Gene Therapy. 31 (13-14), 709-718 (2020).
- Kleine Holthaus, S. -. M., et al. Neonatal brain-directed gene therapy rescues a mouse model of neurodegenerative CLN6 Batten disease. Human Molecular Genetics. 28 (23), 3867-3879 (2019).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved