Method Article
Controlled Reversible Visceral Arterial Ischemia, Venous Congestion and Combined Malperfusion via Midline Laparotomy in Rats
In This Article
Summary
This article introduces a standardized procedure for controlled, reversible malperfusion of visceral organs in rat models. The aim is to induce these malperfusion states with a high degree of methodological certainty and control while maintaining technical simplicity and error resilience.
Abstract
Besides sepsis and malignancy, malperfusion is the third leading cause of tissue degradation and a major pathomechanism for various medical and surgical conditions. Despite significant developments such as bypass surgery, endovascular procedures, extracorporeal membrane oxygenation, and artificial blood substitutes, tissue malperfusion, especially of visceral organs, remains a pressing issue in patient care. The demand for further research on biomedical processes and possible interventions is high. Valid biological models are of utmost importance in enabling this kind of research. Due to the multifactorial aspects of tissue perfusion research, which include not only cell biology but also vascular microanatomy and rheology, an appropriate model requires a degree of biological complexity that only an animal model can provide, rendering rodents the obvious model of choice. Tissue malperfusion can be differentiated into three distinct conditions: (1) isolated arterial ischemia, (2) isolated venous congestion, and (3) combined malperfusion. This article presents a detailed step-by-step protocol for the controlled and reversible induction of these three types of visceral malperfusion via midline laparotomy and clamping of the abdominal aorta and caval vein in rats, underscoring the significance of precise surgical methodology to guarantee uniform and dependable results. Prime examples of possible applications of this model include the development and validation of innovative intraoperative imaging modalities, such as Hyperspectral Imaging (HSI), to objectively visualize and differentiate malperfusion of gastrointestinal, gynecological, and urological organs.
Introduction
While the implications of tissue perfusion deprivation in the form of local or systemic tissue malperfusion conditions have long been recognized, they persist as one of the primary causes of morbidity and mortality in both the United States and Europe1. These malperfusion conditions are the third leading cause of tissue degradation, following malignancy and septic inflammation, but have a far wider spectrum of origins compared to the latter two2.
This spectrum ranges from local mechanisms such as atrial fibrillation with thromboembolic occlusion, vasoconstriction, and iatrogenic or traumatic dissection, to systemic mechanisms such as cardiac insufficiency or shock, sepsis, hypovolemia, and steal phenomena. These diverse mechanisms underlie a variety of medical and surgical conditions. The significant morbidity and mortality associated with these conditions have directed medical attention toward procedures for reinstating blood flow to malperfused tissues in order to forestall necrosis and restore organ function over the decades3.
This research effort has resulted in a variety of pharmaceutical, medical, and surgical solutions to restore physiological organ perfusion, including advances in bypass surgery4, endovascular procedures5, extracorporeal membrane oxygenation6,7, organ machine perfusion during transplantation8, and artificial blood substitutes9.
Yet, despite these significant developments, malperfusion, especially of visceral organs, remains a pressing issue in patient care, and the demand for further research on biomedical processes and rescue strategies is high. Valid biological models are of utmost importance in enabling this kind of research. Due to the multifactorial aspects of tissue perfusion research, which include not only cell biology but also vascular microanatomy and rheology, an appropriate model requires a degree of biological complexity that only a complete model organism can provide, making rodents the obvious model of choice.
Tissue malperfusion can be differentiated into three distinct conditions: isolated arterial ischemia, isolated venous congestion, and combined malperfusion10. Clinically relevant scenarios for these conditions include (1) Arterial ischemia: Atrial fibrillation with thromboembolic occlusion, septic emboli, vasoconstriction, iatrogenic or traumatic vascular dissection or clamping, cardiac insufficiency or shock, aortic dissection, sepsis and hypovolemia, extreme arterial obstruction due to external constriction, pulmonary artery embolism, chronic arterial vascular occlusive diseases, or steal phenomena; (2) Venous congestion: Iatrogenic or traumatic vascular dissection or clamping, heart failure, liver fibrosis or cirrhosis, venous obstruction due to external constriction, venous thrombosis, venous insufficiency, and Budd-Chiari syndrome; (3) Combined malperfusion: Combinations of the above conditions and advanced stages of the aforementioned conditions, such as secondary venous congestion due to ischemia-induced fibrosis or secondary arterial ischemia due to congestion-induced retention, as well as specific organ conditions like ischemic inflammation (e.g., ischemic colitis)11,12.
This article, therefore, aims to provide a step-by-step model to induce controlled, reversible visceral arterial ischemia, venous congestion, and combined malperfusion via midline laparotomy in rats for both survival and non-survival applications, as depicted in Figure 1. The experimental model offers a controlled environment for studying the multifaceted dynamics of arterial ischemia, venous congestion, and their combined sequelae, emulating clinically relevant scenarios encountered in various conditions.

Figure 1: Overview of the protocol. Schematic depiction of vascular rat anatomy and depiction of the clamping site (gray arrow). (A) Physiological perfusion. (B) Arterial ischemia. (C) venous congestion. (D) Combined malperfusion. Please click here to view a larger version of this figure.
{kind=link}
Protocol
All animal activities described here were conducted in accredited facilities and approved by the Institutional Animal Care and Use Committee (IACUC) of the Baden-Württemberg Regional Council in Karlsruhe, Germany (35-9185.81/G-62/23). Experimental animals were managed according to institutional standards, German laws for animal use and care, the directives of the European Community Council (2010/63/EU), and the ARRIVE guidelines. Male Sprague Dawley rats with an order weight of 400 grams were used after being acclimatized for one week. The details of the reagents and the equipment used in this study are listed in the Table of Materials.
1. Anesthesia and analgesia
- Anesthetize the rat with the medication following the institutional protocols. Isoflurane is recommended for induction of sedation followed by an i.p. injection of 100 mg/kg body weight ketamine and 4 mg/kg body weight xylazine. Additional analgesia can be achieved with a s.c. injection of 5 mg/kg body weight carprofen. For details, please refer to Studier-Fischer et al.13.
- Apply ophthalmic ointment to the eyes to prevent dryness.
- Guarantee proper analgetic depth using the toe pinch test with surgical forceps.
- Regularly reassess and adjust the depth of anesthesia during surgery.
2. Procedure preparation
- Prepare the scrub table with all the required materials and instruments, including releasable microvascular clamps and the applicator (Figure 2A-C), blunt overholt clamp, fine preparation scissor, and forceps.
- Prepare the surgical preparation hooks by folding cannulas at an angle of 135° at 1 cm to the tip and connect them to plastic perfusion tubes via Luer-lock ready to apply tension using a surgical mosquito clamp (Figure 2D,E).
- Prepare a rodent surgical exposure apparatus, including Y-shaped fixation rods and a heating pad, as specified in Studier-Fischer et al.13.
- Ensure proper oxygenation is achieved via the inhalation of 100% oxygen using a neonatal face mask (Figure 2F).

Figure 2: Experimental and animal setup. (A) Surgical instruments and materials required. (B,C) Releasable microvascular clamp and applicator. (D,E) A folded cannula connected to a perfusion tube is used as a surgical preparation hook. (F,G) Rat model oxygenated with a face mask and shaven. (H) Cutaneous incision over complete abdominal length. (I-M) resection of the xiphoid and hemostasis. (N-Q) Hepatic mobilization and dissection of the falciform ligament (arrow 1). (R) Application of preparation hooks and metal stands for exposure of organs after laparotomy. (S) Full visceral exposure of abdominal major vessels using blunt hooks (arrow 2), silicone vessel loops (arrow 3), and surgical compress (arrow 4). (T,U) Abdominal aorta and caval vein. (V) Atraumatic preparation instruments. (W) Humidified cotton swap (arrow 5). (X) Humidified compress in forceps (arrow 6) and blunt overholt clamps (arrow 7). Please click here to view a larger version of this figure.
{kind=link}
3. Surgical preparation
- Shave the surgical access site for a midline laparotomy (Figure 2G). Perform a cutaneous incision over the desired abdominal length, i.e., about 7 cm (Figure 2H), advance with the laparotomy by dissecting the fascia, and stitch the surgical preparation hooks with attached plastic tubes and surgical mosquito clamps through the skin. Expose the surgical situs using the surgical preparation hooks, applying tension to the tissue.
- Ensure that the peritoneum is dissected cranially only until a few millimeters below the beginning of the sternum, leaving some of the peritoneum intact. Place a part of a surgical compress below the sternum (Figure 2I) and resect the xiphoid with strong material scissors. Apply pressure to the resection area using the surgical compress to achieve sufficient hemostasis of this well-perfused region (Figure 2I-M).
- Mobilize the liver dorso-caudally to expose the falciform ligament (Figure 2N) and dissect the ligament (Figure 2O-Q).
- For hemostatic control, depending on where the clamping of the major vessels should be performed, perform a full visceral exposure of abdominal major vessels (Figure 2R) and the vessels slung with silicone vessel loops (Figure 2S-U). Only atraumatic preparation instruments should be used (Figure 2V), such as humidified cotton swaps (Figure 2W), humidified compress in forceps, and blunt overholt clamps (Figure 2X).
4. Preparation and clamping of abdominal aorta for arterial ischemia
- Perform a left medialization of the upper abdominal organs using atraumatic preparation instruments to gain access to the left adrenal artery (Figure 3A-D).
- Identify the pulsating site typically medial to the cranial extension of the left adrenal artery, indicating the course of the aorta (Figure 3E). Advance through the soft tissue using overholt clamps for blunt dissection in order to access the abdominal aorta (Figure 3F,G).
- Tunnel the abdominal aorta at the most cranial end using blunt overholt clamps (Figure 3H-L) and sling the aorta using a silicone vessel loop (Figure 3M-T).
- Apply a suitable aneurysm microvascular clamp using the silicone loop to slightly luxate the aorta ventrally and guide the aneurysm microvascular clamp along the silicone loop to guarantee isolated aortic clamping (Figure 3U). Depending on the research question, the microvascular clamp can be released again.

Figure 3: Preparation and clamping of the abdominal aorta. (A) Exposure of visceral organs. (B-E) Left medialization of upper abdominal organs using atraumatic preparation instruments to gain access to the left adrenal artery. (F,G) Blunt dissection medial of the left adrenal artery at the pulsating site (gray arrow) in order to access the abdominal aorta. (H-L) Tunneling of the abdominal aorta using blunt overholt clamps. (M-T) Slinging the aorta using a silicone vessel loop. (U) Application of a releasable aneurysm microvascular clamp using the silicone loop as guidance. (V-Z) Visualization of the celiac artery (orange) in reference to the aorta (red) and the silicone vessel loop. Please click here to view a larger version of this figure.
{kind=link}
5. Preparation and clamping of suprahepatic abdominal caval vein for venous congestion
- Mobilize the liver to the right using atraumatic preparation instruments, sharply dissect the hepatic ligaments, and further lateralize the liver (Figure 4A-C).
- Open the retrohepatic space at the left crus of the diaphragm using blunt overholt clamps (Figure 4D-G).
- Tunnel the caval vein using blunt overholt clamps (Figure 4H-K) and sling the caval vein using silicone vessel loops (Figure 4L-O).
- Apply a suitable aneurysm microvascular clamp using the silicone loop to slightly luxate the caval vein ventrally and guide the aneurysm microvascular clamp along the silicone loop to guarantee isolated clamping of the caval vein (Figure 4R).

Figure 4: Preparation and clamping of suprahepatic abdominal caval vein. (A) Exposure of cranial visceral organs. (B) Tissue-protective mobilization of the liver and sharp dissection of hepatic ligaments using atraumatic preparation instruments. (C) Lateralization of the liver. (D-G) The opening of the retrohepatic space and preparation at the left crus of the diaphragm. (H-K) Tunneling of the caval vein (blue) using blunt overholt clamps. (L-O) Slinging the caval vein using silicone vessel loops. (P,Q) Exertion of tension to tentatively restrict caval blood flow. (R) Application of a releasable aneurysm microvascular clamp using the silicone loop as guidance. Please click here to view a larger version of this figure.
{kind=link}
6. Clamping of the abdominal aorta and suprahepatic abdominal caval vein for combined malperfusion
- Perform the steps above until both the aorta and caval vein are slung with silicone vessel loops. Advance with the application of the aneurysm microvascular clamp for both vessels again using the silicone loop for guidance. Clamping the aorta first and minimizing the time required until subsequent caval clamping to only a few seconds is recommended.
NOTE: Depending on the desired scenario and research purpose, malperfusion can be continued over or released after a defined timespan, and animals can either be euthanized by sharp cardiectomy (following institutionally approved protocols) for non-survival applications, or receive stepwise abdominal closure using surgical sutures in case of planned follow-ups and survival experiments. For the present study, the animals were euthanized.
Results
This protocol was performed in 10 male rats (mean weight 403 g ± 26 g) in a non-survival setting. The success rate was defined by survival over 20 min after arterial clamping, venous clamping, and combined clamping for 5 min with 10 min of reperfusion, each of which was 100%. The mean duration of the preparation from skin incision until both vessels were slung with silicone loops was 11 min 45 s ± 3 min 23 s.
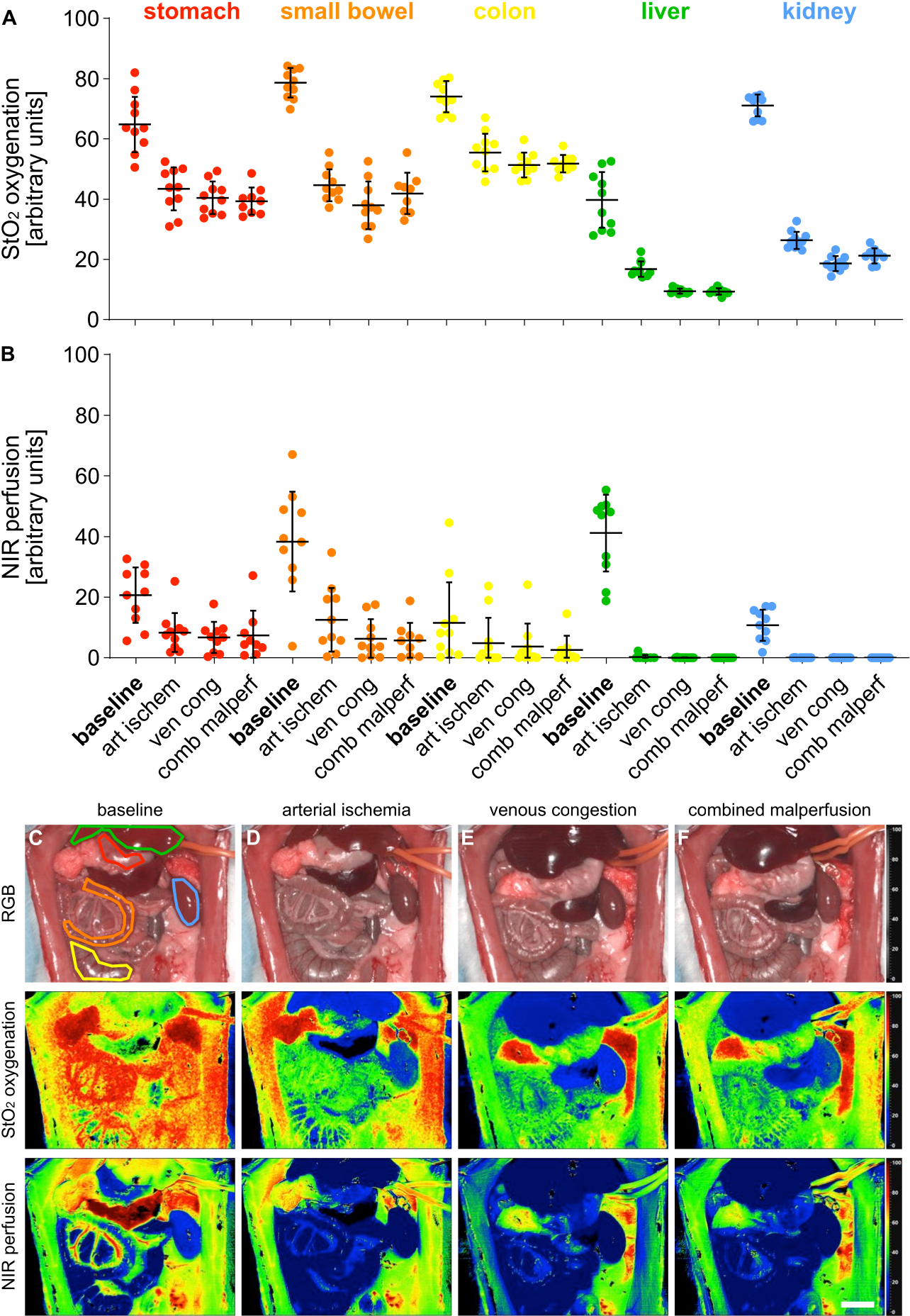
For validation of the 4 different malperfusion states, index parameters for oxygenation (StO2) and perfusion (NIR) were measured using hyperspectral imaging (HSI) across 5 visceral organs (Figure 5).

Figure 5: Validation of the malperfusion model. (A,B) Quantification of HSI oxygenation and perfusion values across four different perfusion states and five different visceral organs with n = 10 animals. (C-F) RGB and color-coded index pictures of HSI recordings containing visceral organs across 4 different perfusion states. Error bars indicate standard deviation. The scale bar depicts 5 cm. Please click here to view a larger version of this figure.
{kind=link}
Values were provided in arbitrary units and showed a significant decrease in the malperfusion states compared to the physiological organ state (Table 1). The hyperspectral results were in line with recent publications indicating that viability and perfusion of tissue can be evaluated using organ-specific HSI StO2 cut-off values that matched the values seen in this study14,15. Exemplarily for the stomach, these were 64.1% (±9.4%) for physiological perfusion,43.1% (±7.4%) for arterial ischemia, 40.5% (±5.4%) for venous congestion and 39.3% (±4.5%) for combined malperfusion.
Since these were non-survival experiments, there is no experimental data on the long-term outcomes of the animals. However, other studies report 100% and 57% survival over 24 h for rats that underwent 30 min and 60 min of superior mesenteric artery clamping16,17 and successfully correlate it with serum levels of Heat Shock Protein 70. Consequently, this might be a possible method to assess outcomes in future survival studies according to different clamping times.
| parameter | organ | baseline | arterial ischemia | venous congestion | combined malperfusion |
| StO2 | stomach | 64.1% (±9.4%) | 43.1% (±7.4%) | 40.5% (±5.4%) | 39.3% (±4.5%) |
| small bowel | 78.4% (±5.1%) | 44.8% (±5.5%) | 38.0% (±7.9%) | 41.9% (±6.9%) | |
| colon | 74.6% (±5.0%) | 56.0% (±6.3%) | 51.3% (±4.1%) | 51.8% (±2.9%) | |
| liver | 39.5% (±9.7%) | 16.9% (±2.6%) | 9.5% (±0.8%) | 9.3% (±1.1%) | |
| kidney | 71.0% (±3.8%) | 26.3% (±3.0%) | 18.6% (±2.5%) | 21.2% (±2.6%) | |
| NIR | stomach | 20.0% (±9.3%) | 8.3% (±6.7%) | 6.8% (±5.1%) | 7.5% (±8.1%) |
| small bowel | 38.6% (±17.4%) | 12.9% (±11.0%) | 6.3% (±6.5%) | 5.7% (±5.9%) | |
| colon | 12.6% (±13.7%) | 5.3% (±8.7%) | 3.8% (±7.5%) | 2.6% (±4.7%) | |
| liver | 40.4% (±13.1%) | 0.3% (±0.7%) | 0.0% (±0.1%) | 0.0% (±0.0%) | |
| kidney | 10.4% (±5.2%) | 0.0% (±0.0%) | 0.0% (±0.1%) | 0.0% (±0.0%) |
Table 1: Tissue parameters. HIS StO2 oxygenation and NIR perfusion values in arbitrary units across 5 visceral organs and 4 different perfusion states.
Discussion
While peripheral arterial occlusive disease (PAOD) alone, as the most prominent representative of tissue malperfusion conditions, already has a prevalence of around 7%, affecting an estimated 8.5 million adults in the United States alone18, tissue malperfusion in general is a relevant pathomechanism in a majority of surgical and medical conditions. Consequently, appropriate and reproducible animal models are absolutely necessary to address novel research questions in this field.
The three vascular dynamic situations that require distinctive investigation are arterial ischemia, venous congestion, and combined malperfusion. By inducing isolated arterial ischemia, scientists can precisely delineate the temporal and spatial progression of tissue hypoxia, investigating the molecular cascades implicated in ischemia-reperfusion injury, cellular apoptosis, and inflammatory responses. By compromising venous drainage, an oftentimes overlooked facet of vascular pathology, scientists can investigate the interplay between arterial inflow and venous outflow discrepancies, shedding light on the pathophysiology of venous thrombosis, congestion-related tissue edema, and microcirculatory dysfunction. When combining both of these pathological situations, one can investigate the dys-synergistic milieu of combined malperfusion, mirroring the complex pathophysiology encountered in clinical syndromes like acute mesenteric ischemia and ischemic colitis.
Beyond elucidating fundamental pathophysiological mechanisms, the ability to induce visceral arterial ischemia, venous congestion, and combined malperfusion in rats serves as an indispensable platform for evaluating the efficacy of pharmacological interventions, surgical techniques, new therapeutic strategies, and innovative imaging modalities, especially such as HSI14,19,20,21,22. This model is, therefore, a key component in providing the required biological tissue ground truth needed to harness the full potential of HSI in tissue evaluation and identification of perfusion states. By leveraging this experimental setup, researchers can expedite the translation of preclinical findings into clinically viable strategies, ultimately reducing the morbidity and mortality associated with diverse vascular and perfusion disorders.
Illustratively, researchers can employ this model to investigate the efficacy of pharmacological agents targeting ischemia-reperfusion injury pathways, such as antioxidants, anti-inflammatory agents, and vasodilators, thereby delineating their potential utility in clinical practice23,24. Additionally, this model facilitates the assessment of novel surgical approaches, such as mesenteric revascularization techniques and venous decompressive procedures, providing invaluable insights into their feasibility, safety, and long-term efficacy25,26.
Furthermore, this experimental framework enables researchers to explore the intricate interplay between vascular dysfunction and systemic comorbidities, such as diabetes, hypertension, and atherosclerosis, thereby illustrating the intricate web of interconnected pathophysiological pathways orchestrating vascular disease progression27,28.
While there are several publications on selective malperfusion of single organs, such as the liver29,30,31or kidney, in rats32,33, there is a lack of scientific literature addressing malperfusion of the complete viscera in rats, and there is explicitly no methodical protocol. This is, therefore, the claim of this manuscript. Limitations of the presented technique mainly include the invasiveness of the procedure and, depending on the duration of malperfusion, consecutive organ thrombosis, and dysfunction, possibly leading to postoperative suffering through multiorgan failure or abdominal compartment syndrome34,35,36. Careful planning and design, depending on the research question, can help balance the required duration of malperfusion and its pathophysiological consequences.
When troubleshooting common challenges encountered during the procedure, attention should be drawn to the following points and recommendations: (1) Ensure thorough preparation of equipment and medication beforehand to minimize interruptions during the procedure; (2) Perform hemostatic control meticulously by carefully preparing and dissecting avascular planes. Consider using bipolar hemostatic forceps for electric hemostasis, if available; (3) Minimize trauma to tissues by using non-traumatic instruments such as humidified cotton swabs or humidified surgical compress with forceps when making contact with the liver parenchyma; (4) Approximately 20% of animals experienced diffuse superficial liver parenchyma bleeding due to delicate tissue conditions. However, the bleeding stopped in all cases with light compression and patience. These recommendations aim to enhance procedural efficiency and minimize complications during the induction of malperfusion in rat models.
When resecting the xiphoid for improved access to the caval vein, ensure that the peritoneum dorsal to the transition between the xiphoid and sternum is left intact over a few millimeters. The resection site of the xiphoid will be hard and sharp, potentially causing trauma to the superficial liver parenchyma. Therefore, it is recommended that the retrosternal peritoneum caudally be mobilized using forceps and wrapped around the bone stump effectively, covering it and supporting hemostasis. The surgical preparation hooks should be stitched through the cranial ventral abdominal wall with cranial tension so that the peritoneal coverage of the xiphoid stump will remain in place.
When dissecting the falciform ligament, care should be taken to avoid accidentally causing iatrogenic injury to the hepatic vein, as this could be fatal to the animal. Due to the high risk of bleeding during vascular preparation, it is recommended that the majority of surgical preparation be done by spreading with blunt overholt clamps, rather than using sharp dissection instruments. Additionally, silicone vessel loops should be moistened prior to usage to reduce surface friction and minimize the risk of tissue trauma.
When applying the aneurysm microvascular clamp, it is crucial to visualize the exact vascular anatomy. For instance, the celiac artery originates very cranially from the abdominal aorta. If celiac occlusion is desired, such as to investigate hepatic malperfusion, the celiac artery should be visualized in reference to the aorta and the silicone vessel loop. This ensures that the celiac artery is included in the clamped vascular tissue (Figure 2V-Z). There was one case in which the clamp was initially placed caudal to the celiac artery by accident. However, this was promptly recognized due to the missing drop in StO2 liver values, and proper reclamping was successfully performed.
The most hazardous preparation step is tunneling the caval vein. This step requires gentle movements and patience, and overholt clamps should only be spread when certain there is no contact with the caval vein. It can be challenging to judge this, as the caval vein will appear as thin avascular connective tissue when slight compression is applied, causing the contained blood to disappear in both directions. There is also a risk of accidental pleural opening and creating a pneumothorax when tunneling the caval vein too cranially. This can be a serious and life-threatening complication, especially since the animal is spontaneously breathing, and no invasive respiratory measures can be taken. It has been found helpful to slightly retract the preparation instruments and continue more caudally to avoid this complication. In cases of hemodynamically relevant and visible pneumothorax with bulging of the hepatic diaphragm, a trans-diaphragmatic one-time puncture and aspiration of the trapped air using a 30 G needle and a small syringe can be recommended as a rescue strategy. This technique was successfully employed in one animal to save it intraoperatively.
Finally, special care should be taken when applying the microvascular clamps to avoid including surrounding connective tissue, which could lead to insufficient occlusion of the desired vessel.
While this protocol is intended as a step-by-step guide for global visceral malperfusion, the clamping site can be adjusted according to the specific research question due to the extensive vascular preparation and mobilization depicted in Figure 1T-V. Therefore, selected malperfusion of organ groups or single organs is also an option when choosing the clamping site further distally along the vascular tree, such as selectively clamping the celiac trunk for hepatic ischemia. By offering a detailed and reproducible methodology, this protocol facilitates a standardized approach for controlled reversible arterial ischemia, venous congestion, and combined malperfusion in rat models, leading to improved data reliability, robustness, researcher independence, and comparability across future animal studies. Consequently, it represents an indispensable tool within the biomedical research armamentarium, offering insights into the complex interplay between vascular compromise, tissue injury, and therapeutic interventions. By harnessing the versatility of this experimental setup, researchers can investigate the mysteries around vascular pathophysiology, forging new frontiers in translational medicine, and ultimately enhancing patient outcomes in the realm of vascular health.
Disclosures
None.
Acknowledgements
The authors gratefully acknowledge the data storage service SDS@hd supported by the Ministry of Science, Research and the Arts Baden-Württemberg (MWK) and the German Research Foundation (DFG) through grant INST 35/1314-1 FUGG and INST 35/1503-1 FUGG. Furthermore, the authors gratefully acknowledge the support from the NCT (National Center for Tumor Diseases in Heidelberg, Germany) through its structured postdoc program and the Surgical Oncology program. We also acknowledge the support through state funds approved by the State Parliament of Baden-Württemberg for the Innovation Campus Health + Life Science Alliance Heidelberg Mannheim from the structured postdoc program for Alexander Studier-Fischer: Artificial Intelligence in Health (AIH) - A collaboration of DKFZ, EMBL, Heidelberg University, Heidelberg University Hospital, University Hospital Mannheim, Central Institute of Mental Health, and the Max Planck Institute for Medical Research. Furthermore, we acknowledge the support through the DKFZ Hector Cancer Institute at the University Medical Center Mannheim. For the publication fee, we acknowledge financial support from Deutsche Forschungsgemeinschaft within the funding program "Open Access Publikationskosten" as well as from Heidelberg University.
Materials
| Name | Company | Catalog Number | Comments |
| Atraumatic preparation forceps | Aesculap | FB395R | DE BAKEY ATRAUMATA atraumatic forceps, straight |
| Blunt overholt clamp | Aesculap | BJ012R | BABY-MIXTER preparation and ligature clamp, bent, 180 mm |
| Cannula | BD (Beckton, Dickinson) | 301300 | BD Microlance 3 cannula 20 G |
| Fixation rods | legefirm | 500343896 | tuning forks used as y-shaped metal fixation rods |
| Heating pad | Royal Gardineer | IP67 | Royal Gardineer Heating Pad Size S, 20 Watt |
| Plastic perfusor tube | M. Schilling GmbH | S702NC150 | connecting tube COEX 150 cm |
| Preparation scissors | Aesculap | BC177R | JAMESON preparation scissors, bent, fine model, blunt/blunt, 150 mm (6") |
| Silicone vessel loop tie | SERAG WIESSNER | SL26 | silicone vessel loop tie 2,5 mm red |
| Spraque Dawley rat | Janvier Labs | RN-SD-M | Spraque Dawley rat |
| Steel plate | Maschinenbau Feld GmbH | C010206 | Galvanized sheet plate, 40 x 50 cm, thickness 4.0 mm |
| Yasargil clip | Aesculap | FE795K | YASARGIL Aneurysm Clip System Phynox Temporary (Standard) Clip |
| Yasargil clip applicator | Aesculap | FE558K | YASARGIL Aneurysm Clip Applicator Phynox (Standard) |
References
- Carden, D. L., Granger, D. N. Pathophysiology of ischemia-reperfusion injury. J Pathol. 190 (3), 255-266 (2000).
- Balkwill, F., Mantovani, A. Inflammation and cancer: Back to Virchow. Lancet. 357 (9255), 539-545 (2001).
- Cruz, R. J., Garrido, A. G., Ribeiro, C. M., Harada, T., Rocha-E-Silva, M. Regional blood flow distribution and oxygen metabolism during mesenteric ischemia and congestion. J Surg Res. 161 (1), 54-61 (2010).
- Leng, G. C., Davis, M., Baker, D. Bypass surgery for chronic lower limb ischemia. Cochrane Database Syst Rev. 3, Cd002000 (2000).
- Droc, I., Calinescu, F. B., Droc, G., Blaj, C., Dammrau, R. Aortic stenting. Minim Invasive Ther Allied Technol. 24 (5), 296-304 (2015).
- Le Gall, A., et al. Veno-arterial-ecmo in the intensive care unit: From technical aspects to clinical practice. Anaesth Crit Care Pain Med. 37 (3), 259-268 (2018).
- Napp, L. C., Kühn, C., Bauersachs, J. ECMO in cardiac arrest and cardiogenic. Herz. 42 (1), 27-44 (2017).
- Sousa Da Silva, R. X., Weber, A., Dutkowski, P., Clavien, P. A. Machine perfusion in liver transplantation. Hepatology. 76 (5), 1531-1549 (2022).
- Sen Gupta, A. Bio-inspired nanomedicine strategies for artificial blood components. Wiley Interdiscip Rev Nanomed Nanobiotechnol. 9 (6), 1464 (2017).
- Lu, D., et al. Intramuscular microvascular flow sensing for flap monitoring in a porcine model of arterial and venous occlusion. J Reconstr Microsurg. 39 (3), 231-237 (2023).
- Nguyen, G. K., et al. Novel biomarkers of arterial and venous ischemia in microvascular flaps. PLoS One. 8 (8), e71628 (2013).
- Redlin, M., et al. How near-infrared spectroscopy differentiates between lower body ischemia due to arterial occlusion versus venous outflow obstruction. Ann Thorac Surg. 91 (4), 1274-1276 (2011).
- Studier-Fischer, A., et al. Endotracheal intubation via tracheotomy and subsequent thoracotomy in rats for non-survival applications. J Vis Exp. (205), e66684 (2024).
- Nickel, F., et al. Optimization of anastomotic technique and gastric conduit perfusion with hyperspectral imaging and machine learning in an experimental model for minimally invasive esophagectomy. Eur J Surg Oncol. , 106908 (2023).
- Barberio, M., et al. Quantitative fluorescence angiography versus hyperspectral imaging to assess bowel ischemia: A comparative study in enhanced reality. Surgery. 168 (1), 178-184 (2020).
- Doukas, P., et al. Onset of adverse abdominal events due to intestinal ischemia-reperfusion injury after aortic cross-clamping is associated with elevated hsp70 serum levels in the early postoperative phase. Int J Mol Sci. 23 (23), 15063 (2022).
- Mine, Y., et al. Heat shock protein 70 messenger RNA in rat leukocytes elevates after severe intestinal ischemia-reperfusion. J Surg Res. 242, 342-348 (2019).
- Criqui, M. H., et al. Lower extremity peripheral artery disease: Contemporary epidemiology, management gaps, and future directions: A scientific statement from the American Heart Association. Circulation. 144 (9), e171-e191 (2021).
- Seidlitz, S., et al. Robust deep learning-based semantic organ segmentation in hyperspectral images. Med Image Anal. 80, 102488 (2022).
- Studier-Fischer, A., et al. Icg-augmented hyperspectral imaging for visualization of intestinal perfusion compared to conventional icg fluorescence imaging: An experimental study. Int J Surg. 109 (12), 3883-3895 (2023).
- Studier-Fischer, A., et al. Heiporspectral - the heidelberg porcine hyperspectral imaging dataset of 20 physiological organs. Scientific Data. 10 (1), 414 (2023).
- Studier-Fischer, A., et al. Spectral organ fingerprints for machine learning-based intraoperative tissue classification with hyperspectral imaging in a porcine model. Sci Rep. 12 (1), 11028 (2022).
- Mallick, I. H., Yang, W., Winslet, M. C., Seifalian, A. M. Ischemia-reperfusion injury of the intestine and protective strategies against injury. Dig Dis Sci. 49 (9), 1359-1377 (2004).
- Malekinejad, Z., et al. Prazosin treatment protects brain and heart by diminishing oxidative stress and apoptotic pathways after renal ischemia-reperfusion. Drug Res (Stuttg). 72 (6), 336-342 (2022).
- Feldman, Z. M., et al. Inferior mesenteric artery revascularization can supplement salvage of mesenteric ischemia. J Vasc Surg Cases Innov Tech. 9 (3), 101041 (2023).
- Munley, J. A., et al. Chronic mesenteric ischemia-induced intestinal dysbiosis resolved after revascularization. J Vasc Surg Cases Innov Tech. 9 (2), 101084 (2023).
- Lejay, A., et al. Ischemia reperfusion injury, ischemic conditioning and diabetes mellitus. J Mol Cell Cardiol. 91, 11-22 (2016).
- Huang, D., et al. Macrovascular complications in patients with diabetes and prediabetes. Biomed Res Int. 2017, 7839101 (2017).
- Liu, A., et al. Hmgb1 in the ischemic and non-ischemic liver after selective warm ischemia/reperfusion in rats. Histochem Cell Biol. 135 (5), 443-452 (2011).
- Koc, S., Dogan, H. O., Karatas, O., Erdogan, M. M., Polat, V. Mitochondrial homeostasis and mast cells in experimental hepatic ischemia-reperfusion injury of rats. Turk J Gastroenterol. 33 (9), 777-784 (2022).
- Chu, M. J., Vather, R., Hickey, A. J., Phillips, A. R., Bartlett, A. S. Impact of ischaemic preconditioning on experimental steatotic livers following hepatic ischemia-reperfusion injury: A systematic review. HPB (Oxford). 17 (1), 1-10 (2015).
- Chang, M. W., et al. Sitagliptin protects rat kidneys from acute ischemia-reperfusion injury via upregulation of GLP-1 and GLP-1 receptors. Acta Pharmacol Sin. 36 (1), 119-130 (2015).
- Boys, J. A., Toledo, A. H., Anaya-Prado, R., Lopez-Neblina, F., Toledo-Pereyra, L. H. Effects of dantrolene on ischemia-reperfusion injury in animal models: A review of outcomes in heart, brain, liver, and kidney. J. Investig Med. 58 (7), 875-882 (2010).
- Orihashi, K. Mesenteric ischemia in acute aortic dissection. Surg Today. 46 (5), 509-516 (2016).
- Byard, R. W. Acute mesenteric ischemia and unexpected death. J Forensic Leg Med. 19 (4), 185-190 (2012).
- Łagosz, P., Sokolski, M., Biegus, J., Tycinska, A., Zymlinski, R. Elevated intra-abdominal pressure: A review of current knowledge. World J Clin Cases. 10 (10), 3005-3013 (2022).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved